

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Minimally invasive surgery (MIS) has inevitably entered into our practice. Laparoscopic surgery in endometrial cancer (EC) treatment has become increasingly common for 15 years. Surgery is a curative treatment for the majority of patients with EC. Laparoscopic surgery in early-stage EC is an effective and safe approach resulting in similar oncologic outcomes compared to laparotomy (LT) [123]. Many laparoscopic studies in this regard were performed with a relatively small number of patients, short median follow-up and in patients with early stage EC. However, EC is a disease with several histopathologic subtypes and different tumor biology and thus having different clinical outcomes. New risk groups were defined by the European Society for Medical Oncology (ESMO)-European Society of Gynaecological Oncology (ESGO)-European SocieTy for Radiotherapy & Oncology (ESTRO) consensus in 2016 as a guide for adjuvant therapy use [4]. Lymphovascular invasion is also assessed in this novel risk classification because of its prognostic importance indicated in the recent studies [56]. In that classification, a total of 4 groups are formed by dividing the intermediate group into intermediate and high-intermediate. There are limited data regarding the feasibility and safety of laparoscopic management of EC with intermediate and high-risk factors such as advanced stage and type 2 EC.
In this study, we aimed to evaluate long-term oncologic outcomes in patients with low, intermediate, and high-risk EC treated by laparoscopic surgery and to compare the surgical and long-term survival data in LT cases at the same time. To our knowledge, there is no study evaluating laparoscopic surgery considering the risk classification of EC in the literature.
MATERIALS AND METHODS
The medical records of the patients with EC, who underwent surgery and were followed in the department of gynecologic oncology, were reviewed between the January 2005 and 2016. We identified 801 patients with EC and these patients were classified as group 1, who underwent LT (n=515), and group 2, who underwent laparoscopy (LS) (n=286). Informed consent was obtained from all patients before surgery. All patients diagnosed with EC based on endometrial biopsy were examined through transvaginal ultrasonography and chest X-ray in accordance with our clinical approach. The presence of a distant metastasis was excluded via computed tomography in the high-risk group. The main exclusion criteria to perform a laparoscopic surgery were severe cardiopulmonary disease, a contraindication for prolonged Trendelenburg position, and large uterus that could not be removed vaginally intact. Age, high body mass index (BMI), and prior pelvic surgery were not the exclusion criteria for LS. All EC patients were evaluated with an intraoperative frozen section according to histopathologic type, grade, and depth of myometrial invasion. An algorithm was followed for EC surgery in accordance with the Mayo clinic surgical algorithm for EC [78]. Totally hysterectomy and bilateral salpingo-oophorectomy were performed on the patients with endometrioid adenocarcinoma, stage 1a, International Federation of Gynecology and Obstetrics (FIGO) grade 1 and 2 tumors (low-risk factors), tumor diameter of <2 cm by LT or LS whereas pelvic lymphadenectomy (PLND) was performed on the patients with tumor diameter >2 cm. Pelvic-paraaortic lymphadenectomy (PPALND)±omentectomy (for serous or mixed type carcinomas) was performed in cases with grade 3, more than 50% myometrial invasion, type 2 histopathology, and higher stages than stage 1a. The operations were performed by the same gynecologic oncology surgical team (V.M.A., G.A.B., G.U.K.).
The demographic parameters were age, BMI, nulliparity, and the history of infertility. Surgical and treatment parameters were the type of surgery, conversion rate, the duration of surgery (from skin incision to skin closure, except the frozen section time), estimated blood loss, decrease in hemoglobin (Hb) level, postoperative hospitalization time (day), intraoperative complications (bleeding was defined as a blood loss exceeding 1,000 mL or requiring blood transfusion), postoperative complications, and adjuvant therapy modalities. Clinical and pathological variables were stage, grade, histopathologic type, myometrial invasion (as <50% and ≥50%), lymph nodes involvement, lymphovascular space invasion (LVSI), the number of lymph nodes yielded, comorbidities, and survival outcomes. Overall survival (OS) and disease-free survival (DFS) were assessed. The surgical stage was determined considering histopathologic results according to FIGO 2009 guidelines. All patients received antibiotic prophylaxis preoperatively and thromboprophylaxis during the hospitalization.
Risk classification was done based on ESMO-ESGO-ESTRO consensus report [4]. Patients with grade 1 or 2 endometrioid, myometrial invasion less than 50%, stage 1, and LVSI negative were classified as low risk; patients with stage 2, 3, 4 endometrioid tumors, grade 3 endometrioid and myometrial invasion more than 50%, regardless of LVSI and type 2 tumors were classified as high risk; patients with stage 1 endometrioid, grade 1–2, ≥50% myometrial invasion, and LVSI negative were classified as intermediate risk; and patients with stage 1 endometrioid, grade 3, <50% myometrial invasion regardless of LSVI or stage 1 endometrioid, grade 1–2, LVSI positive, regardless of myometrial invasion were classified as high-intermediate risk group (model 1). High-intermediate and high-risk group were combined and formed as a new risk group (model 2). Thus, the groups with a high risk of recurrence and death were evaluated together. The requirement of adjuvant therapy was considered for the risk group stratification. Therefore, adjuvant radiotherapy (RT) or chemotherapy (CT) were suggested to the intermediate and high-risk patients. The adjuvant therapy order was individualized according to the characteristics of the patients and pathology. RT was administered in the form of brachytherapy and/or external pelvic RT. CT that consisted of a platin-based regimen for 6 cycles was given to appropriate patients.
Survival analysis was completed on 763 patients with known outcomes. OS was defined as the time (months) between the date of surgery/diagnosis and the date of death or last follow-up. DFS was defined as the time (months) from surgery to the first evidence of recurrent disease or death. Patients known to be alive or lost in the follow-up at the time of analysis were censored at their last follow-up.
The variables were presented as mean±standard deviation, median or number (%). The variables were tested to determine whether or not they were normally distributed by using visual (histograms, probability plots) and analytical methods (Shapiro-Wilk's test). Independent t-tests and χ2 test were used for comparisons between the groups. The effect of clinical variables, histopathologic subtypes and risk groups on OS and DFS of the patients were analyzed using the Kaplan-Meier method. Differences in the survival curves were calculated using the log-rank test. The Cox proportional hazard model was used to assess the significance of multiple variables. Data were analyzed using the SPSS software version 20.0 (IBM Corp., Armonk, NY, USA).
RESULTS
The laparoscopic group consisted of 286 patients and the LT group consisted of 515 patients. The demographic data and the comparison of the variables are presented in Table 1. The mean age was 58.1±10.7 years and 56.0±11.1 years in the LT group and in the LS group, respectively (p=0.011). BMI was similar in both of the groups (p=0.234). There was morbid obesity (BMI>40kg/m2) in 25% of the LS group and 30% of the LT group. Approximately 15% of patients had an infertility history for both groups.
Table 1
Demographics and descriptive variables between the study groups

The clinical and pathological characteristics and risk classification of the groups are summarized in Table 2. Comorbidity was similar with high percent in both groups (45% of patients). Type 2 EC rate was 17% in the LT group and 14.8% in the LS group (p=0.326). The details of treatment and surgical procedures and operative outcomes are shown in Table 3. In eleven patients, the surgery technique was changed to LT from LS due to surgical obligations or complications (3.7%). Laparoscopic PLND was performed for 88 patients and PPALND was performed for 48 patients. Laparoscopic lymphadenectomies had a longer operation time than LT (119 vs. 141 minutes for hysterectomy + PLND and 142 vs. 187 minutes for hysterectomy + PPALND). Estimated blood loss and decrease in Hb levels were significantly lower in the LS group than those in the LT group (p≤0.001 and 0.026, respectively). Postoperative hospitalization time was lower in LS than LT (p<0.001). Moreover, not only postoperative complication rate but also intraoperative complication rate was lower in LS than LT (p<0.001 and 0.024, respectively). There were a total of 5 major vessel injuries, 4 of them in laparoscopic surgery (one deep epigastric artery, 2 common iliac vein and one vena cava inferior). The main postoperative complication was wound infection in the LT group (7.5%). Secondary cytoreduction was performed in 19 patients in the LT group (3.7%) and in 2 patients in the LS group (p=0.014). There was no difference between the groups according to lymph nodes yield (p=0.813). Adjuvant therapy was given to 50% of patients in the LT group and 25% of patients in the LS group (p<0.001). The median follow-up time was 46 months in the LT group and 32 months in the LS group. There was a tumor recurrence in 34% of the LT group and 15% of the LS group. Five-year survival rate was 98% for the LS group and 93% for the LT group.
Table 2
Comparison of the clinical and pathological features between the study groups

Table 3
Features of treatment and operative variables according to the groups

Data are shown as number (%) not otherwise specified.
BPLND, bilateral pelvic lymphadenectomy; BPPALND, bilateral pelvic-paraaortic lymphadenectomy; BSO, bilateral salpingo-oophorectomy; CT, chemotherapy; Hb, hemoglobin; LS, laparoscopy; LT, laparotomy; Omen, omentectomy; PALN, paraaortic lymph node; RT, radiotherapy; SD, standard deviation; TAH, total abdominal hysterectomy; TLH, total laparoscopic hysterectomy.
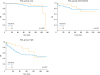
The mean overall and DFS based on the risk groups and prognostic factors such as stage, grade, myometrial invasion, LVSI, and histopathological type are demonstrated in Table 4. There was no difference between the groups in terms of DFS and OS in the risk groups of model 1, whereas there were significant differences regarding OS and DFS in high-risk groups on the model 2. The patients with high risk in the LS group had improved OS and DFS outcomes compared to the LT group (p=0.007 and 0.002, respectively). The patients with advanced stage disease in the laparoscopy group had an advantage for DFS (p=0.048). OS was similar for low and intermediate risk between the groups, but it was higher in the laparoscopy group than in the laparotomy group for high-risk patients (Fig. 1).
Table 4
The results of the survival analysis based on the risk groups and prognostic factors between and within the study groups

Fig. 1
The survival curves between the study groups based on the risk groups. High-risk group refers to the sum of the high-intermediate risk group and the high-risk group.
The results of the regression analysis standardized by age and risk groups revealed that LS or LT as a surgical option was found to be a prognostic risk factor (Table 5). There was an increased risk for death and recurrence in the LT group compared to the LS group (odds ratio [OR]=1.9; 95% confidence interval [CI]=1.2–3.1 for OS; OR=2; 95% CI=1.2–3.3 for DFS) considering the results of covariate analysis. Age, stage, histopathological type, and operation type were determined as independent prognostic factors in multivariate analysis for both of DFS and OS (Table 6).
Table 5
Results of the co-variate analysis
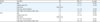
Table 6
Studies of MIS management of high-risk histopathological type EC

| Author-cohort of study | Year | Value | Median follow-up (mo) | PFS | p-value | OS | p-value | |||
|---|---|---|---|---|---|---|---|---|---|---|
| LT | MIS | LT | MIS | LT | MIS | |||||
| Fader et al. [14] | 2012 | 191 | 66 LS (125 robotic assisted LS) | 44 | 81.5 (early stage) | 83.6 (early stage) | 0.588 | 85.5 (early stage) | 84.1 (early stage) | 0.725 |
| (Grade 3+type 2 EC) | 59.5 (advanced stage for 3 yr) | 57.4 (advanced stage for 3 yr) | 0.341 | 65.2 (advanced stage for 3 yr) | 63.8 (advanced stage for 3 yr) | 0.424 | ||||
| Fader et al. [15] | 2016 | 246 | 507 | 60 | 60.5 | 58.8 | 0.745 | 66.7 | 65 | 0.737 |
| (Grade 3+type 2 EC) | ||||||||||
| Favero et al. [16] | 2016 | 36 | 53 LS | 38/47 | 51 (DFS 5 yr) | 58 (DFS 5 yr) | 0.153 | 78 (5 yr) | 86 (5 yr) | 0.312 |
| (Type 2 EC) | ||||||||||
| Koskas et al. [17] | 2016 | 114 | 93 LS (21 robotic assisted LS) | 49 | 62 (DFS 5 yr) | 60 (DFS 5 yr) | 0.71 | 72 (5 yr) | 66 (5 yr) | 0.66 |
| (High-risk histology) | ||||||||||
| Current study* | 181 | 63 LS | 46/32 | 65 (DFS 5 yr) | 74 (DFS 5 yr) | 0.002 | 70 (5 yr) | 79 (5 yr) | 0.007 | |
DISCUSSION
The current retrospective cohort study conducted in a single tertiary reference center in the south of Turkey aimed to evaluate the efficiency and reliability of the laparoscopic approach in different risk groups of ECs. In this study, we showed that laparoscopic surgery was as effective and safe as abdominal approach for the treatment of EC. By comparing the operative results between the LS and LT groups that had similar demographic characteristics, a significant superiority was found in the LS cohort in terms of short-term results such as complications, blood loss, and the length of hospital stay in accordance with the literature [291011]. The benefits of the laparoscopic surgery may be particularly marked in women with obesity and comorbidity. In our laparoscopic cohort, there was a higher rate of obese women (twenty-five percent of the LS group had morbid obesity) and approximately half of the patients had comorbidity. Laparoscopic surgery can substantially reduce the rate of postoperative complications compared to LT surgery in such cases [12]. The most common postoperative complication was wound site infection in our cohort.
Most of studies on the laparoscopic management of the EC were performed on the low-risk EC cohort such as stage 1. A meta-analysis including 8 randomized controlled trials showed that LS was associated with similar OS and DFS for early stage endometrioid adenocarcinoma [13]. Efficacy and safety of LS in terms of survival outcomes in early stage EC is at least controversial. The results of LAP2 survival outcomes [1] and meta-analysis of randomized controlled trials [39] highlight the importance of LS in the management of early stage EC. Similarly, we demonstrated that there was no significant difference between the groups in terms of OS and DFS in the low-risk patients. Furthermore, LS has similar survival outcomes to those of LT not only in early stage but also in low-risk patients.
For intermediate risk group, there is no study performed on intermediate group alone in the literature. This group mainly consists of stage 1b patients. In the LAP2 study [1], stage 1b accounted for 12% of LT group and also LS group (n=204). Our laparoscopic cohort consisted of patients with stage 1b at similar rate (15%; n=45). There was no difference between the groups in terms of DFS and OS in both intermediate and high-intermediate groups in our study. In the last guide [4], MIS is recommended in the low and intermediate risk EC (level of evidence 1, the strength of recommendation: A). Even in this groups of patients, long-term survival analysis should be further supported by randomized controlled studies.
There is a lack of data on the laparoscopic management of high-risk patients. According to our literature review, 4 recent studies have investigated laparoscopic management of patients with grade 3 and type 2 EC [14151617]. In 2012, a multicenter retrospective study, which is the first on laparoscopic management of high grade and type 2 endometrial carcinomas (n=191), concluded that high-risk histopathologic types were not a contraindication for MIS [14]. The post-hoc analysis of the LAP2 including early stage patients with grade 3 endometrioid and type 2 (n=507) showed that patients with high-grade uterine cancers managed by LS had similar rates of recurrence and survival to those managed by LT [15]. In this study, type 2 cancer recurred 2 times more than grade 3 endometrioid cancer. Favero et al. [16] studied the feasibility, operative outcomes and oncologic safety of laparoscopic surgery in patients with type 2 EC (n=53). They concluded that LS was associated with better oncologic outcomes than LT with no statistical significance [16]. Indeed, with increasing number of patients, a statistical significance could be achieved. And the last study on high-risk EC by Koskas et al. [17] compared 93 laparoscopic and 21 robotic surgeries with 114 laparotomic surgery. In accordance with other studies, DFS and OS were not different between the surgical groups [17]. Survival outcomes of the retrospective studies of MIS management of high-risk histopathological type EC were shown in the Table 6. These 4 trials studied the patients with high-risk histopathology. We evaluated not only patients with type 2 cancer and grade 3 endometrioid adenocarcinoma but also patients with the high-risk which was also the subject of other risk factors such as advanced stage, myometrial invasion, and LVSI. Despite the similar type 2 proportions between the groups (18% vs. 15%) in our cohort, higher superiority of LS in survival analyses occurred for type 2 cancer. Type 2 and grade 3 endometrioid cancer constituted less than 20 percent of all ECs and even in the early stage, the prospects for distant metastasis have increased [18]. The patients with type 2 EC are usually older than those with type 1 cancer and the probability of systemic disease is increased. Adjuvant therapy is frequently recommended in this high-risk group with a high likelihood of recurrence. Therefore, it is important that surgical morbidity is less than in LS and adjuvant therapy can be started immediately. Although there was no difference in survival analysis between the groups on the risk groups. As a result of our study, LS seems to be superior to LT in terms of survival outcomes in multivariate analysis. However, that result should be interpreted carefully because of the retrospective structure and bias in group selection. It is clear that we need more effective and reliable data on the laparoscopic management of high-risk patients.
Our study includes all negative aspects of retrospective study design. Another limitation of our study is that we cannot give the initiation time of adjuvant treatment. However, the main strength of our study was the survival analysis according to risk group classifications which were based on the most important factors (stage, grade, myometrial invasion, LVSI, and histopathology) affecting the prognosis. In this way, we attempted to minimize the effect of non-randomized and biased patient's selection on the survival analysis. Additionally, we had a relatively large cohort of the groups for a single center and longer follow-up period.
The results of our study suggest that LS can be used effectively and safely in patients with intermediate and high-risk EC. Long-term survival analysis should be supported by randomized controlled studies to demonstrate that LS may be an acceptable alternative to LT for EC patients with high-risk.
 XML Download
XML Download