

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Endometrial cancer is the sixth most common cancer among women worldwide along with cervical and ovarian cancer [1]. Changes in childbearing methods, use of hormone-replacement therapy, aging population, and reduced physical activity are associated with increased endometrial cancer incidence [23]. In South Korea, endometrial cancer also has been on the rise, and it was estimated to account for 2.1% (n=2,214) of all newly-diagnosed female cancers, in 2014 (n=104,175) [4]. Endometrial cancer has a relatively good prognosis. Compared to 1993–1995, the 5-year survival rate has gradually increased from 81.5% to 84.6%, during 2010–2014 in South Korea [5].
Psychological problems can affect treatment compliance and can increase cancer patient mortality [6]. The Korean study using the national cancer registry database (n=302,844) showed that depression and anxiety were diagnosed in 2.45% (n=7,415) and in 3.37% (n=10,217) among total cancer patients [7]. Previous studies have shown that cancer survivors have an increased risk of depression, anxiety, and stress disorders within the first year following a cancer diagnosis in patients with breast and ovarian cancer [89]. Because adequate clinical support for these mental disorders can improve the clinical outcomes including the quality of life, it is important to understand the mental health of the cancer survivors before, during and after treatment [10].
Endometrial cancer can also lead to emotional distress due to the associated invasive surgical treatments, such as radical hysterectomy [11]. However, there has been a lack of study of endometrial cancer survivors treated for mental disorders in South Korea. Although a Korean study reported that the incidence of depression was 26.4% in gynecologic cancer [12], the results were limited because of its small sample size with a cross-sectional design. In this study, we analyzed nationwide longitudinal data on mental disorder incidence among endometrial cancer survivors by using the national South Korean claims database.
MATERIALS AND METHODS
The Republic of Korea has a public medical insurance system called the National Health Insurance system. The data generated by the Health Insurance Review and Assessment Service (HIRA) in South Korea are based on payment claims regarding patient visits or inpatient admissions to medical institutions and include patient demographics and clinical information based on prescriptions [13]. We analyzed retrospectively the nationwide cohort based on the HIRA claims data includes patients diagnosed with endometrial cancer from January 1, 2010 to December 31, 2014. The Institutional Review Board (IRB) of the Ajou University Hospital approved this study (IRB No. AJIRB-MED-EXP-16-494).
The study population consisted of patients diagnosed with endometrial cancer (category C54) according to the Korean Classification of Disease, sixth edition, a version of the International Classification of Disease 10 (ICD-10) modified for the Korean health care system. Due to using the pathological staging system for endometrial cancer diagnosis, there was no difference in the time interval between diagnosis and hysterectomy. Also, we confirmed subjects underwent hysterectomy (procedure codes R414 and R415). The first diagnosis of a mental disorder was identified using claims data from inpatient and outpatient first visits. To confirm the existence of mental disorders among the endometrial cancer survivors, we used ICD-10 as the principal diagnosis. Based on previous studies, we selected the following mental disorders: depression (F32, F33), anxiety (F40, F41), and stress reaction/adjustment disorders (F43) [8].
Since we focused on mental health issues near hysterectomy, we excluded individuals who had psychiatric disorders for more than 1 year before surgery. Descriptive statistics were employed to estimate the frequency of mental disorders based on their first day of diagnosis. We also analyzed the disease characteristics according to age and the nature of the disease. The total number of prescriptions for treatment follow-up has been confirmed for survivors of endometrial cancer from the first diagnosis through December 31, 2014, to the last hospital visit date. To analyze patient preferences regarding the treating medical institution and departments, we classified hospitals into 3 categories (general hospital, hospital, and private clinic) with specific medical department categories. A comparison between or among the groups was performed using the χ2 test. Two-sided p-values less than 0.05 were considered statistically significant. All statistical analyses were performed with R 3.0.2 (R Foundation, Vienna, Austria).
RESULTS
A total of 8,155 endometrial cancer survivors who were diagnosed and received a hysterectomy between 2010 and 2014 in South Korea, were identified. The median age at diagnosis for patients with endometrial cancer was 54 years. The frequency of mental disorders among endometrial cancer survivors is shown in Table 1. In total, 567 (7.0%) endometrial cancer survivors with mental disorder first visited a hospital from 1 year before hysterectomy to later. These mental disorder groups included 249 cancer survivors with depression (43.9%), 248 with anxiety (43.7%), and 70 with stress reaction/adjustment disorders (12.3%). The higher the elderly, the higher the diagnosis rate of mental disorders and the more anxiety. The total number of prescriptions for mental disorder was 6,034. The prescription for depression was the most commonly prescribed (63.0%, n=3,799), followed by anxiety treatment (29.4%, n=1,771) (Table 2).
Table 1
The frequency of mental disorders in endometrium cancer survivors (n=8,155)

![]()
Table 2
The distribution of claim data for mental disorder among endometrium cancer survivors (n=6,034)

![]()
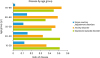
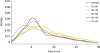
Disease incidence ratios by age group are reported in Fig. 1. Depression incidence rates were relatively high in young endometrial cancer survivors. In contrast, the ratio of anxiety was higher in older age groups. Among the survivors of endometrial cancer, 177 were diagnosed with the mental disorder before surgery and 390 were diagnosed after surgery. Anxiety was the most common disease in the preoperative period (45.8%, n=81). Depression was most frequently observed in the postoperative period (44.9%, n=175). The overall frequency of mental disorders started to increase 12 months before hysterectomy, changing sharply before and after surgery. There was a slight difference in the incidence of mental disorder, but most of the peak was reached during the first 2 months after hysterectomy (Fig. 2). Depression frequency reached a peak 2 months later, and anxiety peaked just before hysterectomy. The highest rate of increase after hysterectomy was noted for stress reaction/adjustment disorders. There was a difference in the peak time among age groups. For elderly cancer survivors, over 70 years old, the highest incidence of mental disorders occurred before hysterectomy, while for younger cancer survivors, under 40 years old, the highest mental disorder incidence rate presented after hysterectomy (Fig. 3).
 | Fig. 2The frequency density of mental disorders in endometrial cancer survivors (The area under density curve for each mental disorder is 1).
|
 | Fig. 3The frequency density of mental disorders by age group in endometrial cancer survivors (The area under density curve for each age group is 1).
|
The mental disorder claims data varied according to the different medical departments and types of medical institutions. From a total of 6,034 prescriptions, over 80% (n=5,362) claims for mental disorder treatment were in psychiatric medical departments, whereas family medicine hospital visit accounted for only 1.2% (n=72). Private clinics accounted for 65.0% (n=3,924), whereas general hospitals accounted for 29.7% (n=1,790). Notably, the number of claims in general hospitals was over 30% (n=1,647).
The frequencies of mental disorders according to age and adjuvant therapies was summarized in Table 3. There were no significant differences in mental disorders between patients with an age of ≥54 and <54 years old (p=0.653). Adjuvant therapies was not a significant factor affecting the frequency of mental disorders (p=0.287).
Table 3
The frequency of mental disorders according to age and adjuvant therapies

![]()
DISCUSSION
Hysterectomy for endometrial cancer treatment can induce emotional stress, which in turn can affect the prognosis of the disease [14]. The prevalence of mental disorders changed significantly during the different periods of the disease [15]. We analyzed changes in the frequency of mental disorders starting from 1 year before endometrial cancer hysterectomy using nationwide claims data. From a group of 8,155 endometrial cancer survivors, we identified 567 patients with mental disorders (Table 1). The occurrence of depression (43.9%, n=249) and anxiety (43.7%, n=248) was similar during the initial diagnosis. However, based on the total number of prescriptions, depression was the most common mental disorder among endometrial cancer survivors (63.0%; n=3,799). Compared to the rates of newly-diagnosed mental disorders, it could be inferred that the frequency with which cancer survivors with depression visit medical institutions is relatively high and depression was a relatively long-lasting trend. Over time, patients with chronic anxiety could have a trend to present with depression [16].
Most endometrial cancer survivors experienced psychological distress resulting from treatment fear; treatment-related side effects, such as lymphedema, urological symptoms, and sexual problems; and cancer recurrence or progression [17]. The underlying causes of distress after hysterectomy might be associated with patients' reactions to anesthetics and painkillers, and the hormonal imbalance caused following ovary removal [18]. Moreover, the fear of surgical complications together with the impending loss of fertility could lead to a great emotional burden for the patients [19]. Generally, the peak of mental disorder incidence was noted within 2 months after a hysterectomy and decreased after that (Fig. 2). Being aware of these recovery periods after hysterectomy might help cancer survivors avoid further frustration due to cancer-related distress. Moreover, if mental evaluations are carried out during that period, patients with a high risk of mental illness can easily be screened and identified. If these patients receive immediate psychiatric care, it might aid in improving their quality of life.
Every mental disorder showed a different time-dependent pattern of manifestation. Before the hysterectomy, anxiety incidence was at its peak and decreased after the surgery (Fig. 2). Additionally, depression incidence was peaked after hysterectomy and the frequency was confirmed as persistent until 1 year after hysterectomy. It may have been associated with treatment-induced symptoms [20]. Previous studies also showed the highest frequency of visits in the first year after diagnosis [21]. The frequency of stress/adjustment disorders increased rapidly after hysterectomy. The emotional distress that occurs close to hysterectomy is further affected by cortisol variability, which is suggestive of higher hypothalamic-pituitary-adrenal (HPA) axis activation [2223]. These alternations in HPA axis functioning have been associated with mental disorders. In a previous study of cancer survivors, stress reaction/adjustment disorder showed the highest rate of increase after cancer diagnosis [9]. This information is useful for providing the right intervention, based on the time-dependent patterns of each mental disorder.
In the analysis of the mental disorder prevalence according to age, mental disorder frequency increased before hysterectomy, and reached its peak around the time of surgery, with a decline after that (Fig. 3). Patients in the 70–99 years age group had the highest mental disorder incidence right before hysterectomy, while the younger age group (10–39 years) showed the highest mental disorder incidence after hysterectomy. Elderly patients may have a greater fear of surgery in this group because they have the more underlying disease than younger patients [24]. In premenopausal women who have had a hysterectomy that included both ovary removal, both salpingo-oophorectomy may induce premature menopause, fertility loss [25]. This change in hormonal status may affect patients' mood and put them at risk of depression. Some women may also experience vaginal dryness after hysterectomy, which can affect their sexual well-being. Also, depression was more frequent in the younger age group than in the older age group (Fig. 1). On the contrary, the frequency of anxiety disorders was higher in elderly patients. Therefore, different interventions should be considered for each age group in a clinical setting. Particularly, young cancer survivors are required to cope with the problem of returning to work and caring for their children [26].
Our results provide information about the psychological status of endometrial cancer survivors during their cancer journey. Because endometrial cancer survivors usually have a good prognosis, recognition of psychological symptoms, prompt diagnosis, and appropriate treatment for distress are vital in the management of cancer survivors. The majority of hysterectomies and post-operative management for endometrial cancer took place at a general hospital. However, only about 29.7% of the mental disorder diagnoses were done in a general hospital setting, while over 65.0% were from private clinics. Also, other studies report an increase in private clinic use among cancer survivors compared to the general population [2728]. These results indicate that there are unmet needs for emotional illness management in general hospitals. Therefore, our findings confirm the need for a validated screening tool to detect high-risk groups for mental disorder in general hospitals and a referral system for psycho-oncological care. Moreover, educational information on the mental status of cancer survivors should be provided in private clinics for managing cancer survivors. Especially, emotional disorders have a high rate of visits to psychiatry (88.9%, n=5,362), so preparation of psychiatrists for cancer survivor treatment is important.
In this study, we confirmed that 3.1% (n=249) of endometrial cancer survivors were diagnosed with depressive disorder. On the other hand, only 1.3% (n=354,343) of the general female population reported having a depressive disorder by the National Health Insurance Service result. Similarly, while 3.0% (n=248) of endometrial cancer survivors were diagnosed with anxiety disorder, only 1.2% (n=318,633) were diagnosed in the general female population. These results show that endometrial cancer survivors are more vulnerable to mental illnesses than the general population. However, cancer survivors tended to underestimate and undertreat psychosocial distress [29]. Therefore, the physician needs to monitor the mental status at various stages of the illness in endometrial cancer survivors in addition to the physical condition during the follow-up period [30]. Early intervention, which is important, also should be provided.
We evaluated the impact of age and the type of adjuvant therapies on the risk of mental disorders (Table 3). However, these factors were not significant risk factors in developing mental disorders in our cohort. It may be due to the limited information of public claim data with undetected cancer-related parameters such as cancer stage.
There are a few limitations to this study. First, we examined mental disorder cases using HIRA claims data, which offered only code and demographic information. Clinical data (cancer stage, pathologic type), social data (educational level, marital status), and psychosocial factors were not available. Moreover, patient-related factors, such as disease stage and pathologic type could also be associated with mental disorder prevalence. Second, the disease code was based on claim data in the treatment environment and was not created for the research setting. The diagnostic accuracy of ICD codes for mental disorders is not as high as the diagnostic accuracy obtained from structured clinical interviews using questionnaires. Moreover, the diagnostic codes for the mental disorders may be influenced by the medications, such as antidepressants prescribed for insomnia. However, in South Korea, there was a tendency to refuse treatment with fear of being labeled patients with a mental disorder [31]. Therefore, the diagnoses of mental disorders are very conservative, which can compensate for the potential biases that would have arisen if patients have comorbid psychiatric disorders or symptoms. Lastly, this study was not able to exclude the effect of surgery on mental disorders because our study population was confined to patients with endometrial cancer. The comparison between the groups with benign conditions and endometrial cancer should be performed to adjust the impact of surgery on mental disorders in the other studies.
In conclusion, survivors of endometrial cancer experience mental illness from pre-diagnosis to post-treatment to subjective follow-up. These mental disorders showed different patterns of prevalence depending on age, time of hysterectomy, and disease nature. Timely diagnosis using validated screening tools and early intervention through an effective referral system are essential for the proper management of mental disorders in cancer survivors.
 XML Download
XML Download