

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The effect of air pollution on mortality and the burden of disease increases as air pollution increases, although estimates can vary from region to region. According to the Global Burden of Disease Study, ambient air pollution accounted for 7.5% of deaths globally in 2016 and was the sixth leading contributor to attributable disability-adjusted life years (DALYs) in that year.1 Korea has experienced rapid economic growth in the last century, and the quality of the atmosphere has worsened. Air pollution reduction policies, such as the Special Law on Air Quality in the Seoul metropolitan area, have had limited effect on particulate matter (PM) pollution, and the overall air quality remains poor. Concentrations of PM with aerodynamic diameter less than 10 µm (PM10) have improved over the past decade, reaching the lowest national average of 45 µg/m3 in 2012, and then rebounding to a level of 47 µg/m3 in 2016. However, the concentration of nitrogen dioxide (NO2) has remained relatively constant, with no large changes. The average values of ozone (O3) concentration are continuously increasing.2
Epidemiological studies on the health effects of air pollution have been actively conducted in many countries. In particular, time series studies to examine the short-term effects of air pollution have been conducted worldwide and have yielded relatively consistent results.34 However, cohort studies to assess the long-term effects of air pollution have been primarily conducted in Western countries that have relatively low concentrations of air pollutants. Due to a lack of direct evidence at higher global concentrations, the integrated expose–response (IER) model was developed. The IER combines information on PM-mortality associations from non-outdoor sources, including secondhand smoke, active smoking, and household air pollution,5 and has been used to estimate the disease burden attributable to PM with aerodynamic diameter less than 2.5 µm (PM2.5).1 As the use of IER requires a strict assumption of equal toxicity per unit dose across these non-outdoor sources, cohort studies are needed that reflect the different air pollution concentrations in different regions.6
The health effects of air pollution can vary regionally depending on the composition of pollutants or characteristics of the population at risk. The regional differences in PM2.5 mortality risk estimates can likely be attributed to geographic variation in particle composition or the spatial heterogeneity of constituents,7 as well as differences in the total air pollution mixture.8 Regional differences of topography, which may lead to regional differences of exposure error, can contribute to regional differences in PM risk estimates.9
To accurately understand the impact of air pollution on health in Korea, the results of research performed specifically for Korea are needed. Since the publication of time series research starting in 1999 in Korea,10 many epidemiological studies have been conducted; however, the results of these studies have not been systematically summarized. To accurately assess the impact of air pollution in Korea and to clarify future research directions, systematic sorting of epidemiological studies on air pollution conducted in Korea is required. The aim of the present analysis was to comprehensively review previous epidemiological studies on air pollution and health conducted in Korea to identify future study needs.
LITERATURE SEARCH
We conducted a literature search in PubMed using the search terms (“air pollution”[MeSH Terms] OR (“air”[All Fields] AND “pollution”[All Fields]) OR “air pollution”[All Fields]) AND (“mortality”[Subheading] OR “mortality”[All Fields] OR “mortality”[MeSH Terms]) AND (“Korea”[MeSH Terms] OR “Korea”[All Fields]) and ((“air pollution”[MeSH Terms] OR (“air”[All Fields] AND “pollution”[All Fields]) OR “air pollution” [All Fields]) AND (“epidemiology”[Subheading] OR “epidemiology” [All Fields] OR “morbidity”[All Fields] OR “morbidity” [MeSH Terms]) AND (“Korea”[MeSH Terms] OR “Korea”[All Fields])) NOT (“mortality”[Subheading] OR “mortality” [MeSH Terms]) to find published studies on the associations of air pollution with mortality and morbidity respectively in Korea, between January 1990 and July 2018.
We also searched for health impact assessment studies using the same search engine and the search terms (“number” [All Fields] AND (“death”[MeSH Terms] OR “death”[All Fields] OR “deaths”[All Fields])) OR “burden of disease”[All Fields] OR “health impact assessment”[All Fields] AND “Korea”[All Fields] AND (“air pollution”[All Fields] OR “ambient”[All Fields]).
After reviewing the title and abstract of each article, we selected epidemiological studies that reported associations between exposure to air pollution and mortality or morbidity. We then summarized these articles according to their characteristics and results.
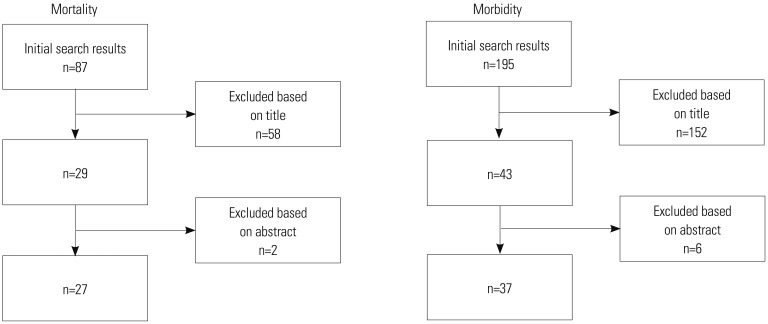
The initial search for mortality and morbidity returned 87 and 195 results, respectively. After excluding articles that did not meet the inclusion criteria (Fig. 1), there remained 27 (Table 1) and 37 studies (Table 2) on mortality and morbidity, respectively. One of the mortality study also reported morbidity results, so a total of 38 studies were included in the present review. The search for health impact analyses returned 22 studies; four articles remained after a review of titles and abstracts.
Air pollution and mortality
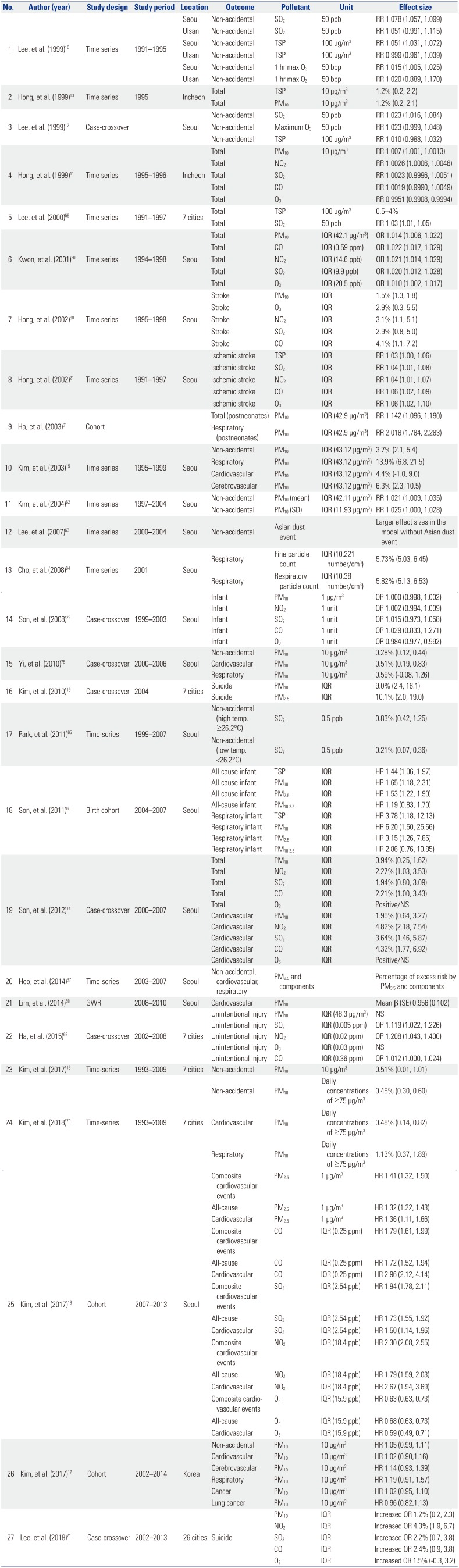
Among the included studies, the earliest reports regarding an association between air pollution and mortality in Korea were published in 1999.10111213 Three of these were time series studies and one was a case-crossover study. Both time series and case-crossover designs are suitable for analysis of acute effects (in days) of short-term exposure to air pollution. One time series analysis was conducted in Seoul and Ulsan. That study reported that the daily variation of ambient concentrations of sulfur dioxide (SO2), total suspended particles (TSP), and O3 in Seoul were significantly associated with increased non-accidental mortality.10 In the same year, the results of reanalysis of Seoul data from the previous time series using a case-crossover approach, in which each participant became its own control, were reported, showing that only SO2 was significantly associated with non-accidental mortality.12 Another time series study conducted in Incheon showed that, in addition to TSP, a 10-µg/m3 increase in the daily mean concentration of PM10 was also associated with a 1.2% increase in total mortality.13 The remaining study was the first to examine the effects of all five criteria pollutants [PM10, SO2, NO2, carbon monoxide (CO), and O3] on mortality in Seoul. That study reported that the previous day's concentrations of PM10 and NO2 were significantly associated with increased daily mortality [relative risks (RRs) of 1.0007 and 1.0026 for PM10 and NO2, respectively].11
After 1999, most subsequent studies examined the associations between air pollutants and total or non-accidental mortality using time series analysis and a case-crossover design. However, the effect sizes varied according to different studies. For instance, the percent increase in mortality for an interquartile range (IQR) increment in PM10 ranged between 0.9%14 and 3.7%.15 This may be due to different factors of these studies, including the study period and area, and a multi-city study may provide more robust effect size. There were few multi-city studies and even fewer reported associations with total mortality. The most recent such study stated that a 10-µg/m3 increase in daily ambient PM10 was associated with a 0.51% increase in mortality.16
The effects of air pollution are not only acute but also chronic, and long-term exposure is generally expected to have a much higher effect size than short-term exposure. However, the chronic effect of air pollution has rarely been examined in Korea. In fact, there were only two studies reporting long-term effects of PM exposure on mortality among our search results, one each for PM10 and PM2.5. Kim, et al.17 analyzed a sample cohort of the National Health Insurance Service and reported a marginally significant 5% increase in mortality per a 10-µg/m3 increase in annual PM10 concentration. Another study reported a hazard ratio (HR) of 1.32 for all-cause mortality with an increment of 1 µg/m3 in PM2.5.18 Long-term exposure to other gaseous pollutants was also found to be associated with increased risk of mortality, and CO, SO2, and NO2 showed HRs of 1.72, 1.73, and 1.79 for each IQR increase, respectively.
The effect of air pollution exposure on mortality is cause-specific, and the related cardiovascular and respiratory effects are well known. There have been several reports on cardiovascular and respiratory mortality owing to air pollution in Korea. An interesting cause of death that shows an association with air pollution is suicide. In a case-crossover study conducted using data from seven metropolitan cities in Korea (Seoul, Incheon, Daejeon, Gwangju, Daegu, Busan, and Ulsan), the authors reported that an IQR increase of PM2.5 was associated with a 10.1% increase in the number of suicides.19
Most gaseous air pollutants (SO2, NO2, and CO) showed consistently significant associations with increased mortality. For acute exposure, an IQR increase of SO2, NO2, and CO increased daily mortality about 2%, and an IQR increase in chronic exposure to those three pollutants showed consistent RRs of around 1.7 (Table 1). However, the association between ambient O3 concentration and mortality seems inconclusive. Two studies reported significant positive associations of O3 concentration with total mortality20 and ischemic stroke mortality.21 However, we also found reports of significant negative associations with all-cause,1318 cardiovascular,18 and infant mortality.22
Air pollution and morbidity
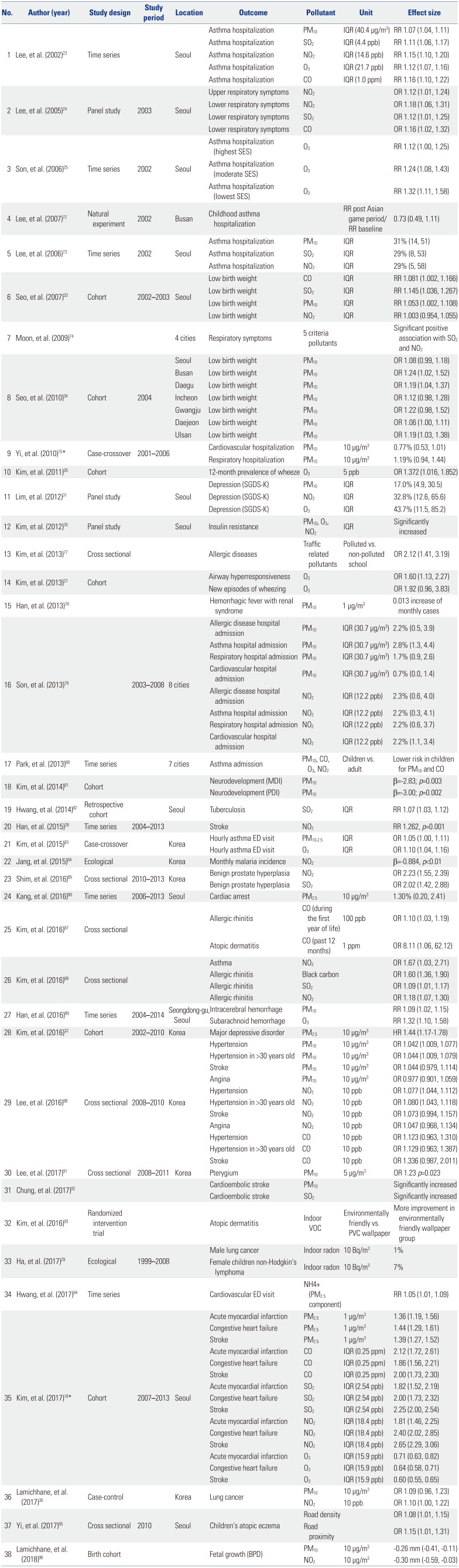
Asthma and respiratory diseases were among the first specific disorders analyzed in Korea. A time series analysis conducted in Seoul reported that an IQR increase in PM10, SO2, NO2, CO, and O3 showed significant RRs for children's asthma hospitalization of 1.07, 1.11, 1.15, 1.16 and 1.12, respectively.23 Another study reported the results of a children's panel for NO2 exposure showing an OR of 1.12 for upper respiratory symptoms and ORs for lower respiratory symptoms of 1.18, 1.12, and 1.16 for increased exposures to NO2, SO2, and CO, respectively.24 O3 was also associated with children's asthma hospitalization, especially in groups with lower socioeconomic status (RR: 1.32, 95% CI: 1.11, 1.58).25 In a cohort study, O3 concentration was associated with a 12-month prevalence of wheeze26 and airway hyperresponsiveness27 in children. Other allergic disorders, such as allergic rhinitis and atopic dermatitis, were also associated with air pollution (Table 2).
Similar to the association between air pollution and cardiovascular mortality, the morbidity of cardiovascular and cerebrovascular diseases, such as stroke, myocardial infarction, and hypertension, were also significantly associated with increased exposure to air pollution. A time series analysis reported that NO2 increased stroke (RR=1.2, p-value=0.001),28 and a cohort study reported that long-term exposure to PM2.5, CO, SO2, and NO2 increased the risk of acute myocardial infarction, congestive heart failure, and stroke (Table 2).18
We found two studies examining the association of air pollution with cancer. In these recent studies, indoor radon concentrations were associated with an increased risk of male lung cancer and non-Hodgkin's lymphoma in girls,29 and conventional air pollutants (PM10 and NO2) were associated with lung cancer with marginal significance.30
Similar to the association of suicide with air pollution, depressive symptoms were also found to be associated with air pollution in Korea. A panel study examining air pollution and depressive symptoms was one of the first to report such an association.31 An association between PM2.5 and major depressive disorder was also found in a community-based urban cohort.32
Health impact assessment
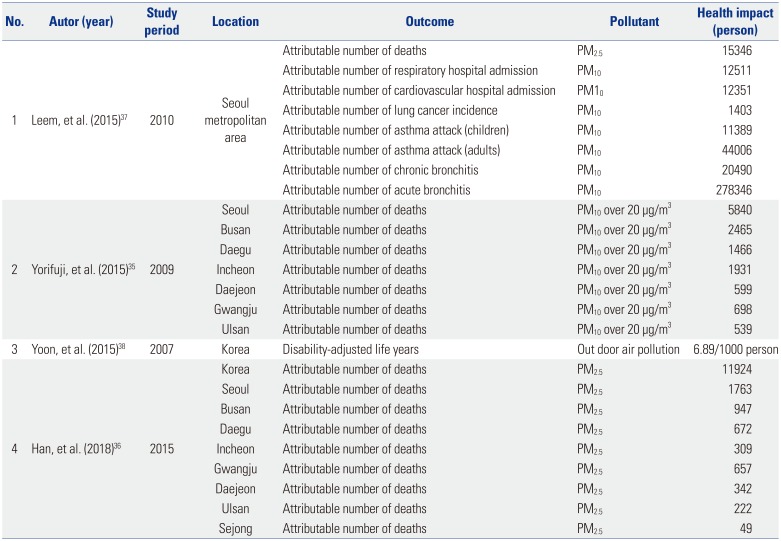
Among four studies (Table 3), two calculated the attributable number of deaths,3536 one calculated the attributable number of deaths and morbidity,37 and a fourth calculated DALYs.38
There were substantial differences in the attributable number of deaths among the study results. For instance, Leem, et al.37 estimated the number of deaths attributable to PM2.5 to be 15346 in the Seoul metropolitan area, whereas Han, et al.36 estimated this number to be 1763. Yorifuji, et al.35 estimated the number of deaths attributable to PM10 over 20 µg/m3 at 5840 in Seoul. These numbers are substantially different, even when considering the differences in study area, study period, and pollutants investigated.
DISCUSSION
Beginning in 1999, many studies have been conducted to elucidate the health effects of air pollution in Korea. These studies have reported associations with mortality (all-cause, respiratory, cerebrovascular, cardiovascular, infant, injury, and suicide) and morbidity (allergic, respiratory, cardiovascular, cerebrovascular, adverse birth outcomes, depression, and cancer). Most studies examined the short-term effects of air pollution using a time series or case-crossover study design; we found only three cohort studies that examined long-term effects. There were four studies that estimated the health impacts of air pollution, and except for one study that reported DALYs, three studies had inconsistent estimations of the attributable number of deaths.
Estimating health impacts is usually conducted later than other research as previously estimated associations between exposure and outcome, or concentration-response function (C-R function) are required.39 Naturally, the estimated health impact depends on the C-R function used. We suspect that differences in the attributable number of deaths estimated in the three studies reviewed here is partly due to the different C-R functions applied by the authors. Specifically, Yorifuji, et al.35 and Leem, et al.37 used C-R functions for mortality derived from epidemiological studies conducted in the United States (U.S.), whereas Han, et al.36 used an IER function developed for the Global Burden of Disease 2010 and 2013. The C-R function derived from U.S. studies only accounted for a relatively low level of PM; thus, it may be inadequate for estimation of health impacts in Korea where exposure to higher concentrations of PM is observed. The IER function was developed by integrating various C-R functions of other exposures, such as tobacco smoke and burning of indoor solid fuel, to fill the gap in exposure range.36 However, it remains uncertain whether the C-R function is comparable to the higher exposure range observed in Korea. Considering this, it is important to produce C-R functions using Korean data to accurately estimate the health impacts of exposure to air pollution.
As mentioned above, the effect of air pollution exposure can be divided into short-term and long-term effects. Typically, short-term effects are examined using time series and case-crossover studies, and long-term effects are investigated in cohort studies. The most recent time series study in Korea reported a 0.51% increase in mortality for each 10-µg/m3 increase in PM10.16 This is comparable to the results of a recent meta-analysis of studies from East Asian cities, including Seoul and Incheon, which reported a 0.47% increase in total mortality for the same amount of increase in PM10.40 Similarly, although we could not find health impact assessment studies regarding air pollutants other than PM, we believe that previous epidemiological studies can provide relatively robust C-R functions for NO2 and SO2 to estimate health impacts.
Previous studies have reported inconsistent associations between O3 exposure and mortality. Some published studies have reported a negative association, and the cause of this negative association has been an intriguing subject for additional analysis. One hypothesis is that the C-R function between O3 concentration and mortality is not linear.41 Time series analyses conducted in Korea and Japan support this hypothesis in short-term associations.4243 However, such non-linearity has not been observed in other studies,4445 and the shape of the C-R function between O3 concentration and acute mortality is still controversial. Nevertheless, studies analyzing the C-R function for long-term exposure of O3 and mortality consistently report no evidence of a threshold.4647 However, these studies may not have accounted for lower concentrations of O3; this may be the reason for not observing a non-linear association, as the reported threshold of non-linear associations tends to be at lower concentrations. The negative association reported in a cohort study conducted by Kim, et al.18 may suggest the existence of a non-linear C-R function between long-term exposure to O3 and mortality because Korea has lower concentrations of O3 than the U.S.;43 however, no analysis has been conducted using Korean data, as far as we know.
Among the two cohort studies on air pollution and mortality, one study examined the long-term health effects of PM2.5 exposure. Although it is a valuable addition to the current knowledge, the results of that study seem inconsistent with previous reports. For instance, Kim, et al.18 reported an HR of 1.32 for all-cause mortality for a 1-µg/m3 increment of PM2.5 in a cohort constructed using the National Health Insurance Service database, and a recent U.S. study analyzing a cohort constructed from a Medicare database reported an HR of 1.073 for a 10-µg/m3 increment of PM2.5.47 Kim, et al.18 suggested possible differences in the effect and composition of PM2.5, genetic characteristics, and range of exposure between these studies, although we find a more than 30-fold greater HR difficult to explain. The largest difference between these two studies was in exposure assessment. Kim, et al.18 linked the concentration measured at a fixed monitoring station to the addresses of participants, whereas Di, et al.47 used a model-based estimation of individual exposure. Another cohort study examined the long-term effect of PM10 exposure.17 Those authors reported similar effects for PM10 exposure, although the association was not statistically significant. However, this latter study applied an exposure assessment strategy, which could alleviate the effect of misclassification caused by participant mobility and exposure measurement at fixed monitoring stations.
Conventionally, air pollution studies use concentrations measured at fixed monitoring stations for exposure, which is an advantage for providing a large amount of data for a wide range of pollutants. However, data linked to study participants' addresses may not reflect individual exposure, especially when the mobility pattern of individuals is not accounted for.48 This limitation may lead to misclassification, which may have substantial implications for the interpretation of results.49 In recent years, advanced sensor and modeling technologies have facilitated individual exposure measurement in air pollution studies with the use of personal sensors and various exposure models based on dispersion models, geographical information, and satellite images.485051 Estimation of exposure using these methods in Korea has been reported recently,52 and these individual exposure estimation methods should be applied in future studies to reduce uncertainty.
In addition to observational studies, there have been many intervention studies on air pollution and its health effects. Recent intervention studies have explored the benefits of exposure reduction using devices, such as an air purifier5354 and facemasks,55 in randomized controlled trials. The strength of intervention studies is two-fold: First, intervention studies may provide more robust evidence regarding the health effects of exposure to air pollution. Second, these trials may provide evidence regarding the effectiveness of personal measures that can be used to reduce the effects of air pollution. However, due to ethical and practical limitations, randomized controlled trials can only be applied to evaluate acute effects of exposure to air pollution. For instance, it may be unfeasible and unethical to design a study in which a portion of study participants are asked to wear facemasks for a long period (e.g., years). Causal modeling is a method that has been proposed to mitigate the shortcomings of observational studies without the need to conduct a randomized trial. This approach includes marginal structure modeling, instrumental variable analysis, and negative exposure control.56 The causal modeling approach provides associations that are free of confounding under certain assumptions, which can be interpreted as causal, similar to the results of a trial. To date, there had been reports on the causal associations of PM2.5, black carbon, and NO2 in various circumstances.5758 Such experimental studies are necessary so as to correctly assess the effects of air pollution on health and to facilitate more effective interventions through which to reduce exposure and to mitigate the health effects of air pollution.
Finally, despite our best efforts to comprehensively summarize the study results regarding the health effects of air pollution exposure in Korea, it is possible that we did not compile a complete list of all relevant research, which should be considered a limitation of the present review.
CONCLUSION
In the present review, we presented epidemiological studies conducted in Korea examining the health effects of exposure to air pollution. For the past 2 decades, there has been a considerable accumulation of knowledge regarding air pollution and health in Korea. However, the present review highlights that additional studies, especially cohort and experimental studies, are needed to provide more robust and accurate evidence that can be used to promote evidence-based policymaking.
 XML Download
XML Download