

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since the first successful resection for gastric cancer by Theodor Billroth at Vienna General Hospital in 1881,1 the treatment of gastric cancer has changed and advanced tremendously. 23 The Department of Surgery, Severance Hospital, Yonsei University College of Medicine, has been at the center of these changes. This institution is one of the largest centers in the world specializing in gastric cancer treatment, and surgeons at the hospital perform surgeries on high-risk patients. 45 The most recent practices include new techniques, such as laparoscopic and robotic surgery.678910 Not necessarily limited to patient care delivery, the surgeons at this institution have been leading translational research in the field of gastric cancer,11121314151617 with the advantage of a high volume of surgical cases (over 1200 gastrectomies annually).
Dr. Sung Hoon Noh is a distinguished gastric cancer surgeon and a surgical oncologist. He is the head of the Gastric Cancer Clinic team at Severance Hospital, and his valuable contributions to the field of gastric cancer are important and meaningful. As a clinician, he performed his 10000th gastrectomy for gastric cancer on November 7th, 2017. As an academic surgeon, he has published more than 350 scientific papers. As a mentor, he has overseen the training of numerous international and domestic surgical fellows and residents, and has dedicated his career to bettering the understanding of gastric cancer and surgical oncology. He has also served in various positions in academic societies as a key opinion leader in the community. This article reviews his profound contributions and long history of service in the field of gastric cancer, including his 10000 consecutive gastric cancer surgeries, and provides perspectives from his experience. As his contributions to the field of gastric cancer are extensive, this review will surely omit achievements of Dr. Sung Hoon Noh that some of his colleagues consider very important. We wish the readers will be generous on any omissions.
RÉSUMÉ OF DR. NOH
Dr. Sung Hoon Noh has worked at Severance Hospital since 1987. He was the 16th Chairman of the Department of Surgery, Yonsei University College of Medicine (2009–2013), and Director of the Yonsei Cancer Center (2008–2009, 2013–2019). He has been a Fellow of the American College of Surgeons since 2008. He has served as the President of the Korean Gastric Cancer Association (2009–2011) and International Gastric Cancer Association (2011–2013); the Vice President of the Korean Society of Gastroenterology (2011–2012), the Chairman of the Board of the Korean Cancer Association (2011–2013), and the Chairman of the Board (2014–2018); and President of the Korean Surgical Society (2018–2019). He is a member of the National Academy of Medicine of Korea and the Korean Academy of Science Technology.
REVIEW OF THE 10000 GASTRECTOMIES FOR GASTRIC CANCER PERFORMED BY DR. NOH
Dr. Noh performed his first gastrectomy for gastric cancer in 1987, and has performed 10000 gastrectomies for gastric cancer as of November 7, 2017: his annual number of gastrectomies was over 600 at his peak (Fig. 1). The mean age of his patients was 56.9-years, with 6607 and 3393 male and female patients, respectively. He performed 6978 distal subtotal gastrectomies and 3022 total gastrectomies, including completion total gastrectomy. He treated all stages of gastric cancer, of which 50.1, 17.3, 27.8, and 4.5% were pathologic stages I, II, III, and IV, respectively (Table 1). His mean operative time was 190.1 minutes, including time for anesthesia; the mean hospital stay was 11.5 days; and there were 31 cases (0.31%) of surgical mortality within 30 days.
DEVELOPMENT AND STANDARDIZATION OF SURGICAL TECHNIQUES FOR GASTRIC CANCER
Dr. Noh first used an electrocautery device, “Bovie” for lymph node dissection in gastric cancer surgery in 1989. His use of the Bovie device for procedures in gastric cancer surgery increased over time, and he ultimately used the Bovie throughout the entire procedure. He first presented an operative video of gastric cancer surgery using the Bovie in 1995 at the Congress of the Korean Surgical Society. As this technique is now common, most young surgeons may not recognize the importance of this challenge; moreover, many senior surgeons criticized his use of the Bovie due to concerns for thermal injury to the bowel and blood vessels. He persevered and advanced this procedure and presented another operative video in 1996 on radical gastrectomy with D2 lymph node dissection for advanced gastric cancer using the Bovie at the Congress of the International Association of Surgeons, Gastroenterologists, and Oncologists. This procedure subsequently attracted international attention among surgeons.
Next, he expanded the application of the Bovie to spleenpreserving total gastrectomy. Historically, pancreatico-splenectomy was a standard procedure in radical total gastrectomy for gastric cancer because the extent of lymph node dissection includes supra-pancreatic and splenic hilar areas. In 1979, Dr. Maruyama developed pancreas preserving total gastrectomy. In 1995, he reported that pancreas-preserving total gastrectomy, compared to conventional total gastrectomy with distal pancreatectomy, had low morbidity and mortality with similar oncologic outcomes, and total gastrectomy with splenectomy subsequently became a standard procedure.18 Dr. Noh questioned the necessity of splenectomy for total gastrectomy and introduced spleen-preserving total gastrectomy with D2 lymph node dissection (including splenic hilar lymph node dissection). He presented a video of this procedure using the Bovie in 1997 at the 2nd International Gastric Cancer Congress.1920 Because this procedure was considered technically very difficult, its feasibility impressed other surgeons, many of whom, including gastric cancer experts, came to Yonsei University to observe Dr. Noh's technique. His clinical data showed that spleen preservation during total gastrectomy is associated with low morbidity and similar or better survival outcomes compared to those of total gastrectomy with splenectomy.2122 Subsequent studies including a randomized controlled trial supported his results,2324 and spleen preservation is now a standard procedure for total gastrectomy. He also developed new surgical techniques that can reduce anastomosis leakage after gastroduodenostomy.2526
Dr. Noh has sought to improve survival in gastric cancer with peritoneal metastases. He first used cyto-reductive surgery with intraperitoneal chemotherapy for gastric cancer in Korea in 1993,272829 followed by hyperthermic intraperitoneal chemotherapy (HIPEC) in 1995. These intraperitoneal treatments for recurrent gastric cancer have been revisited as chemotherapy regimens have evolved, and HIPEC, extensive peritoneal lavage,30 and most recently, pressurized intraperitoneal aerosol chemotherapy31 have been attempted and evaluated for efficacy in gastric cancer.
He has always emphasized the importance of oncologic principles in gastric cancer surgery to his fellows and residents. The “no-touch technique,” in which the tumor is wrapped with surgical tape or towels to prevent contamination of the surgeon's hands and dissemination in the surgical field and patient's abdomen, is a key principle in gastric cancer surgery. Minimizing manipulation of the stomach to reduce dissemination of tumor cells through blood and lymphatic vessels, anatomical and meticulous dissection with careful hemostasis to prevent direct spillage of tumor cells, and en-bloc lymphadenectomy with complete surgical resection of macro/microscopic tumors (R0) are also basic and important principles in gastric cancer surgery.
PROCEDURAL CHANGES BASED ON PATIENT-ORIENTED INSIGHTS
Dr. Noh was interested in reducing discomfort in patients undergoing surgery for gastric cancer. Believing that the patient is the most important part of the medical team, he was deeply concerned for frequent complaints of postoperative pain from the incision, nasogastric tube, and drainage tube. To relieve pain, he introduced the epidural patient-controlled analgesia pump in the clinic in 1997. He also demonstrated the feasibility of gastric cancer surgery with a <15-cm midline incision to reduce postoperative pain. In addition, to minimize surgical stress, he reduced operative time and blood loss, as well as the need for transfusion through his use of the Bovie.
Nasogastric tube insertion was for a long time a standard procedure for most gastrointestinal surgeries, with the belief that it could reduce postoperative anastomosis leakage and decompress bowel gas. He questioned this belief and conducted a single-center randomized controlled trial to compare clinical outcomes with and without nasogastric tube insertion for gastric cancer surgery and found no difference between the procedures.32 Accordingly, he discontinued routine nasogastric tube use for gastric cancer surgery in his clinic. To achieve a good operative field during surgery, he developed a simple technique to decompress the stomach and colon without the use of a nasogastric tube.3334
Dr. Noh also evaluated the necessity of routine intraperitoneal drainage for gastric cancer surgery and found no difference in short-term outcomes with or without use of a drainage tube.35 As his experience without using a drainage tube accumulated, he found that postoperative external drainage is required for some patients. He therefore developed a predictive model to identify high-risk patients who would require postoperative drainage,36 enabling selective insertion of a drainage tube in gastric cancer surgery. His collective efforts were the basis for the concept of enhanced recovery after surgery.
IMPROVING SURVIVAL IN GASTRIC CANCER THROUGH A MULTIDISCIPLINARY APPROACH
After a trial comparing the clinical outcomes of D2 versus D2 + para-aortic lymph node dissection failed to show the benefit of D4 lymph node dissection,37 the optimal extent of radical lymph node dissection was considered D2 level.383940 As techniques became standardized and postoperative management evolved, the benefit of radical surgery to survival in gastric cancer had reached a maximum. To improve survival in gastric cancer, another strategy, such as chemotherapy or radiation therapy, was needed; however, until 2001, it was thought that surgery was the only effective treatment option for resectable gastric cancer.41 The success of the Intergroup and MAGIC trials4243 showed the benefit of perioperative chemotherapy and postoperative chemotherapy combined with radiation therapy compared to surgery alone, leading to the era of adjuvant/neoadjuvant therapy for resectable gastric cancer. However, the trials were criticized because radical surgery with D2 lymph node dissection was only performed in some of the patients; furthermore, the prognosis of those who received additional treatment plus surgery was much worse than in patients who received radical surgery alone in Korea.
To evaluate the benefit of adjuvant chemotherapy after radical D2 surgery for gastric cancer, Dr. Noh and Dr. Yung-Jue Bang designed and conducted the Capecitabine and Oxaliplatin Adjuvant Study in Stomach Cancer (CLASSIC) trial targeting stage II/III gastric cancer. Thirty-seven institutions from Korea, China, and Taiwan participated in this open-label, parallel-group, phase III, prospective randomized controlled trial. This trial succeeded in showing the clear survival benefit of adjuvant chemotherapy after D2 surgery, compared to D2 surgery alone.4445 This result changed clinical practice from a D2 surgery alone strategy to D2 surgery plus adjuvant chemotherapy and contributed to improvement in survival in gastric cancer. These results were included in international guidelines for treatment of gastric cancer.404647
Another phase III, open-label, randomized controlled trial, PRODIGY, has been designed by Dr. Noh and Dr. Yoon-Koo Kang to determine whether early administration of chemotherapy in addition to conventional adjuvant chemotherapy would improve survival in gastric cancer (NCT01515748). In this study, the effect of Neoadjuvant Docetaxel+Oxaliplatin+S-1 (DOS)+Surgery+adjuvant S-1 compared to Surgery+adjuvant S-1 in patients with resectable advanced gastric cancer has been investigated. Enrollment in this trial has been completed and the final results will be announced soon. The trial is expected to provide another treatment option for patients with gastric cancer.
INTRODUCTION OF PRECISION MEDICINE FOR TREATMENT OF GASTRIC CANCER
Despite the success of the CLASSIC trial, there remains a number of unmet clinical needs in the treatment of gastric cancer. Most of all, few clinically applicable biomarkers have been identified for use in stratifying patients with resectable gastric cancer according to prognosis and/or response to chemotherapy. Given that more than approximately 60% of patients do not seem to benefit from adjuvant chemotherapy after curative intent D2 surgery, development of clinically usable biomarkers to identify these subgroup of patients is an urgent need in real-world clinic. According to the final result of the CLASSIC trial, estimated 5-year disease-free survival was 68% and 53% in the D2 surgery plus adjuvant chemotherapy group and D2 surgery only group, respectively.4445 The 15% added benefit was clinically valuable and suggested that half of patients with stage II/III gastric cancer can be treated with D2 surgery alone; however, only 15% of those treated with adjuvant chemotherapy received real benefit from chemotherapy, which caused treatment-related toxicity. If we can predict who will be cured with surgery alone without use of adjuvant chemotherapy, a significant number of patients can avoid unnecessary medication-induced toxicity. Moreover, if we can predict who will benefit from adjuvant chemotherapy, we can select patients for treatment using a current standard regimen or a regimen other than standard chemotherapy. In the middle of the CLASSIC trial, Dr. Noh realized the need for a biomarker study.
One possible biomarker is microsatellite instability (MSI). The clinical characteristics of MSI-high (MSI-H) colorectal cancer have been well studied; MSI-H tumors show good prognosis and are not responsive to 5-fluorouracil-based chemotherapy. 48 Consequently, guidelines recommend consideration of MSI status in colorectal cancer in deciding whether to use adjuvant chemotherapy.49 Dr. Noh and his colleagues conducted a meta-analysis and retrospective cohort studies to evaluate the clinical implications of MSI-H status in gastric cancer. As in colorectal cancer, MSI-H gastric cancer has a good prognosis, although the benefit from adjuvant chemotherapy in stage II/III gastric cancer was not clear.115051 These results were validated in randomized controlled trial cohorts in the CLASSIC and MAGIC studies.125253 Accordingly, MSI status has been deemed a powerful candidate biomarker that can be used in clinical practice, and treatment guidelines are likely to recommend its use in deciding treatment with or without chemotherapy for stage II/III gastric cancer.
Some trials have classified various tumors according to molecular characteristics,5455 some of which can be applied in clinical practice to predict responsiveness to chemotherapy.5657 Some molecular subtypes of gastric cancer have been evaluated according to genetic characteristics, including mRNA expression levels585960; however, the clinical implications were not clear or validated. Dr. Noh and his colleagues conducted a meta-analysis on mRNA expression data using multiple gastric cancer cohorts, including those from the Yonsei cohort, and found that gastric cancer can be stratified into five molecular subtypes based on the expression patterns of tumor transcriptome. Through rigorous statistical analyses, they identified four genes (with mRNA expression of five housekeeping genes), based on a single patient classifier (SPC) algorithm. According to the SPC algorithm, an immune type with enriched immune signatures (GZMB- and WARS-positive) was associated with a good prognosis, but was not responsive to adjuvant chemotherapy. Cancers with high expression of cancer stem-cell (ST type)-related gene (SFRP4) were associated with the worst prognosis. If cancer exhibits high expression of epithelial cell-related gene (CDX1, EP type), the benefit from adjuvant chemotherapy is obvious; however, a tumor with low expression of CDX1 is likely to receive no additional benefit from chemotherapy, compared to surgery alone. These results were validated in the CLASSIC trial cohort;14 consequently, the SPC algorithm was implemented in clinical practice to stratify patients with gastric cancer according to whether or not adjuvant chemotherapy should be given after surgery. Dr. Noh's collective efforts and achievements have ushered in the era of precision medicine for treatment of resectable gastric cancer.61
OTHER CONTRIBUTIONS
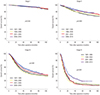
Dr. Noh planed establishing a clinical database in the Yonsei Gastric Cancer Clinic in 1993, and the first version was completed in 1998. This database made it possible to evaluate and respond to many clinical questions concerning gastric cancer, with the results leading to changes in treatment. Dr. Noh organized the Yonsei Gastric Cancer Symposium in 2000; this symposium was the first gastric cancer-specific conference in Korea, and the first to show live surgery in a symposium. The Yonsei Gastric Cancer Symposium has become an annual international event and has contributed to the dissemination of knowledge about gastric cancer surgery, including technical tips, treatment, biology, and translational research. Dr. Noh has also performed live surgeries in many countries to promote the excellence of gastric cancer treatment in Yonsei and Korea. Many surgeons from other countries including Japan visit Korea to learn about surgery for gastric cancer. To educate doctors who cannot visit Korea, he has organized live web seminars and for internet study. The efforts by Dr. Noh have led to progressively improved survival of patients with gastric cancer at Yonsei (Fig. 2).
PERSPECTIVES OF A MASTER SURGEON
Although major practice changes and scientific developments have occurred over the last decades, continued innovation is necessary to curb the burden of gastric cancer. New screening systems targeting high-risk individuals based on genomic characteristics should be developed for super-early detection of gastric cancer. How we manage the rapid increase in survivors of gastric cancer and the occurrence of a second malignancy should be considered. Since the extent of lymph node dissection for advanced gastric cancer is set at D2 level, current surgery is somewhat standardized rather than personalized. Improving our knowledge of cancer biology will enable us to predict lymph node metastasis before surgery, and advances in technology for intraoperative visualization of lymph nodes6 will make it possible to perform tailored surgery. Consequently, the roles of limited and minimally invasive surgery including endoscopic resection and robot-assisted surgery will expand. Combined targeted therapy and immunotherapy based on molecular characteristics if individual tumors will be accepted, and the treatment of patients can be tailored in greater detail as the concept of the N-of-one trial being realized, leading to personalized treatment. Although surgery has not seemed helpful in patients with distant metastases,62 we will be able to identify subgroups in which surgery can cure the disease, as some of these patients will demonstrate long-term survival.63 Future changes will be based on not only the molecular characteristics of tumor itself but also those of the patients, and the importance of a multi-disciplinary approach will be further emphasized. Clinician-based Multi-Disciplinary Treatment will and should evolve to Integrative Multi-Disciplinary Health Care that includes not only clinicians but also basic scientists, ancillary providers, and even patients and their families. At the center of these changes, surgeons should spearhead paving the road and taking legitimate leadership. This requires understanding of the biology of cancer and active involvement in clinical, translational, and basic research. We are now in an era of precision health care beyond precision surgery.


 XML Download
XML Download