

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Current guidelines suggest that adequate treatment of locally advanced rectal cancer consists of curative resection followed by neoadjuvant chemoradiation (nCRT) [12], which is associated with better local control [3] and possibly improved sphincter preservation [4]. Response to nCRT differs among patients with rectal cancer, with pathologic complete response (pCR) observed in 15%–20% of cases [5]. It is important to predict pCR to nCRT in locally advanced rectal cancer, because pCR is associated with not only a low rate of local recurrence but also favorable long-term survival [56]. Numerous clinical, radiologic, and molecular features have been investigated as possible predictors of pCR, but currently, no robust markers exist [7].
Meanwhile, obesity has been reported to be associated with surgical outcomes following rectal cancer [89]. Because of the associated technical difficulties in performing total mesorectal excision, obesity was found to increase local recurrence as well as postoperative morbidity [89]. Also, obesity may decrease the possibility of sphincter preservation [89]. In addition, some studies reported a relationship between obesity and oncologic outcomes of patients with rectal cancer following nCRT, although their results were controversial [1011121314]. Given the fact that obesity is associated with inflammation and angiogenesis [15] and is associated with the chronic oxidative stress [16], it is possible to consider the possibility that obesity is related to the response of radiotherapy. However, few previous studies reported the significance of obesity in predicting pCR after nCRT in rectal cancer [13].
Therefore, we designed the present study to investigate the possible association between obesity and pathologic response to nCRT, as well as subsequent oncologic outcomes in patients with rectal cancer.
METHODS
This study was approved and informed consent was waived by the Institutional Review Board of Chonnam National University Hwasun Hospital (CNUHH-2018-004). We retrospectively reviewed clinicopathologic data of patients with primary rectal cancer who underwent curative resection following nCRT between January 2010 and September 2014. Patients with distant metastasis were excluded. Obesity was defined as body mass index (BMI) of ≥ 25 kg/m2 according to Asian BMI classification [17].
Preoperative evaluation
All patients were evaluated with serum CEA, colonoscopy, abdominopelvic and chest CT, pelvic MRI, and/or endorectal ultrasound for local staging. Prior to nCRT, rigid rectoscopy was used to assess the distance of the tumor from the anal verge, and this was classified into 3 groups: lower rectum (0–5 cm), middle rectum (6–10 cm), and upper rectum (11–15 cm). Both tumor circumferentiality and macroscopic ulceration were also determined by rigid rectoscopy by the attending surgeon. Macroscopic ulcerative tumors were defined as ulcerative, diffuse infiltrative, or annular constrictive rectal tumors, and circumferential tumors were defined as those involving >75% of the circumference of the rectum [18]. Clinical tumor size, which means the maximal diameter of the tumor, was measured by endorectal ultrasound and/or pelvic MRI. Included patients received nCRT, which consisted of long-course radiation (5,040 cGy in 28 fractions) and concomitant 5-fluorouracil-based chemotherapy. Study inclusion criteria for nCRT administration were locally advanced rectal cancers (clinical diagnosis of ≥T3 or ≥N1) or low rectal cancer of cT2N0 for sphincter-preserving surgery.
Surgery and adjuvant therapy
Radical surgery was performed with curative intent 6–10 weeks after the completion of radiotherapy. In all patients, surgery was conducted according to general oncologic principles. The surgeon in each case decided whether to perform abdominoperineal resection or sphincter-preserving surgery. Anastomosis was performed by either the double-stapling method or the hand-sewing method in very-low rectal cancer. Administration of adjuvant chemotherapy was determined by the medical oncologist based on the patient's condition. In general, 5-fluorouracil-based adjuvant chemotherapy was recommended for all patients regardless of their final pathologic stage.
Pathologic examination
The final pathologic features were restaged according to the seventh edition of the American Joint Committee on Cancer TNM staging system at the time of data review. We defined pCR as the absence of adenocarcinoma cells in the surgical specimen (ypT0N0). Circumferential resection margin was determined to be positive in cases of margin < 1 mm. Tumor regression grade was classified according to the Dworak/Rödel grading system [19].
Follow-up
Patients underwent follow-up every 3 months during the first 2 years, at 6-month intervals for the next 3 years, and annually thereafter. Serum CEA tests, abdominopelvic and chest CT, colonoscopy, and positron emission tomography were conducted on a semiannual basis or in cases of suspected recurrence. Recurrence was diagnosed via radiological detection of lesions with increasing size or by histological confirmation. Local recurrence was defined as recurrent disease in the pelvic cavity, including the anastomosis and lateral pelvic wall. Distant metastasis was defined as disease outside the pelvis.
Statistical analysis
Categorical variables were compared using the chi-square test or Fisher exact test, and continuous variables were compared using Student t-test. Multivariate logistic regression analysis was also performed to explore predictive factors for pCR. Survival rates were estimated and compared using the Kaplan-Meier method and log-rank test. The Cox proportional hazard model was utilized for multivariate survival analysis. Results were considered significant at P < 0.05. Statistical analyses were conducted using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA).
RESULTS
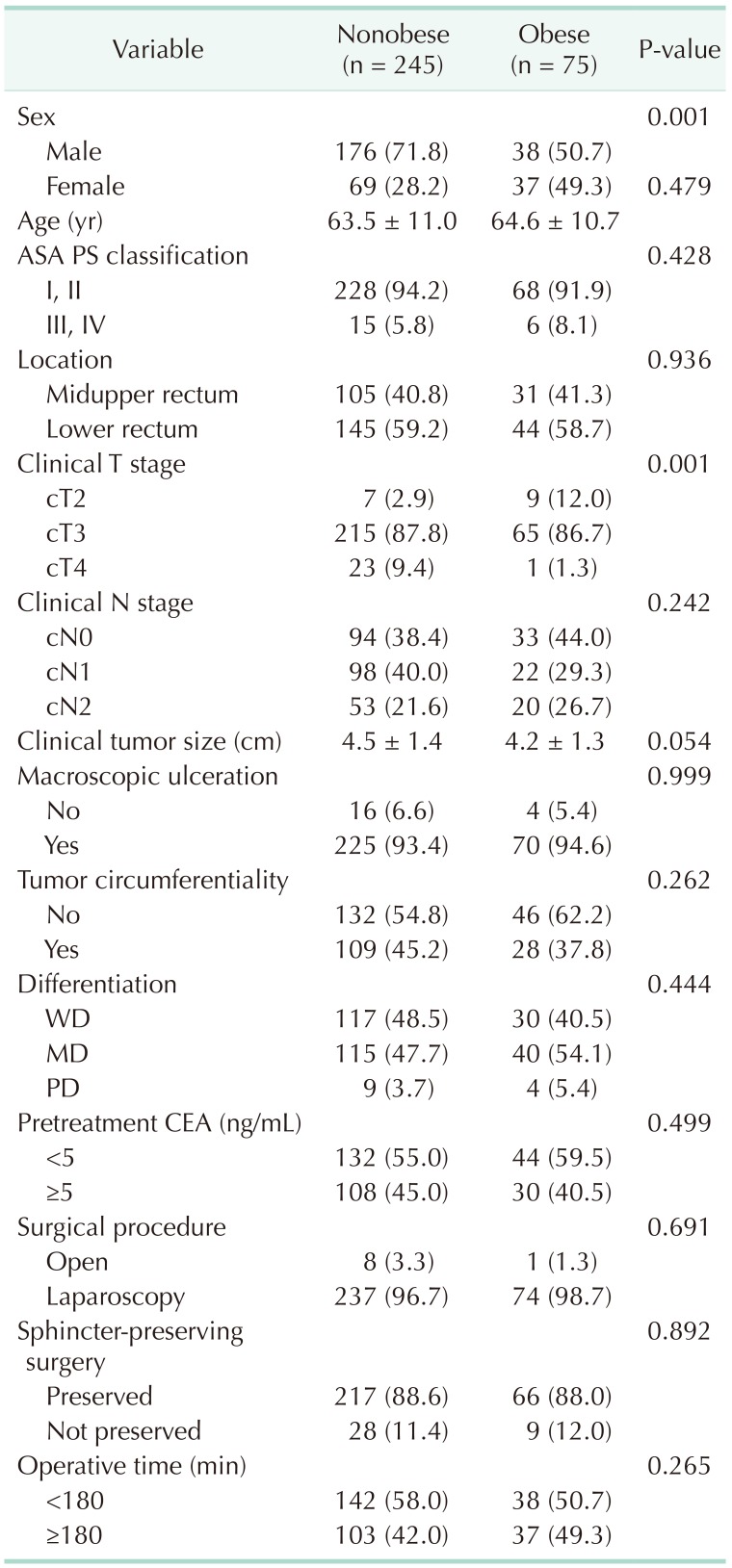
Among the 320 patients included, 75 (23.4%) were classified as obese. Table 1 shows the baseline characteristics of the patients according to obesity status. In general, clinical variables were similar between obese and nonobese patients, except that more women (49.3% vs. 28.2%, P = 0.001) and more cT2 disease (12.0% vs. 2.9%, P = 0.001) were found among the obese patients.
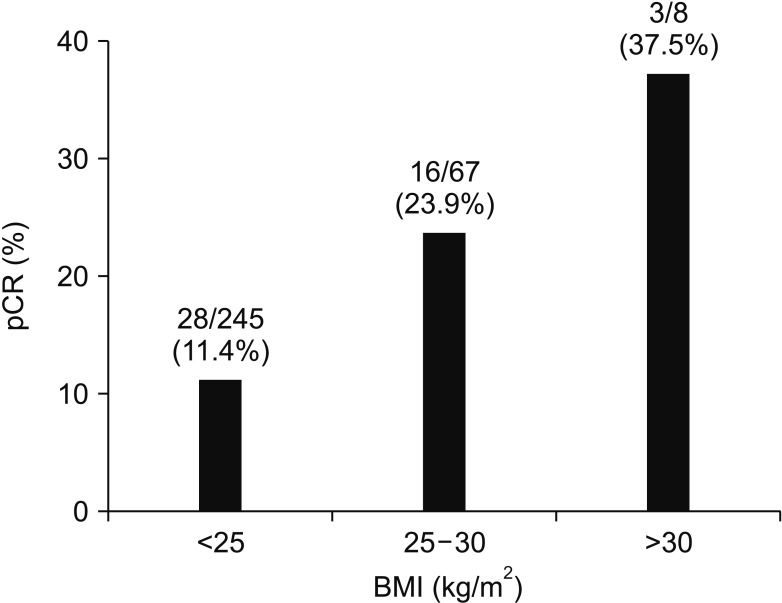
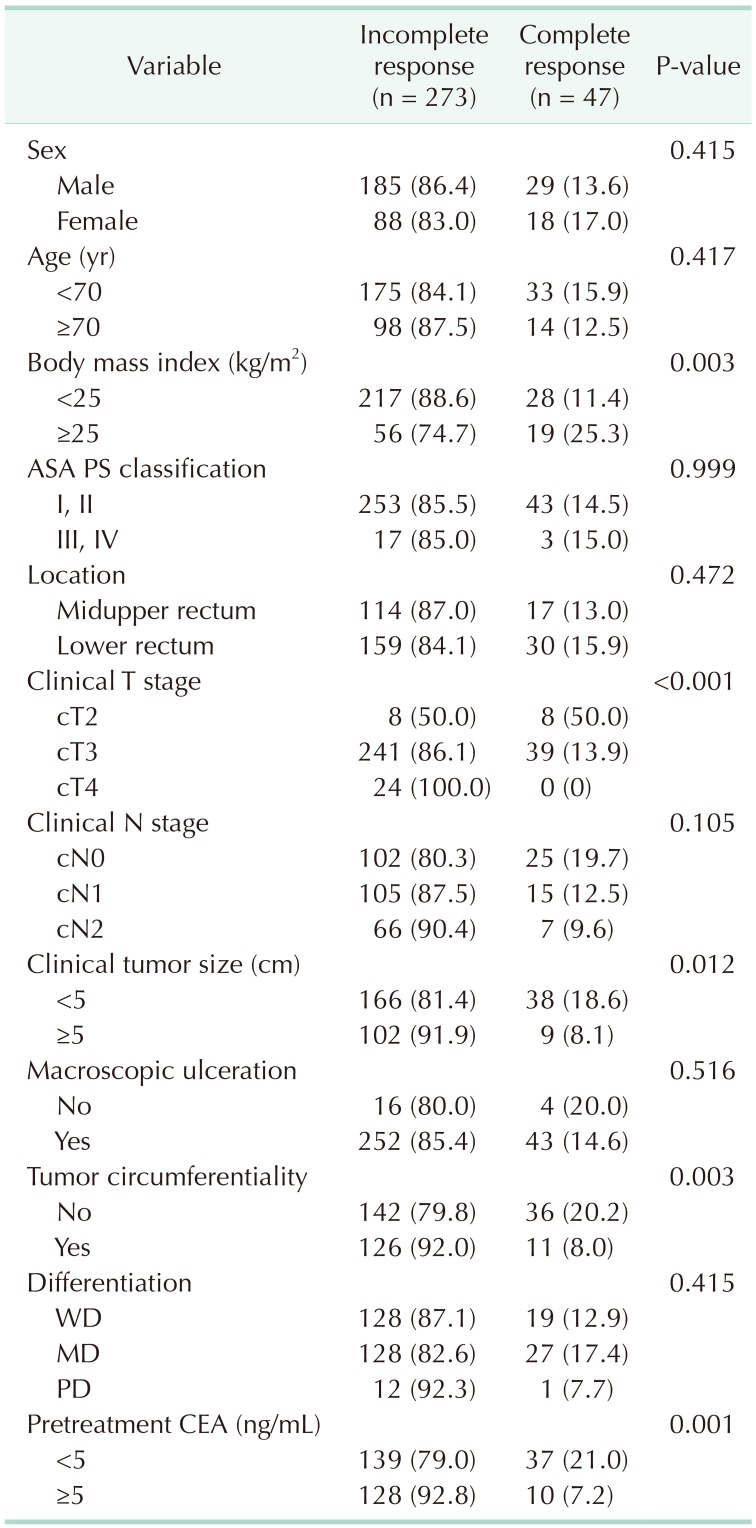
A total of 47 patients (14.7%) showed pCR. When analyzing the relationship between BMI and pCR, the higher the BMI, the higher the pCR ratio (BMI < 25, 25–30, and ≥ 30 kg/m2; pCR 11.4%, 23.9%, and 37.5%, respectively) (Fig. 1). We analyzed associations between clinical variables and pathologic response to nCRT, and found that BMI ≥ 25 kg/m2 (25.3% vs. 11.4%, P = 0.003), clinical T stage (cT2, 50.0% vs. cT3, 13.9%, and cT4, 0%, P < 0.001), clinical tumor size (<5 cm, 18.6% vs. ≥5 cm, 8.1%, P = 0.012), tumor circumferentiality (8.0% vs. 20.2%, P = 0.003), and pretreatment CEA (<5 ng/mL, 21.0% vs. ≥5 ng/mL, 7.2%, P = 0.001) were related to pCR rate (Table 2). On multivariate logistic regression, obesity (adjusted odds ratio [OR], 2.051; 95% confidence interval [CI], 1.009–4.168), cT2 (adjusted OR, 3.614; 95% CI, 1.166–11.202), and pretreatment carcinoembryonic antigen <5 ng/mL (adjusted OR, 2.921; 95% CI, 1.365–6.253) were independent predictors for pCR (Table 3).
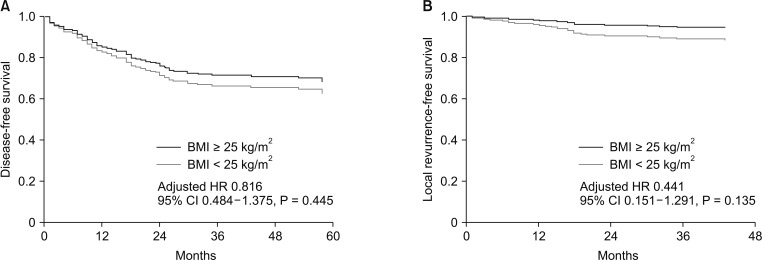
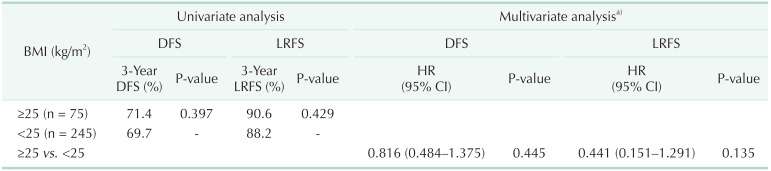
After a median follow-up period of 42 months (range, 1–83 months), 99 patients (30.9%) experienced recurrence, and 33 of these (10.3%) had local recurrence. The overall rates of disease-free survival (DFS) and local recurrence-free survival (LRFS) at 3 years were 67.4% and 88.8%, respectively. Table 4 summarizes the results of univariate and multivariate survival analyses for DFS and LRFS. Obese patients had a tendency toward better DFS (71.4% vs. 69.7%, P = 0.397) and LRFS (90.6% vs. 88.2%, P = 0.429) compared with nonobese patients, although these findings were not statistically significant. On multivariate survival analysis, obesity was not associated with either DFS (hazard ratio [HR], 0.816; 95% CI, 0.484–1.375; P = 0.445) or LRFS (HR, 0.441; 95% CI, 0.151–1.291; P = 0.135) (Fig. 2).
DISCUSSION
In the present study, we investigated the association between obesity and pCR following nCRT in patients with rectal cancer. Obesity was an independent predictor of pCR after adjusting for possible confounders, although it was not associated with recurrence.
The association between obesity and cancer recurrence has been widely investigated in breast cancer, and was shown to be associated with local recurrence, distant metastasis, and decreased overall survival [202122]. One possible reason for these findings is that increased adipose tissue may elevate the levels of circulating estrogens, insulin, and insulin-like growth factors, which can facilitate cancer cell growth [22]. In contrast, some studies have reported that obesity was associated with better prognosis after chemoradiation in other types of cancers, such as cervical cancer, lymphoma, and head and neck cancers [2324252627]. These studies commonly suggested that better survival in obese patients might be caused by better tolerance to chemoradiation and/or surgery. Patients with higher BMI may withstand the inevitable weight loss after treatment including chemoradiation [26], and underweight patients may be more likely to suffer from comorbidities because of their weakened immune systems [27], factors that could result in survival differences.
On the other hand, there have been only a few studies reporting on associations between obesity and oncologic outcomes in rectal cancer following nCRT [1011121314]. Three studies demonstrated poorer survival and/or a lower rate of pCR in obese patients [111213], whereas one study reported similar survival outcomes between obese and nonobese patients [10], and a recent study even reported that obesity was an independent favorable prognostic factor for DFS in patients with rectal cancer treated with nCRT [14]. These studies reported conflicting results, and some were limited by their small sample sizes [111214]. In the present study, we showed that obesity was an independent predictor of pCR. In addition, although multivariate survival analysis showed that obesity was not associated with DFS and LRFS, a tendency (HR, 0.441; 95% CI, 0.151–1.291) was observed between obesity and better LRFS (Table 4, Fig. 2). As is widely known, pCR brings about desirable oncologic outcomes [56]. Therefore, if obesity brings a higher rate of pCR, it is likely that obesity is associated with better DFS or LRFS. Considering the association between obesity and pCR, a possible hidden relationship between obesity and improved oncologic outcomes must be investigated by means of future large-scale studies.
The reason for the close relationship between obesity and response to radiotherapy is uncertain. One possible explanation is that obesity is associated with a state of chronic inflammation. In adipose tissue in obese patients, the number of macrophages and subsequent production of inflammatory cytokines are increased [28]. In other words, excessive adipose tissue in obese patients is associated with inflammation, angiogenesis, and immune cell infiltration [15]. This interplay between obesity and immune response may alter the tumor microenvironment and increase the tumor response to radiotherapy [26]. Furthermore, obesity is related to increased levels of free fatty acids, which may stimulate the production of reactive oxygen species. Obesity-induced chronic oxidative stress may induce epigenetic alterations, which could result in a different response to radiotherapy [16]. Another possible mechanism is a hidden interaction between obesity and molecular signaling pathways. Gomez-Millan et al. [14] recently reported that patients with rectal cancer who expressed nuclear β-catenin showed better DFS after nCRT than those who did not express β-catenin. Nuclear β-catenin has been reported to be associated with better cancer-specific and overall survival in obese patients [29]. Therefore, alterations of key components in the Wnt/β-catenin signaling pathway caused by diet-induced obesity may be a possible reason for the relationship between obesity and the response to radiotherapy [28]. Further translational research may be needed to investigate this issue.
There are some limitations in the present study. As described above, the group of obese participants included higher percentage of patients with cT2 disease, which may represent a selection bias. To overcome this confounding effect, we performed multivariate logistic regression analysis and showed that both cT2 disease and obesity were independent predictive factors for pCR. Therefore, we strongly believe that the results of the present study are still meaningful. Another limitation is that we could not elucidate the exact mechanism underlying the relationship between obesity and better response to radiotherapy. Therefore, there is still a possibility that the results of this study may not reflect the actual phenomenon, but merely a result of statistical analysis. Nevertheless, a strength of this study is that it is one of the rare studies reporting an association between obesity and pathologic response in rectal cancer after nCRT.
In conclusion, obesity was an independent predictive factor for pCR after nCRT in rectal cancer, although it was not associated with recurrence. Further studies to explore the mechanism of the relationship between obesity and pathologic response to nCRT are warranted.

 XML Download
XML Download