

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most commonly encountered cardiac arrhythmia in the clinical practice,1)2) and is associated with a 4- to 5-fold increase in stroke risk.2) Stroke prevention is the principal management priority in patients with AF. Vitamin K antagonists (VKAs) have been the maintenance of oral anticoagulant (OAC) treatment for several decades and reduce the relative risk of stroke in patients with AF by 64% and all-cause mortality by 26%, compared to control.3) However, VKAs have many limitations including narrow therapeutic window, variability in dose response, slow onset and offset of action, and food and drug interactions.4)
The non-VKA oral anticoagulants (NOACs) have all been proven at least as effective and safe as warfarin in large randomized controlled trials,5)6)7)8) with a lower incidence of intracranial hemorrhage (ICH). Indeed, NOACs also have advantages compared with warfarin, such as fewer drug–drug and food–drug interactions and no requirement for routine coagulation monitoring.9) Current guidelines recommend preferential use of NOAC in patients with nonvalvular AF and risk of thromboembolic events.10)11) Nevertheless, the use of NOAC has been limited due to both economical and medical reasons.
In patients with AF, rivaroxaban was noninferior to warfarin for the prevention of stroke or systemic embolism. There was no significant between-group difference in the risk of major bleeding, although intracranial and fatal bleeding occurred less frequently in the rivaroxaban group.6) Cost-effectiveness of NOAC was well demonstrated in western counties. However, it has not been well assessed in Asian countries. The aim of our study was to evaluate the costs, cost-effectiveness, quality-adjusted life years (QALYs), and incremental cost-effectiveness ratio (ICER) of rivaroxaban compared to adjusted-dose warfarin for the prevention of stroke in Korean patients with AF.
METHODS
This study is based on the national health claims database established by the Health Insurance Review & Assessment Service (HIRA) of Republic of Korea.12)13) The National Health Insurance Service (NHIS) is the single insurer controlled by the Korean government, and the majority (97.1%) of Korean population are mandatory subscribers, with the remaining 3% of the population being medical aid subjects. HIRA database contains the information of medical aid subjects, therefore it is based on the entire Korean population.12)13) The sociodemographic information of patients, their use of inpatient and outpatient services, pharmacy dispensing claims, and mortality data are provide. Every subject in the HIRA database was linked by the Korean social security numbers. This study was approved by the Institutional Review Board of Yonsei University Health System (4-2016-0179) and informed consent was waived.
Study population
In the Korean NHIS data, 109,125 patients with prevalent AF who were aged 18 years or older were identified during the period from January 1, 2012 to December 31, 2014. After the diagnosis of AF, warfarin and rivaroxaban were used to confirm the prescription, and the number of all drugs used in the analysis was calculated. It was prescribed for 20,431 patients with warfarin, and 713 patients with rivaroxaban. The following were exclusion criteria: 1) those with valvular AF such as moderate to severe mitral valve stenosis and prosthetic valve disease (International Classification of Disease [ICD]-I050, I052, I342), and 2) those who ever received treatment with NOAC before enrollment. Finally, this study included 19,895 patients who had taken warfarin and 709 patient who had taken rivaroxaban.
AF was diagnosed using the International Classification of Disease 10th Revision (ICD-10) codes, I48 (AF and atrial flutter), I48.0 (AF), and I48.1 (atrial flutter). Moreover, patients were defined as AF only when it was a discharge diagnosis or confirmed more than twice in the outpatient department to ensure diagnostic accuracy. The AF diagnosis has previously been validated in the NHIS database with a positive predictive value of 94.1%.1)14)15)
Decision tree model
The cost-effectiveness of rivaroxaban (at a daily dose of 20 mg) compared to adjusted-dose warfarin in patients with AF was evaluated using a Markov chain Monte Carlo model. Rivaroxaban was reduced to a daily dose of 15 mg in patients with creatinine clearance from 15 to 50 mL/min.16) The base-case analysis assumed a cohort of patients with AF who were aged 18 years or older regardless of congestive heart failure, hypertension, age ≥75 (doubled), diabetes mellitus, prior stroke or transient ischemic attack (doubled), vascular disease, age 65 to 74, female (CHA2DS2-VASc) score (CVS).
The CHA2DS2-VASc score was calculated using the medical history of the past year for AF diagnosis. The CHA2DS2-VASc scores of 0, 1 and 2 or more were classified as low-, intermediate- and high-risk group, respectively.17)
Adherence rates of therapy were assumed to be similar across all treatments, and the efficacy was assumed to remain constant over time for rivaroxaban and warfarin. Patient movement between health states was modeled using 1-month cycles for 20 years or until death. The mean age of the patients was 66.5 years for men and 71.8 years for women in analysis, and twenty cycles were repeated to determine the transition probability to the final health state, considering that the average life expectation was 77.3 years for men and 84 years for women.18)
Baseline comorbidities and outcomes were defined using the medical claims and prescription medication. In order to ensure diagnostic accuracy, the patients were considered to have comorbidities when the condition was a discharge diagnosis or was confirmed at least twice in an outpatient setting, which was similar to previous studies with NHIS (Supplementary Table 1).2)12)19) The base case included the following health states: healthy, ischemic stroke, ICH, myocardial infarction (MI), and death (Figure 1). We classified all events into fatal and non-fatal. Events related with death were defined as fatal events. Non-fatal ischemic stroke included stroke with major (moderated to severe neurologic residua), minor (neurologic residua), or reversible ischemic neurologic deficit (no neurologic residua).20) Non-fatal ICH included ICH with major, minor or no neurologic deficit.21) Non-fatal gastrointestinal (GI) bleeding events included overt or occult GI tract bleeding. Non-fatal MI was defined MI events which was not related with death.
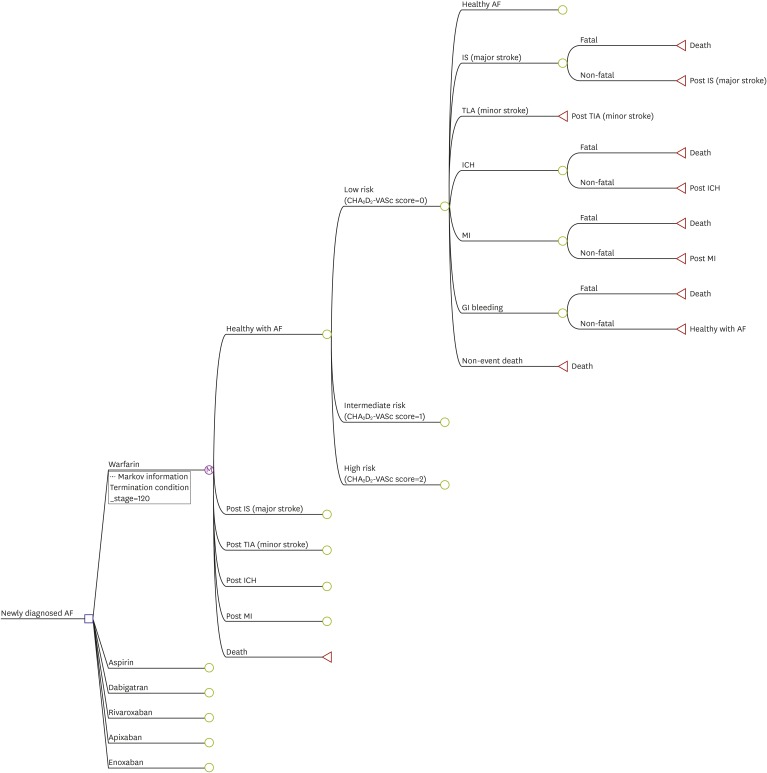
Figure 1
Schematic representation of Markov model shows that all patients start at 65 years of age with AF and then cycle between health states until death occurs or the 20-year time horizon is reached. Probabilities of these events depend on prescribed therapies. The length of each cycle is 1 year. Patients can die from stroke, hemorrhage, MI, or other co-morbidities. Decision node (square), chance nodes (circles) under the control of transition probabilities, and terminal nodes (triangles) are depicted.
AF = atrial fibrillation; ECH = extracranial hemorrhage; M = Markov node; MI = myocardial infarction; RIND = reversible ischemic neurological deficit.
![]()
Over a period of 30 years using a societal perspective, quality-adjusted life expectancy, risk of adverse events, and net costs were quantified.
All costs were calculated in Korean won (KRW) and converted into US dollar (1 US dollar=1,000 KRW). Cost-effective therapies were selected using a willingness-to-pay threshold of $30,000 per QALY gained.22) Model implementation, sensitivity analyses, and outcome calculations were performed using TreeAge Pro 2012 (TreeAge Inc, Williamstown, MA, USA).
Probability and severity of adverse events
In our study, the probability parameters of NOACs and adverse events of warfarin were based on nation specific real-world data using HIRA registration data.
In the diagnosis of AF, HIRA data were used to calculate the CHA2D2-VASc scores of patients, and also, the ratio of low, intermediate, and high-risk was calculated.6) Probabilities of adverse events for warfarin were calculated from pooled data. If ischemic stroke, transient ischemic accident (TIA), ICH or MI were non-fatal, they were considered as post disease status. In contrast, if they were fatal, they were considered to death. Non-fatal GI bleeding was considered to as “healthy with AF.”
Utilities
The baseline patient utility value was adjusted for age, AF, and OAC treatment.23) Subsequent disutilities for ischemic stroke, neurological events with residual symptom, MI, GI hemorrhage, and minor hemorrhage were estimated using pooled nationally representative Medical Expenditure Panel Survey data, as well as derived from published population-specific articles.23)
Cost
We defined the healthy state is assumed to be transition in annually. The transient probability is determined by the probability of an independent health event occurring within 1 year. The probability of occurrence of each health event was estimated based on the data of the newly diagnosed AF patient from January 1, 2012 to December 31, 2014.
The cost was composed of single event cost, medication cost, maintenance cost. The cost of each event (GI bleeding, hemorrhage, and MI) was defined as hospitalization costs for each health events and it was calculated based on HIRA data. Annual costs of medication were defined as 365 times the price of daily medication price also based on HIRA. Post-event cost was defined as the total cost minus medication cost and event related cost.
Costs and QALYs were implemented in each cycle according to the health state of patients. According to the amount of time a person spent in the health state, the costs and QALYs accrued for each Markov state were weighted. Costs were calculated in US dollars and utility was based on QALY units. The utility value corresponding to each health condition was defined in the existing literature. The cost-effectiveness of each healthy state was compared through an ICER. The willing-to-pay ratio was set at 30,000 USD/QALY to reflect the GDP (US $29,115 in 2017). The discount rate is set at 5% per annum, reflecting the annual inflation rate in Korea.
RESULTS
Number of patients with CHA2DS2-VASc scores 0, 1 and ≥2 were 56 (0.2%), 1,944 (6.3%) and 28,650 (93.5%), respectively. In patients with CHA2DS2-VASc scores ≥2, the incidence rate of ischemic stroke was 3.11% and 3.76% in warfarin and rivaroxaban groups, respectively. The incidence rate of ICH was 0.42% and 0.15% in warfarin and rivaroxaban, respectively. Moreover, the incidence rate of GI bleeding was 0.32% and 0.15% in warfarin and rivaroxaban, respectively.
Warfarin disutility was 0.03 and rivaroxaban disutility was 0.004.24)25) Disutility of major ischemic stroke or ICH, GI bleeding, and MI were 0.75, 0.85, and 0.84, respectively. Annual medication cost was $23 for warfarin and $847.9 for rivaroxaban. The cost of major ischemic stroke, TIA, MI, hemorrhagic stroke, and GI bleeding were $2,318.68, $2,361.62, $2,337.87, $2,666.39, and $3,218.91, respectively (Table 1).
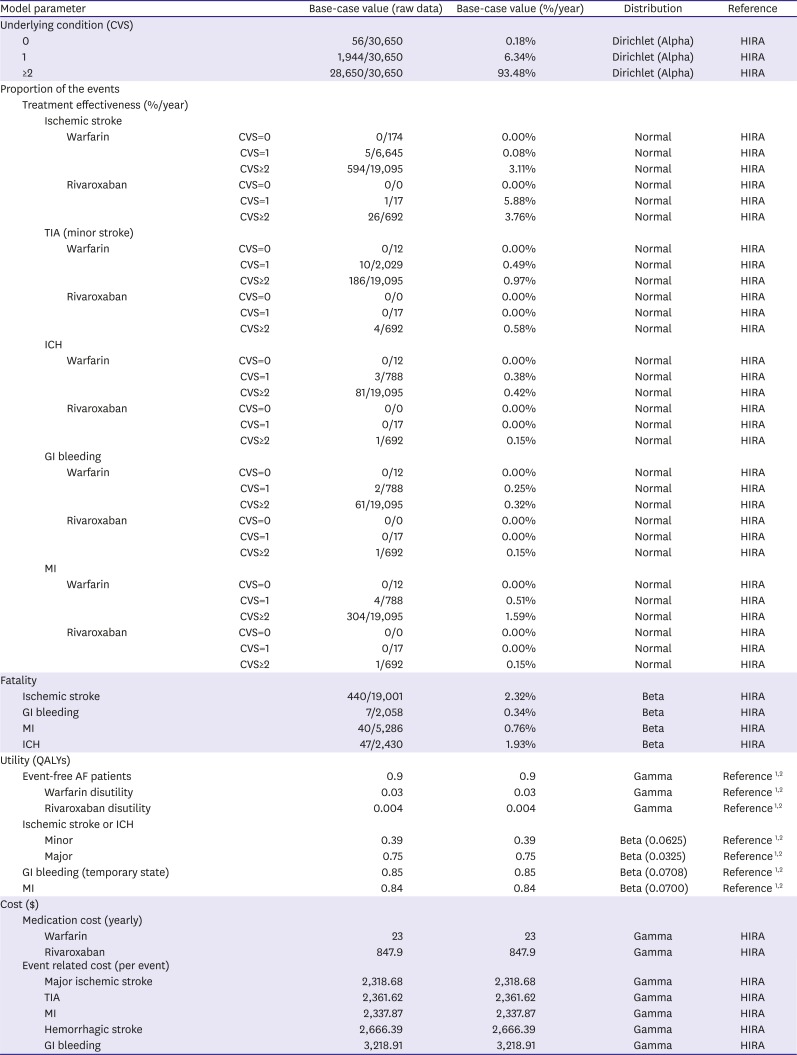
Table 1
Base-case model variables and ranges used in sensitivity analysis
| Model parameter | Base-case value (raw data) | Base-case value (%/year) | Distribution | Reference | ||||
|---|---|---|---|---|---|---|---|---|
| Underlying condition (CVS) | ||||||||
| 0 | 56/30,650 | 0.18% | Dirichlet (Alpha) | HIRA | ||||
| 1 | 1,944/30,650 | 6.34% | Dirichlet (Alpha) | HIRA | ||||
| ≥2 | 28,650/30,650 | 93.48% | Dirichlet (Alpha) | HIRA | ||||
| Proportion of the events | ||||||||
| Treatment effectiveness (%/year) | ||||||||
| Ischemic stroke | ||||||||
| Warfarin | CVS=0 | 0/174 | 0.00% | Normal | HIRA | |||
| CVS=1 | 5/6,645 | 0.08% | Normal | HIRA | ||||
| CVS≥2 | 594/19,095 | 3.11% | Normal | HIRA | ||||
| Rivaroxaban | CVS=0 | 0/0 | 0.00% | Normal | HIRA | |||
| CVS=1 | 1/17 | 5.88% | Normal | HIRA | ||||
| CVS≥2 | 26/692 | 3.76% | Normal | HIRA | ||||
| TIA (minor stroke) | ||||||||
| Warfarin | CVS=0 | 0/12 | 0.00% | Normal | HIRA | |||
| CVS=1 | 10/2,029 | 0.49% | Normal | HIRA | ||||
| CVS≥2 | 186/19,095 | 0.97% | Normal | HIRA | ||||
| Rivaroxaban | CVS=0 | 0/0 | 0.00% | Normal | HIRA | |||
| CVS=1 | 0/17 | 0.00% | Normal | HIRA | ||||
| CVS≥2 | 4/692 | 0.58% | Normal | HIRA | ||||
| ICH | ||||||||
| Warfarin | CVS=0 | 0/12 | 0.00% | Normal | HIRA | |||
| CVS=1 | 3/788 | 0.38% | Normal | HIRA | ||||
| CVS≥2 | 81/19,095 | 0.42% | Normal | HIRA | ||||
| Rivaroxaban | CVS=0 | 0/0 | 0.00% | Normal | HIRA | |||
| CVS=1 | 0/17 | 0.00% | Normal | HIRA | ||||
| CVS≥2 | 1/692 | 0.15% | Normal | HIRA | ||||
| GI bleeding | ||||||||
| Warfarin | CVS=0 | 0/12 | 0.00% | Normal | HIRA | |||
| CVS=1 | 2/788 | 0.25% | Normal | HIRA | ||||
| CVS≥2 | 61/19,095 | 0.32% | Normal | HIRA | ||||
| Rivaroxaban | CVS=0 | 0/0 | 0.00% | Normal | HIRA | |||
| CVS=1 | 0/17 | 0.00% | Normal | HIRA | ||||
| CVS≥2 | 1/692 | 0.15% | Normal | HIRA | ||||
| MI | ||||||||
| Warfarin | CVS=0 | 0/12 | 0.00% | Normal | HIRA | |||
| CVS=1 | 4/788 | 0.51% | Normal | HIRA | ||||
| CVS≥2 | 304/19,095 | 1.59% | Normal | HIRA | ||||
| Rivaroxaban | CVS=0 | 0/0 | 0.00% | Normal | HIRA | |||
| CVS=1 | 0/17 | 0.00% | Normal | HIRA | ||||
| CVS≥2 | 1/692 | 0.15% | Normal | HIRA | ||||
| Fatality | ||||||||
| Ischemic stroke | 440/19,001 | 2.32% | Beta | HIRA | ||||
| GI bleeding | 7/2,058 | 0.34% | Beta | HIRA | ||||
| MI | 40/5,286 | 0.76% | Beta | HIRA | ||||
| ICH | 47/2,430 | 1.93% | Beta | HIRA | ||||
| Utility (QALYs) | ||||||||
| Event-free AF patients | 0.9 | 0.9 | Gamma | Reference 12 | ||||
| Warfarin disutility | 0.03 | 0.03 | Gamma | Reference 12 | ||||
| Rivaroxaban disutility | 0.004 | 0.004 | Gamma | Reference 12 | ||||
| Ischemic stroke or ICH | ||||||||
| Minor | 0.39 | 0.39 | Beta (0.0625) | Reference 12 | ||||
| Major | 0.75 | 0.75 | Beta (0.0325) | Reference 12 | ||||
| GI bleeding (temporary state) | 0.85 | 0.85 | Beta (0.0708) | Reference 12 | ||||
| MI | 0.84 | 0.84 | Beta (0.0700) | Reference 12 | ||||
| Cost ($) | ||||||||
| Medication cost (yearly) | ||||||||
| Warfarin | 23 | 23 | Gamma | HIRA | ||||
| Rivaroxaban | 847.9 | 847.9 | Gamma | HIRA | ||||
| Event related cost (per event) | ||||||||
| Major ischemic stroke | 2,318.68 | 2,318.68 | Gamma | HIRA | ||||
| TIA | 2,361.62 | 2,361.62 | Gamma | HIRA | ||||
| MI | 2,337.87 | 2,337.87 | Gamma | HIRA | ||||
| Hemorrhagic stroke | 2,666.39 | 2,666.39 | Gamma | HIRA | ||||
| GI bleeding | 3,218.91 | 3,218.91 | Gamma | HIRA | ||||
AF = atrial fibrillation; CVS = congestive heart failure, hypertension, age ≥75 (doubled), diabetes mellitus, prior stroke or transient ischemic attack (doubled), vascular disease, age 65 to 74, female (CHA2DS2-VASc) score; GI = gastrointestinal; HIRA = Health Insurance Review & Assessment Service; ICH = intracranial hemorrhage; MI = myocardial infarction; QALYs = quality-adjusted life years; TIA = transient ischemic attack.
![]()
Cost-effectiveness of rivaroxaban and warfarin
Under base-case hypothesis, patients who treated with adjusted-dose warfarin lived an average of 11.4±0.2 QALYs, and caused mean lifetime treatments costs of $17,151. Those treated with rivaroxaban lived a mean of 11.8±0.2 QALYs, with an average lifetime cost of $20,886 (Table 2). Figure 2 shows the cost-effectiveness scatterplot of rivaroxaban and warfarin.
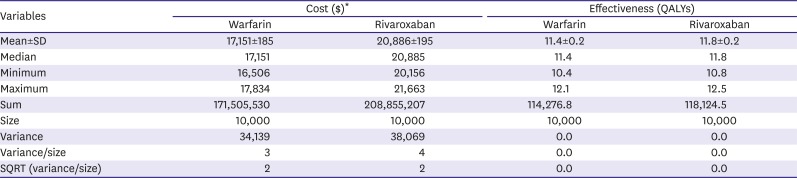
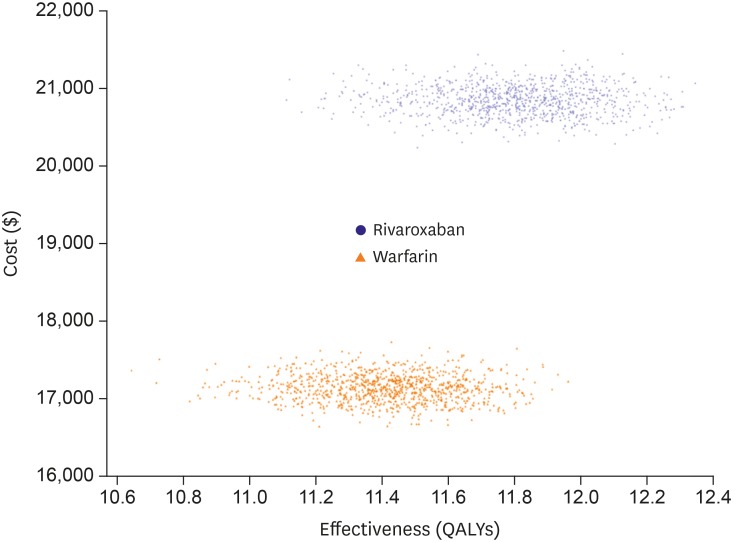
Table 2
Descriptive statistics of cost and effectiveness for warfarin and rivaroxaban
SD = standard deviation; SQRT, square root; QALYs = quality-adjusted life-years.
*All costs were calculated in Korean won and converted into US dollar (1 US dollar=1,000 KRW).
![]()
Incremental cost-effectiveness ratio
Cost, benefits and ICER for base-case analysis over a life-time is presented in Table 3. While the ICER for rivaroxaban was $9,707 per QALY in total AF patients, it was $7,536 per QALY in those with high stroke risk (CHA2DS2-VASc score ≥2). Figure 3 shows that rivaroxaban is more cost-effective with willingness-to-pay more than $9,707.
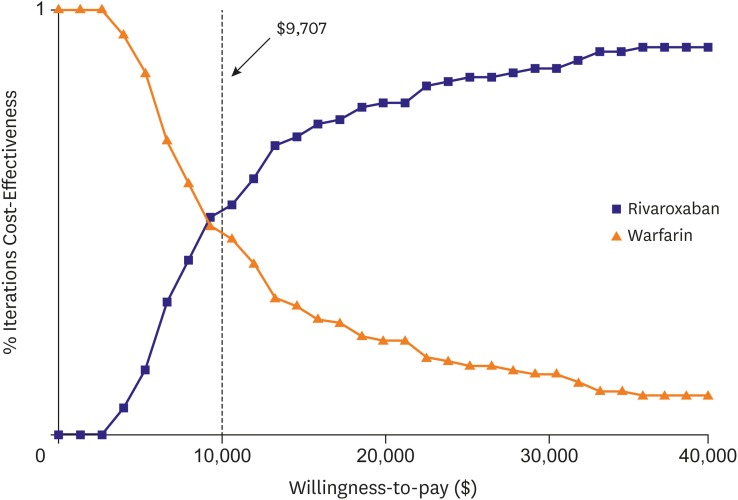
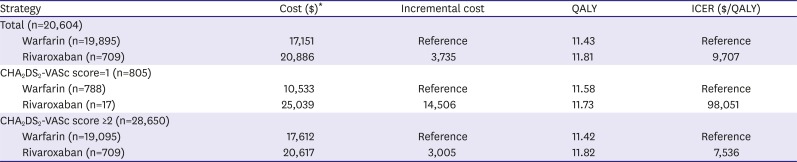
Figure 3
Changes in ICER estimates for rivaroxaban compared to warfarin with different time horizons. Employing a shorter time horizon (e.g., 1 year) results in a peak ICER of $9,707 perQALY. Vertical dotted line demarcates the $9,707 per QALY threshold.
ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
![]()
Table 3
Cost, benefits and incremental cost-effectiveness ratio for base-case analysis over a life-time
CHA2DS2-VASc = congestive heart failure, hypertension, age ≥75 (doubled), diabetes mellitus, prior stroke or transient ischemic attack (doubled), vascular disease, age 65 to 74, female; ICER = incremental cost-effectiveness ratio; QALY = quality-adjusted life-year.
*All costs were calculated in Korean won and converted into US dollar (1 US dollar=1,000 KRW).
![]()
DISCUSSION
The cost-effectiveness analysis demonstrated that rivaroxaban may be a cost-effective alternative to warfarin in Korean patients with AF. Patients with rivaroxaban needed an additional cost of $3,735, but gained an additional 0.4 QALYs over a lifetime, resulting in an ICER of $9,707 per QALY. The probability of rivaroxaban was remaining cost-effective at willingness-to-pay thresholds of $9,707 per QALY, in Monte Carlo simulation. To our knowledge, this is the first study which demonstrate that rivaroxaban is cost-effective in Korean AF patients.
Current guidelines for stroke prevention published by the 2016 European Society of Cardiology and 2014 American Heart Association/American College of Cardiology/Heart Rhythm Society recommend OAC, and NOAC as an alternative to warfarin for patients with high stroke risk factors (i.e., CHA2DS2-VASc score ≥2).17) Although the cost-effectiveness of NOAC had been identified in Korea, it was evaluated in many countries.
Dabigatran found a cost-effective alternative to warfarin in all economic models performed at a $50,000–$100,000 per QALY willingness-to-pay threshold. Dabigatran was reported to be a cost-effective alternative to warfarin in Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) trial (ICER of US $45,372 per QALY),26) and from a Canadian (Canada $10,440 per QALY) and United Kingdom health care perspective (€26,700 per QALY), respectively.27)28)
Markov model using a United States payer/Medicare perspective and a lifetime time horizon showed that the ICER for rivaroxaban was $27,498 per QALY.29) Our Markov model demonstrated that the ICER for rivaroxaban was $9,707 per QALY in total Korean AF patients. Interestingly, the cost-effectiveness was improved with $7.536 per QALY in Korean AF patients with high stroke risk (CHA2DS2-VASc score ≥2). ICER of intermediate risk (CHA2DS2-VASc score=1) group was higher than that of high-risk group. This finding might be caused by small number of rivaroxaban group with intermediate risk (n=17) rather than low cost-effectiveness of rivaroxaban. In addition, ICER cannot be calculated in low risk group because there were none who was described rivaroxaban in this group
Interestingly, the ICER for rivaroxaban calculated in Korean AF was much lower than those reported in previous studies.28)29) The favorable ICER seen in our model reflects the decreased costs and increased QALYs resulting from relatively low price of NOAC in Korea and the avoidance of ICH with rivaroxaban compared to warfarin.
A recent meta-analysis reported that assuming that the UK National Health Service is willing to pay £20,000 for each year of perfect health (one QALY), all NOACs have a positive expected incremental net benefit compared with warfarin. Apixaban 5 mg twice daily has the highest expected incremental net benefit (£7533), followed by dabigatran 150 mg twice daily (£6,365), rivaroxaban 20 mg once daily (£5,279), and edoxaban 60 mg once daily (£5,212).30) Therefore, other NOACs which is not evaluated in this study may be cost-effective in Korean patients with AF.
There are several limitations to this study. First, in this study, the use of NOACs including rivaroxaban was extremely low compared with warfarin resulting in big difference of patient numbers between warfarin and NOACs. However, study number of patients with rivaroxaban might not affect the direction of the result. Small study number usually exaggerates incidence of events and worsen the treatment effectiveness of study drugs. Therefore, small study number could act as a bias that leads the result toward the null. Our result revealed that rivaroxaban was cost-effective. Moreover, based on Markov chain Monte Carlos methods, small study size can be somehow overcome by the number of iteration. We conducted 10,000 iterations for each cycle and it is enough to compensate sample size. However, further study with larger size is needed for the size of effect, because the effectiveness of rivaroxaban could be underestimated due to small study size. Second, health events were analyzed using Korean National Health Insurance Service (KNHIS) data for three years from January 2012 to December 2014 and this data will not fully reflect the efficacy and safety of the real world. Considering that NOAC has been used in Korea since 2011 for the stroke prevention of nonvalvular AF patients, relatively early data might be included in this study. Third, as in similar models, we assumed any major bleeding would result in permanent discontinuation of rivaroxaban or warfarin and initiation of aspirin. This may not always be the case and would likely be based on individual patient factors.
In conclusion, the cost-effectiveness analysis demonstrated that rivaroxaban may be a cost-effective alternative to warfarin in Korean patients with AF. Patients with rivaroxaban needed an additional cost of $3,735, but gained an additional 0.4 QALYs over a lifetime, resulting in an ICER of $9,707 per QALY. The probability of rivaroxaban was remaining cost-effective at willingness-to-pay thresholds of $9,707 per QALY in Monte Carlo simulation. To our knowledge, this is the first study which demonstrate that rivaroxaban is cost-effective in Korean AF patients.
 XML Download
XML Download