

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The diagnosis of heart failure with preserved ejection fraction (HFpEF) is more difficult than that of heart failure with reduced ejection fraction (HFrEF) because it is not based upon objective parameter, i.e., ejection fraction (EF), but excluding other potential causes of symptom suggestive of heart failure (HF). The prevalence of HFpEF is increasing relative to HFrEF.1) Previous data suggested that HFpEF is a separate syndrome from HFrEF regarding to pathophysiology, neuroendocrine activation, aetiology, co-morbidities, and treatment response.2)3)4) Numerous drugs and device therapy have improved outcomes in patients with HFrEF, but there is no specific treatment option for HFpEF yet.5) Several drugs, already proven to be effective in HFrEF, have all failed to reduce mortality in patients with HFpEF.6)7)8) These results convincingly indicate that treatments that are effective in patients HFrEF cannot be directly applied to patients with HFpEF. The trials for beta-blocker have also reported controversial results in HFpEF. In Japanese Diastolic Heart Failure (J-DHF) trial, carvedilol did not improve a composite of cardiovascular death and unplanned hospitalization in HFpEF.9) On the other hands, a meta-analysis including observational studies showed a significant survival benefit of the use of beta-blocker for all-cause mortality, but not for HF hospitalization.10)
Recently, Lund et al.11) demonstrated that use of beta-blockers was associated with lower all-cause mortality but not with combined all-cause mortality or HF hospitalization. HF registries have raised the issue of heterogeneity, including geographic and ethnic variations. Thus, registries in different regions of the world can facilitate better understanding of HF.
The Korea Acute Heart Failure (KorAHF) registry is a prospective multicentre cohort.12) From the KorAHF registry, we investigated the hypothesis that beta-blockers are associated with reduced adverse events in patients with HFpEF.
METHODS
Study population and data collection
The KorAHF registry has been previously described.12) Briefly, 5,625 patients hospitalized for acute heart failure syndrome from 10 tertiary university hospitals throughout the country have been consecutively enrolled since March 2011 to February 2014. Detailed information on the study design and its results have been previously reported (ClinicalTrial.gov, NCT01389843).13) Patients who have signs or symptoms of HF and one of the following criteria are eligible for the study; lung congestion or objective findings of left ventricular (LV) systolic dysfunction or structural heart disease. The study protocol was approved by the Ethics Committee/Institutional Review Board at each hospital. Written informed consent was waived by the Ethics Committee/Institutional Review Board. The study complied with the Declaration of Helsinki.
Study variables and definitions
HFpEF was defined as left ventricular ejection fraction (LVEF) ≥40%. Considering the controversy of cut-off value of ejection fraction, the sensitivity analysis using another cut-off value (≥50%) was performed.14) Beta-blocker dose at baseline was standardized with carvedilol equivalents and analyzed as discrete dose groups (0, 1 to 13, 14 to 25, 26 to 50, and 51 to 200 mg daily). The following doses are equivalent to carvedilol 25 mg; acebutolol 200 mg, metoprolol 100 mg, propranolol 80 mg, atenolol 50 mg, bisoprolol 5 mg, nadolol 80 mg, and labetolol 200 mg. Dosing groups were selected on the basis of the common titration schedule for carvedilol (i.e., doubling of the dose every 2 to 4 weeks up to target doses recommended by guidelines).
The primary outcome was the all-cause mortality according to beta-blocker use.
After discharge, events including death and re-hospitalization were recorded. The follow-up data were collected by the attending physician and stored in the web-based case report form (30 days, 3 and 6 months, 1 to 5 years annually). The outcome data for patients who had not been followed up have been ascertained by a telephone interview. In addition, the outcome data for patients lost to follow-up will be collected from the National Death Records. The details were previously described.12) The independent investigators monitored data monthly. The clinical event committee was composed of independent experts in HF who have not participated in patient enrolment for this study and verified all clinical events.
Statistical analysis
Descriptive statistics were calculated to summarize characteristics, treatment, and outcomes. Missing data were handled with MICE package. Continuous variables were expressed as the mean±standard deviation and compared with t-test and analysis of variance. Categorical data are summarized as the frequency and proportion and compared with χ2 test. Survival curves were constructed using Kaplan-Meier method and compared with the log-rank test. A propensity score for treatment with beta-blocker was estimated using variables which are known to be related to both the group assignments and the outcome variables; sex, age, height, body mass index, systolic blood pressure, smoking, admission route, hypertension, diabetes, pulmonary congestion, ischemic heart disease, alcohol, cancer, atrial fibrillation (AF), chronic obstructive lung disease, chronic kidney disease, stroke, functional class, history of congestive HF, sodium, potassium, hemoglobin, EF, ischemic heart disease as aggravating factor, amiodarone, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker, loop diuretics, digoxin, warfarin, aspirin, statin, and heart rate difference from discharge to last follow up. Carvedilol, bisoprolol, metoprolol, and nebivolol were considered as ‘recommended beta-blocker’ and amosulalol, atenolol, betaxolol, bevantolol, celiprolol, propranolol, and sotalol were considered as ‘non-recommended beta-blocker.’ The propensity score matching (1:1) was performed by a nearest matching without replacement. Covariates valancing were measured by their standardized differences in means. The balance of matching was assessed by absolute standardized differences (the difference in percentage between the means for the 2 groups divided by the mutual standard deviation). It is considered that pre-treatment variable balancing can be achieved if the absolute standardized difference of means is less than 10%. The Cox proportional hazards regression model was used to compare the clinical outcomes as beta-blocker use in the unmatched and propensity score matched cohort. For the heterogeneity of beta-blocker effect, subgroup analysis was performed. Statistical analyses were performed using R 3.3.1 (R Foundation, Vienna, Austria).15)16) R packages of survival and MatchIt were used to conduct the survival analysis and to construct the matched cohort, respectively. All reported p values are 2-sided, and p values of <0.05 were considered statistically significance.
RESULTS
Patient characteristics
Of 5,625 patients enrolled in the KorAHF registry, 2,087 patients had HFpEF: 979 received and 1,108 did not receive beta-blockers at the discharge. After propensity score matching, there were 979 pairs. Baseline characteristics are shown for the unmatched and matched HFpEF cohort in Table 1. In the unmatched HFpEF cohort, the mean age was similar (71 years) and female were more often (60.5% in no beta-blocker, 55.2% in beta-blocker, p=0.016). Patients discharged on beta-blocker had higher body mass index, more pulmonary congestion, and received more angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) than those without beta-blocker. After matching the baseline characteristics became well balanced between the groups (Table 1).
Table 1
Baseline characteristics
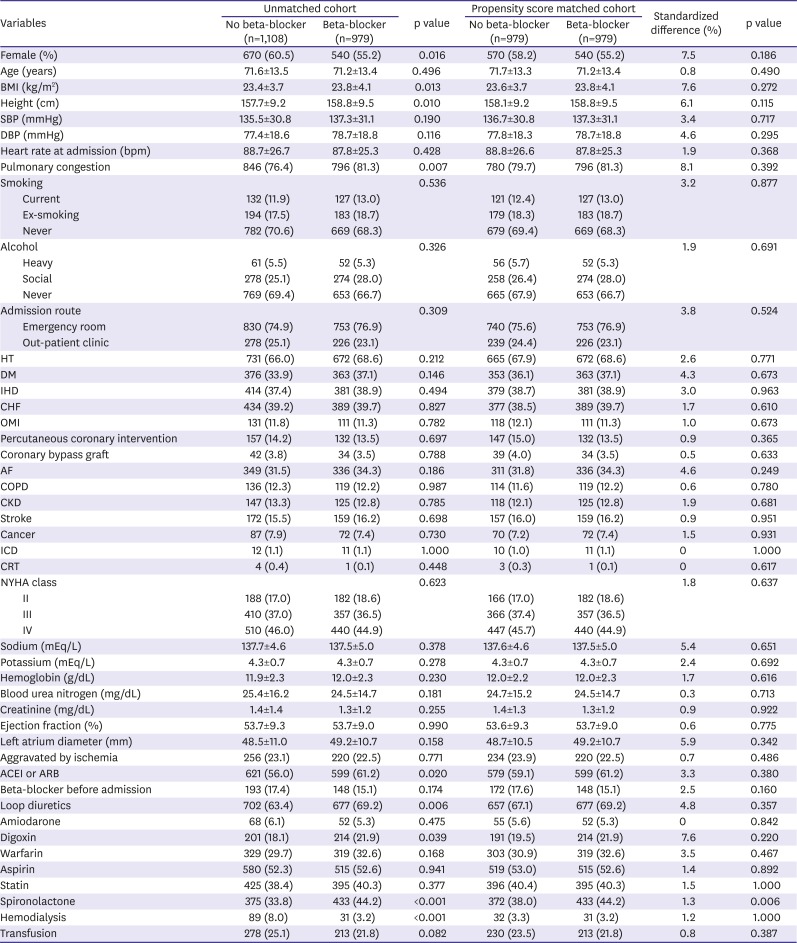
Values are presented as number (%) or mean±standard deviation. Standardized difference between the means for the 2 groups divided by the mutual standard deviation.
ACEI = angiotensin converting enzyme inhibitor; AF = atrial fibrillation; ARB = angiotensin receptor blocker; BMI = body mass index; bpm = beat per minute; CHF = congestive heart failure; CKD = chronic kidney disease; COPD = chronic obstructive pulmonary; disease; CRT = cardiac resynchronization therapy; DBP = diastolic blood pressure; DM = diabetes mellitus; HT = hypertension; ICD = implantable cardioverter-defibrillator; IHD = ischemic heart disease; NYHA = New York Heart Association; OMI = old myocardial infarction.
Main outcomes in patients with heart failure with preserved ejection fraction
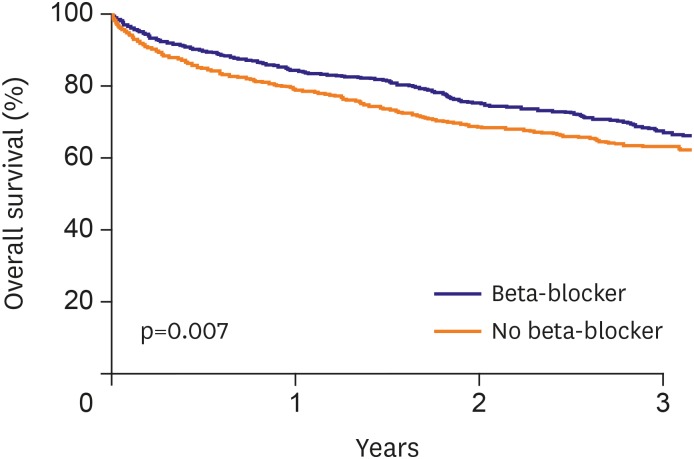
During a median follow-up duration of 807 days (interquartile range, 498–1,122 days). Main outcomes were summarized Figure 1 and Table 2. After adjustment for significant covariates, beta-blocker at discharge was associated with a lower all-cause death (hazard ratio [HR], 0.80; 95% confidence interval [CI], 0.68–0.93). However, there was no significant difference in the risk of rehospitalization for HF (HR, 1.03; 95% CI, 0.85–1.27). In the propensity score matched population, beta-blocker at discharge was associated with a reduced risk of all-cause death (HR, 0.78; 95% CI, 0.66–0.91), as well. The post-discharge rehospitalization did not differ between those with or without beta-blockers (HR, 1.03; 95% CI, 0.83–1.27). The sensitivity analysis using another cut-off value demonstrated the consistent results (Supplementary Tables 1 and 2)

Subgroup analysis
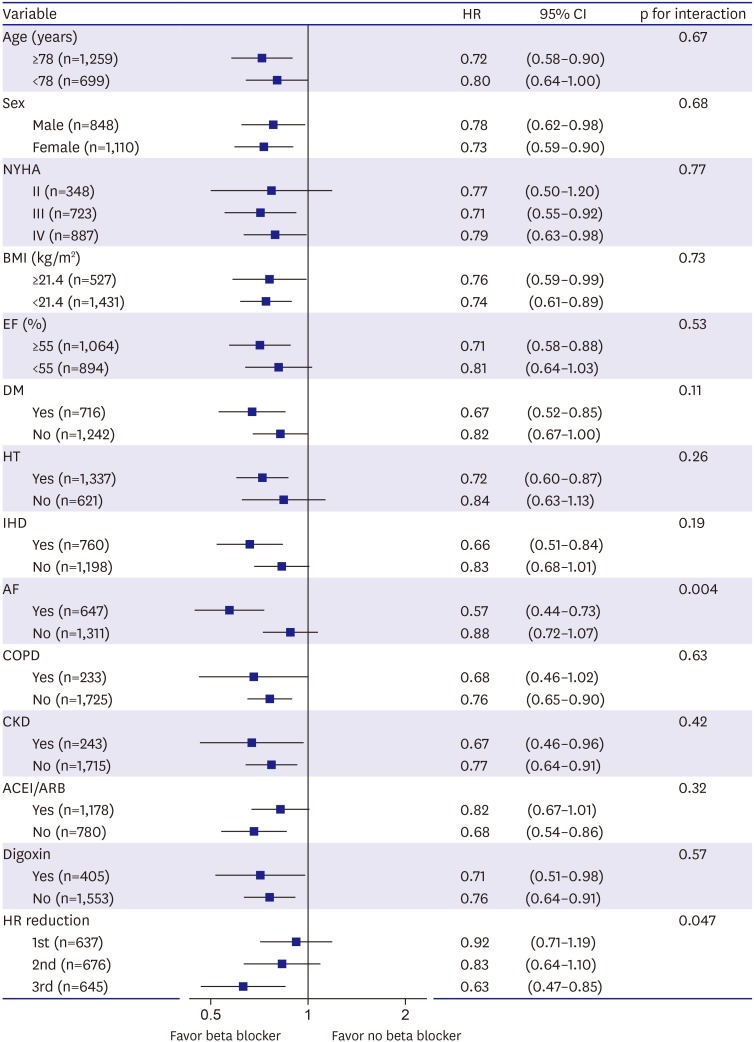
The reduction of all-cause death associated with beta-blocker was consistent with the subgroups with the exception of AF and heart rate reduction during follow up period (Figure 2). In patients with AF, beta-blocker at discharge was significantly associated with the reduction of all-cause mortality (HR, 0.57; 95% CI, 0.44–0.73), but it was not in patients without AF (HR, 0.88; 95% CI, 0.72–1.07). As more heart reduction were achieved during follow period, beta-blocker was significantly associated with lower all-cause mortality (3rd tertile, 16.0±10.4 per minutes reduction, HR, 0.63; 95% CI, 0.47–0.85).
Figure 2
Interactions and HRs for all-cause death in the matched cohorts among patients with heart failure with preserved ejection fraction.
ACEI = angiotensin converting enzyme inhibitor; AF = atrial fibrillation; ARB = angiotensin receptor blocker; BMI = body mass index; CI = confidence interval; CKD = chronic kidney disease; COPD = chronic obstructive pulmonary disease; DM = diabetes mellitus; EF = ejection fraction; HR = hazard ratio; HT = hypertension; IHD = ischemic heart disease; NYHA = New York Heart Association.
Pattern of beta-blocker use and outcomes in the unmatched cohort
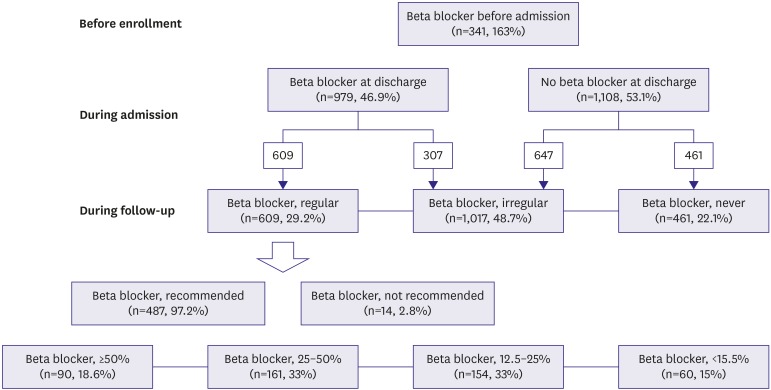
A broad distribution of beta-blocker prescription was observed in this registry (Figure 3). A 39.4% of patients in the unmatched HFpEF cohort had history of congestive HF (Table 1) and 16.3% of patients had already received beta-blocker before enrollment. Among patients discharged on beta-blocker at discharge, 62.2% of patients (n=609) received beta-blocker consistently during follow-up period but 37.8% of patients (n=370) did irregularly. Given beta-blockers were mostly recommended one (97.2%). Among patients who received beta-blocker regularly, only 18.6% of patients received 50% or more target dose. The prescription of regular and recommended beta-blocker was associated with all-cause mortality respectively. After using Cox proportional hazards models, the HR for all-cause mortality was 0.77 (95% CI, 0.64–0.93) lower for patients with regular beta-blocker and 0.62 (95% CI, 0.47–0.82) lower for patients with recommended beta-blocker respectively. However, the dose of beta-blocker was not associated with all-cause mortality (HR, 0.84; 95% CI, 0.60–1.18).
DISCUSSION
The effect of beta-blocker in patients with HFpEF is controversial. In our study we could show that, beta-blocker at discharge was associated with reduced all-cause death, but not with rehospitalization in patients with HFpEF after adjustment of significant covariates and propensity-score matching. Our findings were also strengthened by additional analysis for the pattern and outcomes of beta-blocker prescription after discharge.
Since Bavishi et al.17) reported firstly that propranolol decreased mortality in patients with HFpEF and old myocardial infarction, the results of subsequent studies were controversial. J-DHF study was the first and only prospective randomized trial to investigate the effect of carvedilol in patients with HFpEF (Table 3). Contrast to our results, J-DHF study failed to show the reduction of all-cause death as well as the primary outcome, a composite of cardiovascular death and unexplained hospitalization for HF. This difference may have several explanations. In J-DHF study, both stable chronic HF patients as well as acute HF patients were enrolled, whereas our study population included only hospitalized acute HF patients. So, beta-blocker initiation and titration could be considered more safely in our study. Furthermore, in J-DHF study the expected number of events was not achieved due to poor enrollment and had high loss to follow-up rate.9) All-cause death occurred in just 39 patients (15.9%) among J-DHF study, but in 702 patients (33.6%) in our cohort. In addition, patients with New York Heart Association (NYHA) class II were 72.2%, which was too high compared usual HF cohort as well as our cohort, so the results should be interpreted with caution. Similar with our results, Lund et al.11) have demonstrated that use of beta-blocker was associated with lower all-cause death but not with HF rehospitalization (Table 3). However, the risk reduction of beta-blocker was of smaller magnitude compared our results. Geographic and ethnic differences in the response of beta-blocker have been suggested.18)19)20) A higher prevalence of central obesity and insulin resistance in Korean, are likely to have a higher sympathetic activity.21) It may benefit from the use of a beta-blocker for the treatment of hypertension and HF.19) In prEserveD left ventricular ejectIon fraction chronic heart Failure with ivabradine studY (EDIFY) trial, further heart rate reduction by ivabradine was not associated with improved surrogate outcomes.22) The discrepancy with our results could be explained. First, the patients in EDIFY trial had chronic HF and stable heart rate in baseline compared with our patients. In our registry, heart rate at discharge were variable (38–160 bpm) and some patients were discharged with tachycardia (>90 bpm, 15% of HFpEF cohort). It means that tachycardia could be significant cause of HF and heart rate reduction would be beneficial. Second, majority of patients in EDIFY already had beta-blocker and the goal of EDIFY was the additional benefit of ivabradine. There is no patient who had ivabradine in our HFpEF cohort. European investigators recently reported that beta-blocker was not effective in reducing mortality in patients with HFpEF (≥50% of EF).23) However, in this meta-analysis, the number of patients with preserved EF (≥40%) was only half of our cohort and patients who had more than 50% of EF was only 314 (2.2% of whole patients). Duration of follow-up was much shorter (1.3 year) than that of our cohort. As Cleland et al.23) acknowledged at the paper, there were too few patients and events to draw any conclusions in patients with more preserved LVEF. Second, all of our patients were diagnosed as acute HF. The baseline characteristics including ethnicity was different. Ischemia as etiology was about 90% in Cleland's paper but only 23% in our patients. Female was majority of our patients.
Table 3
Comparison of previous studies
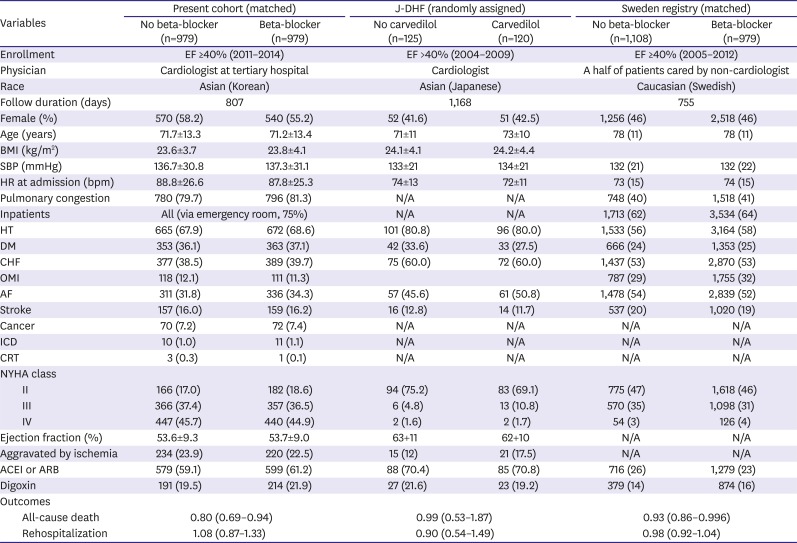
Values are presented as number (%) or mean±standard deviation.
ACEI = angiotensin converting enzyme inhibitor; AF = atrial fibrillation; ARB = angiotensin receptor blocker; BMI = body mass index; bpm = beat per minute; CHF = congestive heart failure; CRT = cardiac resynchronization therapy; DBP = diastolic blood pressure; DM = diabetes mellitus; HR = hazard ratio; HT = hypertension; ICD = implantable cardioverter-defibrillator; J-DHF = Japanese Diastolic Heart Failure; NYHA = New York Heart Association; OMI = old myocardial infarction; SBP = systolic blood pressure.
We identified AF as subgroup was superior to beta-blocker treatment with regard to efficacy. A sophisticated meta-analysis reported that beta-blocker led to a significant reduction in all-cause death in patients with sinus rhythm, but not in patients with AF.24) However, as the author acknowledged, patient with HFpEF accounted for only 1.8% of the pooled population. Although the interaction was not significant (p for interaction=0.10) in the Swedish HF registry, subgroup with AF had also more benefit from beta-blocker compared patients with sinus rhythm. More convincing comment requires the accumulation of large evidence for the efficacy of beta-blocker according to the rhythms status in patients with HFpEF.
There are several limitations. First, rehospitalization was collected by medical record review or telephone interview. So, it would be not easy to adjudicate and missed in case of admission to other hospital. Less duration of follow up for rehospitalization would be affected compared with that for death which were collected from the National Death Records. Second, noncardiovascular comorbidity is more common in HFpEF. Third, the side effects of beta-blocker, that are bradycardia, hypotension, and syncope, would offset the effective of beta-blocker.
In conclusion, in Korean patients with HFpEF, use of beta-blockers is associated with reduced all-cause death but not with reduced rehospitalization.
 XML Download
XML Download