

 PDF
PDF ePub
ePub Citation
Citation Print
Print



CARDIOGENIC SHOCK
Cardiogenic shock (CS) is a pathophysiological state of inadequate tissue perfusion and oxygenation to maintain homeostasis, resulting from primary cardiac dysfunction. Depending on the duration and severity of the state, CS frequently results in profound multi-organ dysfunction and death. Cardiogenic shock complicates between 5% and 15% of ST-elevation myocardial infarction (STEMI) cases. Although survival improved steadily over a few decades, primarily due to early revascularisation,1) contemporary 30-day mortality has plateaued at approximately 50%.2)3) A variety of percutaneous circulatory assist strategies can be deployed in the cardiac catheter laboratory, which allow cardiologists to rapidly initiate potentially life-saving treatment. However, major challenges remain, including the difficulty in matching an individual patient's pathophysiology to the available support strategy and a precarious balance of potential benefit against significant risk.
Cardiogenic shock is classically considered to develop when the indexed cardiac output falls below a critical threshold of 2.2 L/min/m2. Whilst direct measurement of cardiac output is available, it is not routinely used in catheterisation labs. In the absence of direct measurements, commonly used diagnostic criteria are:
-
1) Sustained hypotension
-
2) Elevated left ventricular (LV) filling pressures and absence of hypovolaemia
-
3) Signs of impaired organ perfusion
Whilst hypotension is traditionally considered a hallmark of shock and is inevitably listed as an inclusion criterion in most clinical trials of shock, it should be appreciated that CS may develop with minimally depressed or normal blood pressure (BP). This is primarily due to the compensatory processes that are triggered by hypotension, including peripheral vasoconstriction. Even in patients who are stable at the outset, shock can develop during revascularisation procedures from prolonged ischaemia, as a consequence of reperfusion injury or through iatrogenic mechanisms. In the cardiac catheter laboratory, the onset of CS can be insidious and difficult to identify, as markers of end-organ hypoperfusion are not always easy to detect in sedated and draped patients. Right heart catheter measurements can be vital in establishing the diagnosis quickly and should be encouraged, as right atrial pressure estimation will help to exclude hypovolaemia and pulmonary artery pressure trends can provide an early marker of rising LV end diastolic pressure.2) When the diagnosis of CS is made, and various treatments instituted, serial lactate levels can be useful in assessing the early response to these strategies, alongside mixed central venous oxygen saturations and right heart catheter measurements where indicated.3)
The first priority in managing CS is identification and treatment of the underlying pathology. Where CS complicates acute myocardial infarction (AMI), early culprit-lesion revascularisation significantly improves mortality in the first 30 days, an effect which is maintained to 10 years of follow up.1) Recent evidence suggests that the strategy of culprit-vessel only intervention reduces early all-cause mortality when compared to multi-vessel percutaneous coronary intervention (PCI); the risks of acute multi-vessel intervention therefore outweighs benefit in these circumstances4) and should not routinely be performed. The ability to deliver emergent, high quality revascularisation, most frequently with PCI but with coronary artery bypass grafting (CABG) if necessary, is a pre-requisite for cardiogenic shock centres.
MECHANICAL CIRCULATORY SUPPORT: GENERAL PRINCIPLES
Mechanical circulatory support (MCS) describes a range of technologies used in the treatment of CS. The broad treatment goals of MCS therapy are:
1) Maintain organ perfusion (including cardiac perfusion)
2) Support cardiac output
3) Optimise cardiac recovery
Three main methods for MCS are available in the catheter lab environment–intra-aortic balloon pump (IABP), direct LV unloading via percutaneous LV assist devices (pLVAD) and veno-arterial extra-corporeal membrane oxygenation (VA-ECMO). Direct left atrial unloading (the TandemHeart device) has not been widely adopted and so is not covered in this article.
In most cases these devices will be introduced from the femoral vessels. As an increasing proportion of coronary procedures are performed from radial access, cardiologists experience with femoral access is declining, and the use of adjunctive techniques for safe femoral access, including femoral angiography from the radial or contralateral femoral and/or ultrasound guidance, should be routine. In cases where a bail-out device strategy is anticipated, the preparatory insertion of small gauge (4–5 Fr) arterial or venous sheaths can be considered at the start of the procedure. These can facilitate rapid MCS deployment in deteriorating situations but carry some vascular risk of their own. In elective or semi-elective settings where the patient is known to have peripheral vascular disease, involving vascular surgeons may permit safer vascular access, whether via alternative routes (e.g. axillary artery,5)6) transcaval access7)) or preparatory intervention on the peripheral vessels.
Early consideration must be given to futility and the exit strategy, should the patient deteriorate despite MCS. The amount of information available and timeframe in which these decisions must be made varies dramatically depending on the clinical situation, but the early involvement of multi-disciplinary team should be considered, as allowed by the acuity of the situation.
SPECIFIC MECHANICAL CIRCULATORY SUPPORT DEVICES
Intra-aortic balloon pump
The IABP is the most widely used form of MCS, and was first introduced to clinical practice in the 1960s.8) It is usually inserted retrogradely via the femoral artery and positioned in the proximal descending aorta, 2 cm distal to the left subclavian artery. Insertion can either be via a sheath, or sheathless, with evidence of lower rates of vascular complications using the sheathless method.
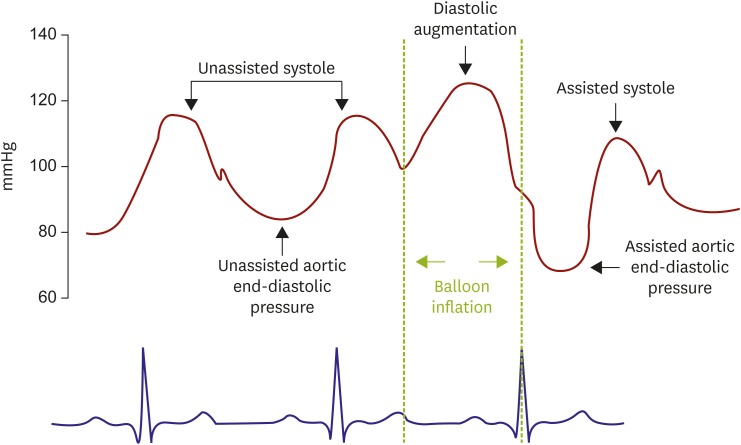
The technique hinges on counterpulsation, whereby the balloon inflates during diastole and deflates rapidly during systole. Inflation is usually timed from the aortic pressure tracing (with the onset of diastole marked by the dicrotic notch) and deflation from a surface electrocardiograph (ECG) (with the R-wave taken to indicate the onset of electrical systole) but both can be gated to the pressure tracing in emergency situations or if the ECG quality is inadequate to trigger deflation reliably.
Figure 1 shows the physiological effects of the IABP over two consecutive cardiac cycles–the first cycle without counterpulsation and the second with counterpulsation. The balloon inflates in diastole, resulting in an augmentation of diastolic pressure and diastolic pressure-time index. This increases coronary perfusion pressure, with an additional accelerating wave of coronary flow in diastole and increased overall flow where coronary autoregulation is exhausted.9) Subsequent deflation in systole reduces aortic end-diastolic pressure and systolic pressure in the next cardiac cycle–this is reflected in a reduced tension time index, an important marker of LV myocardial oxygen demand. The reduction in aortic pressure in systole reduces cardiac afterload and LV end diastolic pressure and wall tension are also reduced, further aiding coronary blood flow and myocardial perfusion.
Augmentation is dependent on native cardiac contractility–the IABP will have little effect if stroke volume is very low (<30 mL) or high (>100 mL). Augmentation is also significantly impaired by tachycardia and irregular heart rhythms due to a relative shortening of diastole in comparison to systole.
The IABP therefore has potential physiological benefits in both supporting reducing myocardial work and maintaining coronary perfusion. It is available in the majority of catheter labs and can be deployed rapidly, with a relatively low risk profile (of all MCS devices, the IABP requires the smallest vascular access and therefore has the lowest risk of vascular complications). The effect of IABP on cardiac output is modest; at optimal performance increases of 0.5 L/min can be expected,10) so it's physiological benefits are in improving the balance of myocardial supply with oxygen demand, predominantly through increased supply.11) Not all patients will exhibit a haemodynamic response to IABP counterpulsation. Our data show the most significant haemodynamic effects are seen in those with an acute coronary syndrome (ACS) or greater extent of coronary disease, as well as those undergoing more complex PCI.11) Effective revascularisation also reduces the benefit of IABP on coronary perfusion, as aortic pressure will be directly transmitted to the distal coronary bed without pressure loss through the epicardial arteries.
Percutaneous left ventricular assist device (Impella)
A number of pLVAD have been developed for utilisation in the catheter lab environment. Of these, the Impella (Abiomed, Danvers, MA, USA), has seen the most widespread adoption.
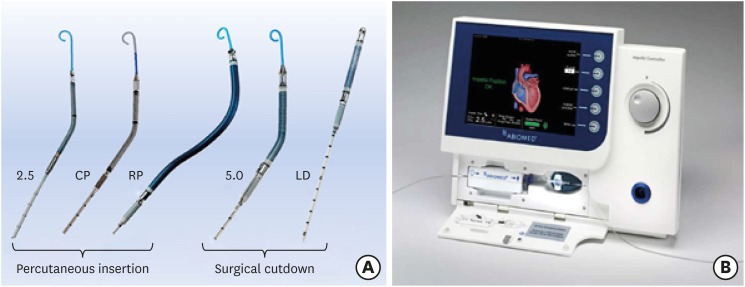
The Impella is a microaxial pump mounted on a 9 Fr pigtail catheter which sits in the LV apex. The pump's action unloads blood through an inlet in the left ventricle. This passes through the catheter and is expelled via an outlet into the aorta. Flow through the device is continuous (i.e. non-pulsatile) and is controlled by a dedicated console. The catheter is continuously flushed through and heparinisation must be maintained throughout to prevent catheter or motor thrombosis. Three catheters are available for percutaneous insertion (the Impella 2.5 [12 Fr, maximum flow 2.5 L/min], CP [14 Fr, 3.5 L/min] and RP [for right ventricular, RV unloading into the pulmonary artery, 23Fr, 4.0L/min]) and two require surgical access (Impella 5.0 and LD [both 21 Fr, 5.0 L/min], the 5.0 via femoral cut-down and arteriotomy and the LD via open-chest procedures) (Figure 2, Panel A). The 2.5, CP and RP devices are therefore more suitable for acute use in the catheter lab environment.
The Impella provides significant augmentation of cardiac output, with positive effects on a number of LV haemodynamic indices. The LV unloading reduces LV end-diastolic pressure and LV wall tension, with corresponding reductions in LV work and myocardial oxygen demand.12) This reduces pulmonary capillary wedge pressure and RV afterload. Assessing the net total increase in cardiac output with Impella is challenging, as flow through the device is offset by a reduction in native cardiac output and a degree of aortic regurgitation induced by the catheter. A single case report initially reported global cardiac output using themodilution13) reported an increase of 24% of native output (5.95 to 7.38 L/min) with the 2.5 L device. In ISAR-SHOCK, a small (n=25), randomised trial comparing the haemodynamic effects of IABP and Impella 2.5 in patients with CS, cardiac output increased from 3.16 L/min to 4.12 L/min in the Impella group, compared to 3.46 L/min to 3.67 L/min in the IABP group.12) This increase in cardiac output resulted in an increase in mean aortic pressure and systemic organ perfusion, with significant reductions in serum lactate over time. There was no significant difference between lactate levels between the IABP and Impella, however. Data on coronary perfusion are conflicting–some reports indicate decreased hyperaemic microvascular resistance and increased coronary flow with Impella use,14) whilst our own data indicates no change from baseline conditions.11) In either circumstance, the significant reduction in myocardial work results in improvement in relative supply/demand ratio.11)14)
The larger-bore access required for Impella results in a higher risk profile than the IABP, with notably higher rates of limb ischaemia and major bleeding in comparative trials to date (30% vs. 8% in the IMPRESS trial).10) Haemolysis is another often-recognised complication. Whilst many centres now have significant experience with the device, it lacks the long-established experience and familiarity most clinicians have with the IABP; this may impact both the speed of deployment as a bail-out device and ability to troubleshoot issues such as device migration and haemolysis. Acute cessation of device support due to thrombosis is rare but has been reported. The best method of vascular closure is yet to be established–plug closure devices are not currently available for >8 Fr arteriotomies and suture-based techniques are not suitable for devices that may remain in situ for several days. Closure devices for larger arteriotomies are currently being rolled out, predominantly for transcatheter aortic valve implantation procedures, but will be well suited to meet these needs.15)
The Impella RP is designed for use in patients with cardiogenic shock either arising from isolated RV failure or more frequently with primary LV pathology with consequent RV failure. Right ventricular dysfunction has been defined by central venous pressure (CVP) >10 mmHg, CVP/PCWP >0.63, pulmonary artery pulsatility index <2.0 and RV stroke work index <450 mmHg·mL/m2. It has been observed to occur in around 1/3 of patients presenting in CS following an AMI and is associated with higher 30-day mortality (hazard ratio vs. no RV dysfunction 1.46 (95% confidence interval 1.03–2.07).16) Observational data demonstrate favourable acute haemodynamic effects of the device either alone or in combination with an LV assist device, termed BiPella17) where both devices are percutaneous.18)19) Randomised outcome data are keenly awaited.
Veno-arterial extra-corporeal membrane oxygenation
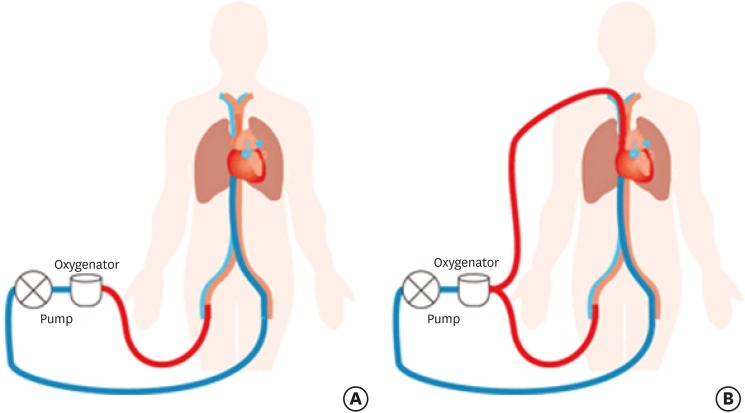
Of the currently available methods of MCS, Veno-arterial extra-corporeal membrane oxygenation (VA-ECMO) provides the greatest amount of circulatory support at the greatest cost in both vascular access and resource. It consists of two large-bore cannulae, one venous drainage cannula (up to 22 Fr) placed in the inferior atrio-caval junction and an arterial return cannula (up to 17 Fr) in the descending aorta (Figure 3).20) Cannulation may be peripheral (via the femoral arteries and veins) or central (via an open chest and direct cannulation of the right atrium and aorta). A membrane oxygenator and pump sit between the drainage and return cannulae and provide blood oxygenation and cardiac output. As with the Impella, flow is non-pulsatile. VA-ECMO provides high flow volumes (typically 50–70 mL/kg/min, up to 100 mL/kg/min) and good oxygenation, adequate to maintain systemic perfusion in profound cardio-respiratory failure or cardiac arrest. The delivery of VA-ECMO requires experienced intensivists in collaboration with cardiologists, cardiac surgeons, perfusionists and vascular surgeons. Access to these devices is currently (and appropriately) restricted to centres with specialist expertise in the management of CS. The numbers of such centres is increasing as interest in improving cardiogenic shock outcomes continues.
Figure 3
Venoarterial (A) and veno-venous arterial extra-corporeal membrane oxygenation circuit configurations (B).
The use of VA-ECMO comes with high-cost and a significant risk of complications, and careful consideration must be given to appropriate patient selection. As with all mechanical support devices, complications rates improve with experience and adequate patient volume. The most common issues encountered are haematological and vascular, including thrombosis, bleeding (including a high incidence of intracranial bleeding), haemolysis, stroke and limb ischaemia. Thrombosis within the ECMO circuit is infrequent but may result in an abrupt cessation of support and/or systemic embolisation which may be fatal.
Whilst removing blood from the venous system and returning oxygenated blood to the aorta results in effective systemic perfusion, overly-high flow rates may significantly decrease cardiac preload and increase afterload, resulting in LV dilatation, stasis and ultimately, thrombosis. The extent to which these effects impair the recovery of cardiac function are open for debate and further investigation. Therapeutic strategies in case of LV dilataton and stasis include implantation of an IABP or Impella, or atrial septostomy and drainage. The optimal strategy has yet to be defined by a prospective trial, but observational evidence supports further study.21)22)23) Recovery of native cardiac output whilst on ECMO may result in competitive flow between the heart and ECMO system, with de-oxygenated blood perfusing the cerebral circulation: this is termed “Harlequin Syndrome.” Lung ischaemia may develop and cannula infection may be fatal in a dependent patient.
EVIDENCE FOR USE IN CARDIOGENIC SHOCK
Intra-aortic balloon pump
Early observational studies of the routine use of IABP in CS suggested significant benefit, a position which was supported by meta-analyses through the early era of reperfusion with thrombolysis for AMI.24) The benefit in these situations appears to be in preventing the development of shock in the face of prolonged, untreated or partially treated ischaemia. Following the roll-out of primary PCI, providing rapid and effective relief from ischaemia and reversal of the resultant shock, the role of the IABP in shock has become more uncertain, with evidence pointing to no overall benefit or even net harm from routine use.24)
The IABP-SHOCK II trial provides the only randomised evidence for the role of IABP in the management of CS complicating AMI.25) This multicentre, open-label trial randomised 600 patients with AMI and CS to either IABP or no IABP (control). The balloon pump was inserted after PCI in the vast majority of cases. The trial inclusion criteria required patients to have cardiogenic shock due to an AMI with planned early revascularisation, preferably by PCI (69% STEMI, 31% NSTEMI). The diagnosis of CS was made using the diagnostic criteria listed above. Around half of patients required resuscitation prior to randomisation. Multi-vessel coronary disease was present in 77% of patients. The mean time between the development of CS and randomisation was 2:17 hours and IABP support was continued for an average of 3 days. Catecholamine use was near-ubiquitous, in 90% of patients. A high proportion (up to 80%) of screened patients underwent randomisation, indicating little risk of recruitment bias.
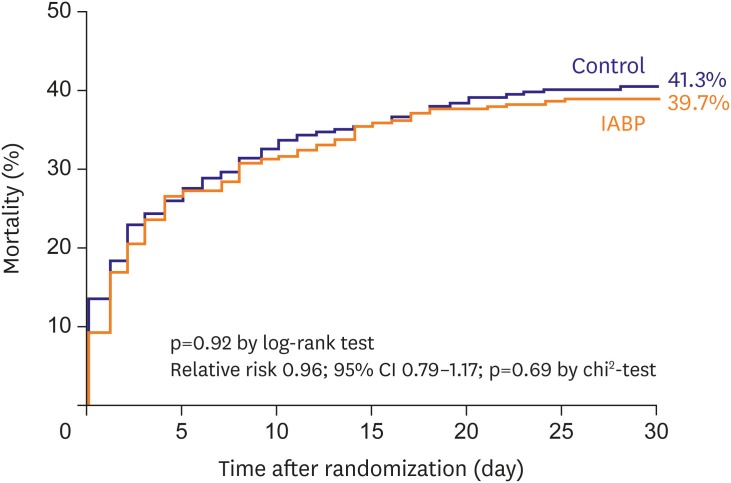
The primary end-point (a composite of all-cause mortality or severe renal failure requiring renal replacement therapy) occurred by 30 days in 37.5% of patients in the IABP arm and 41.3% in the control arm, with no significant difference between groups (P=0.92, Figure 4). On long-term follow up, no benefit was demonstrated at 6 months, 12 months26) or 6 years.27) No difference in IABP effectiveness was observed in STEMI vs. NSTEMI patients or with any comorbid conditions or severity of hypotension at presentation. Patients <50 years of age appeared to have a better outcome with IABP, but the numbers in this group were small (n=70).
Figure 4
Time-to-event curves through 30 days after randomisation for the primary endpoint of all-cause mortality in the IABP-SHOCK II trial. Event rates represent Kaplan-Meier estimates.
CI = confidence interval; IABP = intra-aortic balloon pump.
The trial was broadly successful in delivering a reliable answer to the clinical question posed. Mean patient age was 70 years, older than the average age seen in most ACS trials but representative of the population presenting in CS. The observed mortality rate was similar to contemporary registries. The authors noted no difference between arms in markers of systemic inflammation or serum lactate, suggesting the modest augmentation of cardiac output provided by the IABP failed to impact systemic haemodynamics and preserve organ perfusion. It is worth noting that IABP use was safe, with no significant increase observed in bleeding or peripheral ischaemic complications between the two groups.
The main criticisms of the trial have been the rate of crossover, which occurred in 10% of patients assigned to the control group: the majority were protocol violations (i.e. for reasons not permitted in the trial protocol). There are reasons to believe that these crossovers had little impact, in that these patients were similar in demographics and haemodynamics to the rest of the cohort, and most occurred in five trial centres (of a total of 37). Following publication of the IABP-SHOCK II results, comments were also raised as to whether the results might have differed if insertion had been performed prior to PCI; 4.3% of the IABP group did not undergo balloon pump insertion, the majority because they died before intended insertion. It has been suggested that counterpulsation during the primary PCI procedure may reduce peri-procedural deterioration due to further ischaemia or reperfusion injury. There is, however, no evidence to support this hypothesis and one can easily conceive that, had the majority of patients undergone insertion pre-PCI and the trial results been identical, arguments would be made that delaying PCI had resulted in the observed lack of difference.
The routine use of the IABP in patients with CS has subsequently been downgraded from a class I to a class III indication in American and European guidelines.28)29) The lack of evidence for routine use, however, should not be considered an absolute rejection of the IABP for MCS in specific situations. A recent large registry study examined outcomes in patients with AMI and CS treated with- or without- IABP, stratified by successful or unsuccessful primary PCI (defined as final TIMI flow grade ≤1).30) The data suggested a reduction in 30-day mortality from 89% to 82% when IABP was utilised. Whilst confounding cannot be excluded in this observational dataset (one might expect IABP use to be lower futile cases), these outcomes are in keeping with data from the pre-revascularisation era. IABP use should therefore be considered where effective revascularisation cannot immediately be delivered or where the device's effects may ameliorate severe or prolonged peri-procedural ischaemia. The SEMPER FI trial, currently in recruitment and due to complete in December 2018, will address this hypothesis.31) Common such situations include patients awaiting primary revascularisation with CABG or with acute mitral regurgitation or ventricular septal defects.
Impella
From the initial introduction of Impella into clinical practice, large quantities of registry data have been published reporting the outcomes of patients in cardiogenic shock. A very large registry (15,259 patients) was recently published from 1010 centres in the USA.32) Shock was defined as any systolic BP <90 mmHg or need for vasopressors in patients with either ST or non-ST elevation MI. The mean age of patients treated in the registry was 64 years. Most patients (61%) had support from the Impella CP, with a third receiving Impella 2.5 support. The mean duration of support was 3.78 days. Survival rates were 53% at explant, with no data provided on in-hospital or 30-day mortality. A sub-registry of 479 patients who were followed up in more detail had a 30-day survival of only 40%, despite 73% being alive at explant. There was a suggestion that higher-volume centres had lower mortality rates, but due to the observational nature of this research cannot attribute this success to greater experience with the device, particularly without detailed data to address confounding.
The lack of robust randomised data for Impella has not prevented rapid expansion in use of the devices in many regions. Several trials were stopped early due to poor recruitment. The IMPRESS trial is the only completed randomized controlled trial (RCT) of the Impella for patient outcomes in CS to date. It was a small, open-label, randomised trial comparing prognostically important outcomes between Impella CP to IABP in mechanically ventilated patients with an AMI complicated by CS undergoing PCI.33) Forty-eight patients were enrolled and randomised 1:1 between arms. As with IABP-SHOCK II the assigned MCS device was deployed either prior-to or after angioplasty at the operators' discretion. The primary outcome was 30-day all-cause mortality, with a pre-defined secondary endpoint of mortality at 6 months.
The patient population was younger than those observed in IABP-SHOCK II (58 years vs. 70 years) and much more likely to have had a cardiac arrest prior to randomisation (92% vs. 50%). Primary PCI was successful in all cases. There was no difference in the primary outcome (46% vs. 50%, P=0.92), with no difference in mortality at 6 months. As mentioned earlier in this article, adverse events occurred more frequently in the Impella group. As with IABP-SHOCK II, there was a high rate of crossover (12.5%) from IABP to Impella.
Considered together with the results of IABP-SHOCK II, the IMPRESS results suggest no benefit to routine use of the Impella CP in patients presenting in CS.
Several factors prevent this trial providing the definitive answer on pLVAD use in CS. As would be predicted in a ventilated population, the patients were clearly in severe, established shock at the time of randomisation, with a mean resuscitation time of 24 minutes. Mean blood lactate was 8.3 mmol/L and mean arterial pressure was 66 mmHg despite ubiquitous treatment with catecholamines or inotropes. In this situation the 30-day mortality rates are a relatively impressive advertisement for modern supportive care and primary PCI, when compared to historical figures. In many cases, however, the patient's outcomes were likely to be pre-determined and outwith the influence of the device; it is notable that 46% of deaths were due to irreversible neurological injury, significantly more than those due to refractory CS (29%). The trial was also significantly underpowered to detect smaller but important differences, though the absence of any signal of benefit makes simply increasing the sample size may be unlikely to have a significant effect on the outcome.
Another RCT of Impella CP support in CS is ongoing. The DAN-SHOCK trial has been recruiting across three centres in Denmark since 2012.34) With a sample size of 360 patients, recruitment is expected to complete in 2022. Patients are randomised between conventional circulatory support and Impella CP support for at least 48 hours. Whilst the absence of a standardised support strategy in the control arm may make interpretation somewhat challenging, the trial is powered to assess a primary outcome of all-cause mortality at 6 months and should provide more definitive data on the role of LV offloading in CS.
Isolated RV dysfunction is a relatively rare but under-recognised cause of cardiogenic shock, with a similar mortality to primary left ventricular dysfunction. The RECOVER-RIGHT registry enrolled 30 patients in CS, 18 of whom had previously received a surgical LVAD and 12 with RV dysfunction following surgery or AMI.18) Thirty-day survival was 73%.
Veno-arterial extra-corporeal membrane oxygenation
The substantial flow volumes provided by VA-ECMO make it an exciting option in patients where maintaining systemic organ perfusion is key. Current avenues of exploration include the use of VA-ECMO in severe CS with multi-organ dysfunction and as an adjunct to cardio-pulmonary resuscitation in refractory cardiac arrest in selected patients (eCPR). A number of registry studies have been published reporting local outcomes in many regions, with many focussed on identifying predictors of outcome. A number of these studies report mortality rates well below the median for previous trials in shock, however it should be borne in mind that these are highly selected populations.35) Despite enthusiasm and increasing adoption of the technique, no RCT evidence exists to support the use of VA-ECMO in shock.
The EURO-SHOCK trial, an EU-funded randomised trial of the use of VA-ECMO vs. standard care in patients with CS, is in recruitment.36) Should ECMO prove to be of benefit, further work on the optimal timing and systems for deployment in the catheter lab environment will be required.
Strategy selection
The data above present clinicians involved in managing CS with a challenge; the current evidence base does not support routine use of any form of MCS, but mortality remains high. The evidence of physiological improvement in patients with MCS suggests that some, carefully selected patients may benefit should complications be minimised, but this has not been reflected in RCTs to date. Whilst there is often a desire to compare devices in side-by-side trials, the differing physiological effects and risk profile of each device favour considering them as complementary technologies with overlapping but individual places on the pathway of carefully selected patients. Table 1 summarises the general principles in managing cardiogenic shock at our institution at present, based on our appraisal of the current evidence data.
Table 1
Optimal MCS strategies stratified by presentation with shock
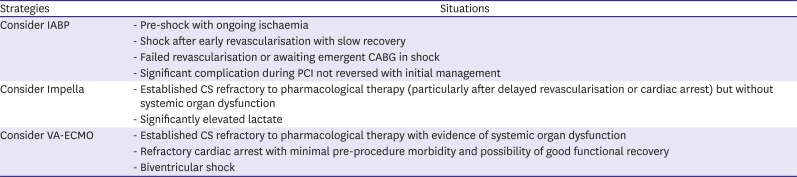
Routine use of MCS is not encouraged in cardiogenic shock. Emergent revascularisation should be performed in ACS. Consider risk of futility and exit-strategy if deteriorating despite support throughout.
ACS = acute coronary syndrome; CABG = coronary artery bypass grafting; CS = cardiogenic shock; ECMO = extra-corporeal membranous oxygenation; MCS = mechanical circulatory support; PCI = percutaneous coronary intervention.
MECHANICAL CIRCULATORY SUPPORT AS A BRIDGING THERAPY AFTER SHOCK
When used to treat patients in cardiogenic shock, the expected period of percutaneous MCS is 3–7 days. It is expected that any improvement in cardiac function will have manifested by this stage, and decisions can be made regarding device removal, treatment withdrawal or escalation to surgical ventricular assist device (VAD) or cardiac transplant in appropriate patients. The prolonged bedrest and risk of infection associated with femoral access were considered prohibitive to more longer durations of support.
Recent experience, however, indicates a novel role for percutaneous MCS; medium-term support for those who have suffered cardiogenic shock and not recovered. This may be a bridge to recovery (where cardiac function is expected to recover in the longer term, commonly in severe acute myocarditis), surgical VAD implantation or transplantation. The latter has seen particular interest in decompensated chronic heart failure, where there is a desire to avoid a pre-transplant sternotomy. When a longer duration of use is anticipated, alternative routes of access are the left axillary artery (percutaneous) or the subclavian (usually via an externalised graft). These routes permit patient ambulation and reduce device associated infections. Specific IABP and Impella catheters and insertion kits are in development for this indication.
PREVENTING SHOCK: MECHANICAL CIRCULATORY SUPPORT IN HIGH-RISK PERCUTANEOUS CORONARY INTERVENTION
Percutaneous MCS devices can also be used prevent shock developing during a high-risk PCI procedure where the patient is haemodynamically stable at the outset. The goals of MCS therapy in these circumstances are subtly different to when used in shock:
1) Reduce myocardial oxygen demand to prevent peri-procedural ischaemia
2) Support cardiac output to prevent the development of shock
3) Permit complete coronary revascularisation
In these circumstances the decision whether to use MCS, and which device to use, should be guided by the risk of developing peri-procedural ischaemia or shock. Whilst factors such as severe left ventricular systolic dysfunction, an ACS presentation, significant previous infarction and a large myocardial area at risk have been shown to increase the likelihood of complications, most high-risk procedures can be safely delivered without MCS. In the Balloon-Pump assisted Coronary Intervention Study (BCIS-1, IABP in high-risk PCI) randomised controlled trial, almost 90% of enrolled patients had no evidence of periprocedural ischaemia or hypotension. This must be balanced against the risks of device-associated complications, which may often exceed 10%. Multiple protocols and decision-making tools exist, but their predictive accuracy remains limited and their efficacy is not supported by RCT evidence.39) The quantification of these risks and identification of patients at exceptionally high risk of complications is a key priority for researchers interested in high-risk PCI.
Intra-aortic balloon pump in high-risk percutaneous coronary intervention
BCIS-1 was the first randomised controlled trial of routine elective IABP use to prevent shock in high-risk PCI.40)41) The trial was open-label and recruited 301 patients across 17 UK centres. These patients were selected for a high risk of procedural complications (mean left ventricular ejection fraction 23.6%, mean BCIS-1 Jeopardy Score 10.4). They were randomised 1:1 to either pre-PCI IABP therapy or no planned IABP therapy, with bailout IABP insertion permitted in defined situations (refractory hypotension, pulmonary oedema or procedural complications). The primary outcome was in-hospital major adverse cardiac events (MACE), with secondary outcomes of procedural complications and 6-month mortality. The primary outcome occurred in 15.6% of patients, with no significant difference between groups (p=0.85). However, fewer procedural complications occurred with elective IABP use (1.3% vs. 10.7%, p<0.001), an outcome that was partially offset by greater rates of major or minor bleeding (19% vs. 11%) and access site complications (3% vs. 0%) respectively.
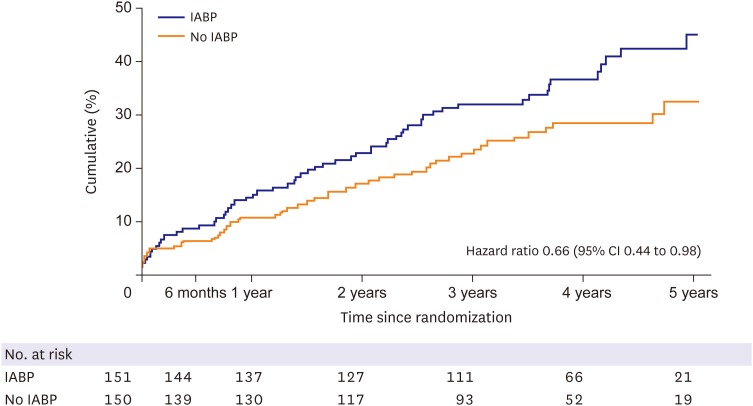
As noted above, bail-out IABP use was required in 12% of patients in the trial due to acute haemodynamic instability or prolonged ischaemia. It is unknown, therefore, what the outcomes of these patients would have been had the device not been available. This trial limitation means there is insufficient evidence to abandon the device in high-risk PCI altogether. Indeed, an initially unplanned extension study followed these patients for mortality in the long-term (mean 51 months), at which point there was a 34% relative risk reduction in all-cause mortality in the elective IABP group (Figure 5).40) We hypothesise that the presence of the IABP may reduce the occurrence of subclinical but prognostically important peri-procedural infarctions; there was no identifiable difference in the quality or amount of revascularisation achieved in either arm.
Figure 5
All cause mortalities in the BCIS-1 trial. Reproduced with permission from Perera D, et al. Long-term mortality data from the Balloon Pump-Assisted Coronary Intervention Study (BCIS-1): a randomized, controlled trial of elective balloon counterpulsation during high-risk percutaneous coronary intervention. Circulation 2013;127:207-212.40)
CI = confidence interval; IABP = intra-aortic balloon pump.
Where acute coronary occlusion occurs during PCI, either due to no-reflow or dissection, augmenting coronary flow may be of benefit if vessel patency cannot be immediately re-established. The rapidity and ease of deployment of the IABP, and its physiological effects make it highly suitable for bail-out use and for ameliorating ischaemia by driving coronary supply during periods of stunning. A bail-out strategy appears effective in these situations. Building on the BCIS-1 data, prophylactic IABP insertion may still be considered in high-risk PCI on a case-by-case basis where there is considered to be exceptionally high risk of ischaemic complications; these cases should all be discussed within the Heart Team before committing to a specific strategy.
Impella in high-risk percutaneous coronary intervention
As with shock, the role of Impella in high-risk PCI has received significant attention in registries but little high-quality, randomised data exist. The only RCT to date was the PROTECT II trial.42) (Figure 6). This open-label trial randomised 452 patients undergoing high-risk PCI to either Impella 2.5 or IABP. The primary outcome was 30-day composite MACE, consisting of death, MI, stroke/transient ischemic attack and repeat revascularisation. No difference was seen, with primary endpoints occurring in 35.1% of the Impella group vs. 40.1% of the IABP group.
Figure 6
Kaplan-Meier curves of major adverse events to 90 days. (A) Intent-to-treat population. (B) Per protocol population. IABP indicates intra-aortic balloon pump. Reproduced with permission from O'Neill WW, et al. A prospective, randomized clinical trial of hemodynamic support with Impella 2.5 versus intra-aortic balloon pump in patients undergoing high-risk percutaneous coronary intervention: the PROTECT II study. Circulation 2012;126:1717-1727.42)
IABP = intra-aortic balloon pump.
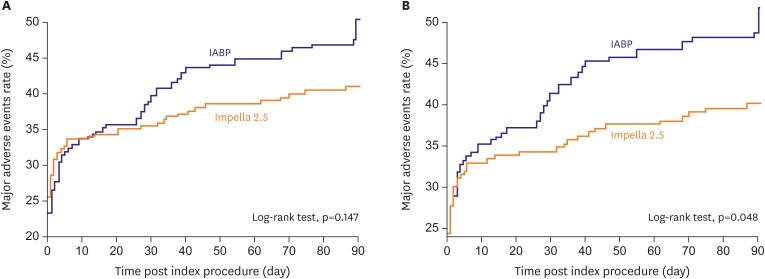
A number of sub-analyses were produced which showed a trend towards benefit with Impella, including as-treated analysis and one with the exclusion of the first patient in each centre43) (justified by the authors due to the learning curve of a new device) but these should be considered in context of the main trial outcome.
Veno-arterial extra-corporeal membrane oxygenation
Given the invasive nature and possible acutely deleterious effects of ECMO on cardiac function, it highly unlikely to be suitable for prophylactic use in high-risk PCI. Bail-out use may be considered if significant peri-procedural complications occur which prove irretrievable with standard measures. Such cases should be the exception, however, and careful consideration of the reversibility of the underlying condition and possibility of futility, even in emergent situations.
SUMMARY
The outlook for patients diagnosed with CS remains poor. Despite initial improvements related to primary PCI and supportive care, mortality has plateaued over the last 15–20 years. MCS devices have long been considered to improve the physiological condition of patients with shock. The routine use of these devices has not shown significant benefit in randomised trials. Given the lack of other options for treating shock, the use of novel MCS devices is increasing rapidly worldwide. Future trials should focus less on comparing devices, and more on personalised support strategies based on individual haemodynamics, coronary anatomy, LV function and morphology and vascular considerations.
 XML Download
XML Download