

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
MATERIALS AND METHODS
Search Strategy and Eligibility Criteria
Data Extraction and Study Endpoints
Quality Assessment
Data Synthesis and Statistical Analysis
RESULTS
Literature Selection

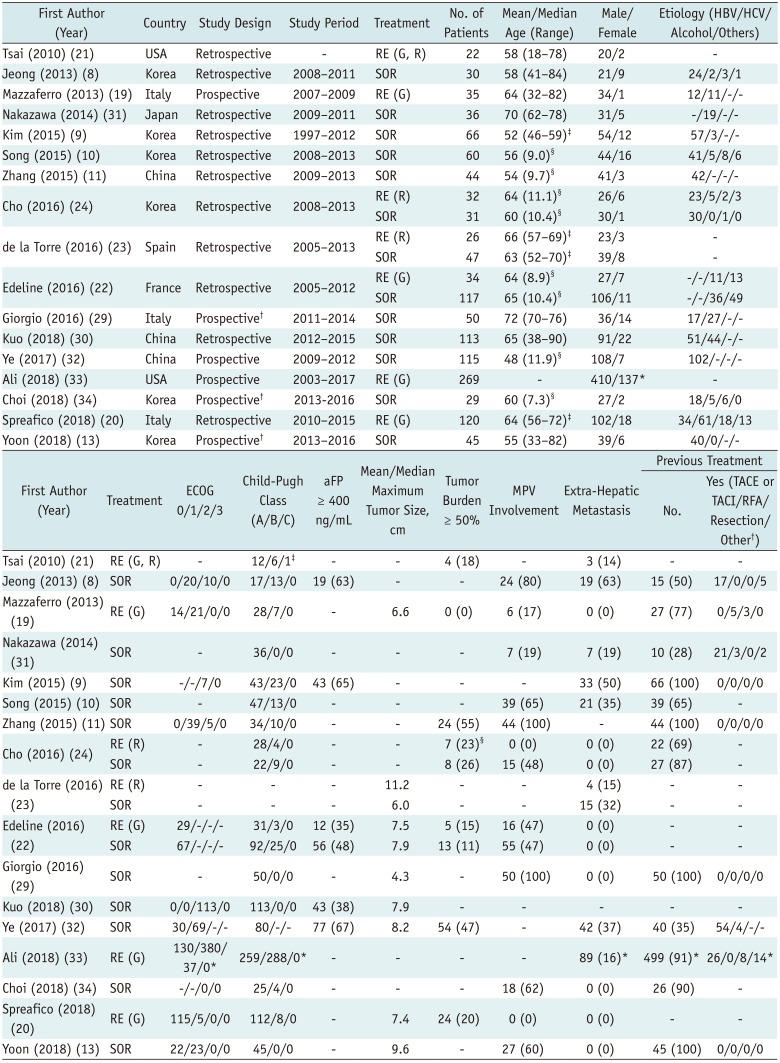
Study Characteristics
Table 1
Study Characteristics
| First Author (Year) | Country | Study Design | Study Period | Treatment | No. of Patients | Mean/Median Age (Range) | Male/Female | Etiology (HBV/HCV/ Alcohol/Others) |
|---|---|---|---|---|---|---|---|---|
| Tsai (2010) (21) | USA | Retrospective | - | RE (G, R) | 22 | 58 (18–78) | 20/2 | - |
| Jeong (2013) (8) | Korea | Retrospective | 2008–2011 | SOR | 30 | 58 (41–84) | 21/9 | 24/2/3/1 |
| Mazzaferro (2013) (19) | Italy | Prospective | 2007–2009 | RE (G) | 35 | 64 (32–82) | 34/1 | 12/11/-/- |
| Nakazawa (2014) (31) | Japan | Retrospective | 2009–2011 | SOR | 36 | 70 (62–78) | 31/5 | -/19/-/- |
| Kim (2015) (9) | Korea | Retrospective | 1997–2012 | SOR | 66 | 52 (46–59)‡ | 54/12 | 57/3/-/- |
| Song (2015) (10) | Korea | Retrospective | 2008–2013 | SOR | 60 | 56 (9.0)§ | 44/16 | 41/5/8/6 |
| Zhang (2015) (11) | China | Retrospective | 2009–2013 | SOR | 44 | 54 (9.7)§ | 41/3 | 42/-/-/- |
| Cho (2016) (24) | Korea | Retrospective | 2008–2013 | RE (R) | 32 | 64 (11.1)§ | 26/6 | 23/5/2/3 |
| SOR | 31 | 60 (10.4)§ | 30/1 | 30/0/1/0 | ||||
| de la Torre (2016) (23) | Spain | Retrospective | 2005–2013 | RE (R) | 26 | 66 (57–69)‡ | 23/3 | - |
| SOR | 47 | 63 (52–70)‡ | 39/8 | - | ||||
| Edeline (2016) (22) | France | Retrospective | 2005–2012 | RE (G) | 34 | 64 (8.9)§ | 27/7 | -/-/11/13 |
| SOR | 117 | 65 (10.4)§ | 106/11 | -/-/36/49 | ||||
| Giorgio (2016) (29) | Italy | Prospective† | 2011–2014 | SOR | 50 | 72 (70–76) | 36/14 | 17/27/-/- |
| Kuo (2018) (30) | China | Retrospective | 2012–2015 | SOR | 113 | 65 (38–90) | 91/22 | 51/44/-/- |
| Ye (2017) (32) | China | Prospective | 2009–2012 | SOR | 115 | 48 (11.9)§ | 108/7 | 102/-/-/- |
| Ali (2018) (33) | USA | Prospective | 2003–2017 | RE (G) | 269 | - | 410/137* | - |
| Choi (2018) (34) | Korea | Prospective† | 2013-2016 | SOR | 29 | 60 (7.3)§ | 27/2 | 18/5/6/0 |
| Spreafico (2018) (20) | Italy | Retrospective | 2010–2015 | RE (G) | 120 | 64 (56–72)‡ | 102/18 | 34/61/18/13 |
| Yoon (2018) (13) | Korea | Prospective† | 2013–2016 | SOR | 45 | 55 (33–82) | 39/6 | 40/0/-/- |
| First Author (Year) | Treatment | ECOG 0/1/2/3 | Child-Pugh Class (A/B/C) | aFP ≥ 400 ng/mL | Mean/Median Maximum Tumor Size, cm | Tumor Burden ≥ 50% | MPV Involvement | Extra-Hepatic Metastasis | Previous Treatment | |
|---|---|---|---|---|---|---|---|---|---|---|
| No. | Yes (TACE or TACI/RFA/Resection/Other†) | |||||||||
| Tsai (2010) (21) | RE (G, R) | - | 12/6/1‡ | - | - | 4 (18) | - | 3 (14) | - | - |
| Jeong (2013) (8) | SOR | 0/20/10/0 | 17/13/0 | 19 (63) | - | - | 24 (80) | 19 (63) | 15 (50) | 17/0/0/5 |
| Mazzaferro (2013) | RE (G) (19) | 14/21/0/0 | 28/7/0 | - | 6.6 | 0 (0) | 6 (17) | 0 (0) | 27 (77) | 0/5/3/0 |
| Nakazawa (2014) | SOR (31) | - | 36/0/0 | - | - | - | 7 (19) | 7 (19) | 10 (28) | 21/3/0/2 |
| Kim (2015) (9) | SOR | -/-/7/0 | 43/23/0 | 43 (65) | - | - | - | 33 (50) | 66 (100) | 0/0/0/0 |
| Song (2015) (10) | SOR | - | 47/13/0 | - | - | - | 39 (65) | 21 (35) | 39 (65) | - |
| Zhang (2015) (11) | SOR | 0/39/5/0 | 34/10/0 | - | - | 24 (55) | 44 (100) | - | 44 (100) | 0/0/0/0 |
| Cho (2016) (24) | RE (R) | - | 28/4/0 | - | - | 7 (23)§ | 0 (0) | 0 (0) | 22 (69) | - |
| SOR | - | 22/9/0 | - | - | 8 (26) | 15 (48) | 0 (0) | 27 (87) | - | |
| de la Torre (2016) (23) | RE (R) | - | - | - | 11.2 | - | - | 4 (15) | - | - |
| SOR | - | - | - | 6.0 | - | - | 15 (32) | - | - | |
| Edeline (2016) (22) | RE (G) | 29/-/-/- | 31/3/0 | 12 (35) | 7.5 | 5 (15) | 16 (47) | 0 (0) | - | - |
| SOR | 67/-/-/- | 92/25/0 | 56 (48) | 7.9 | 13 (11) | 55 (47) | 0 (0) | - | - | |
| Giorgio (2016) (29) | SOR | - | 50/0/0 | - | 4.3 | - | 50 (100) | 0 (0) | 50 (100) | 0/0/0/0 |
| Kuo (2018) (30) | SOR | 0/0/113/0 | 113/0/0 | 43 (38) | 7.9 | - | - | - | - | - |
| Ye (2017) (32) | SOR | 30/69/-/- | 80/-/- | 77 (67) | 8.2 | 54 (47) | - | 42 (37) | 40 (35) | 54/4/-/- |
| Ali (2018) (33) | RE (G) | 130/380/ | 259/288/0* | - | - | - | - | 89 (16)* | 499 (91)* | 26/0/8/14 |
| Choi (2018) (34) | SOR | -/-/0/0 | 25/4/0 | - | - | - | 18 (62) | 0 (0) | 26 (90) | - |
| Spreafico (2018) (20) | RE (G) | 115/5/0/0 | 112/8/0 | - | 7.4 | 24 (20) | 0 (0) | 0 (0) | - | - |
| Yoon (2018) (13) | SOR | 22/23/0/0 | 45/0/0 | - | 9.6 | - | 27 (60) | 0 (0) | 45 (100) | 0/0/0/0 |
*Data only available for entire study population only, †Randomized controlled trial, ‡Interquartile range, §Standard deviation. G = glass, HBV = hepatitis B virus, HCV = hepatitis C virus, R = resin, RCT= randomized controlled trial, RE = radioembolization, SOR = sorafenib
Data are shown as n (%). *Data available for entire study population only, †Including radiotherapy and liver transplantation, ‡Information was not available in three patients, §Information was not available in one patient. aFP = alpha-fetoprotein, ECOG = Eastern Cooperative Oncology Group, MPV = main portal vein, RFA = radiofrequency ablation, TACE = transcatheter arterial chemoembolization, TACI = transcatheter arterial chemotherapy infusion
![]()
Study Quality
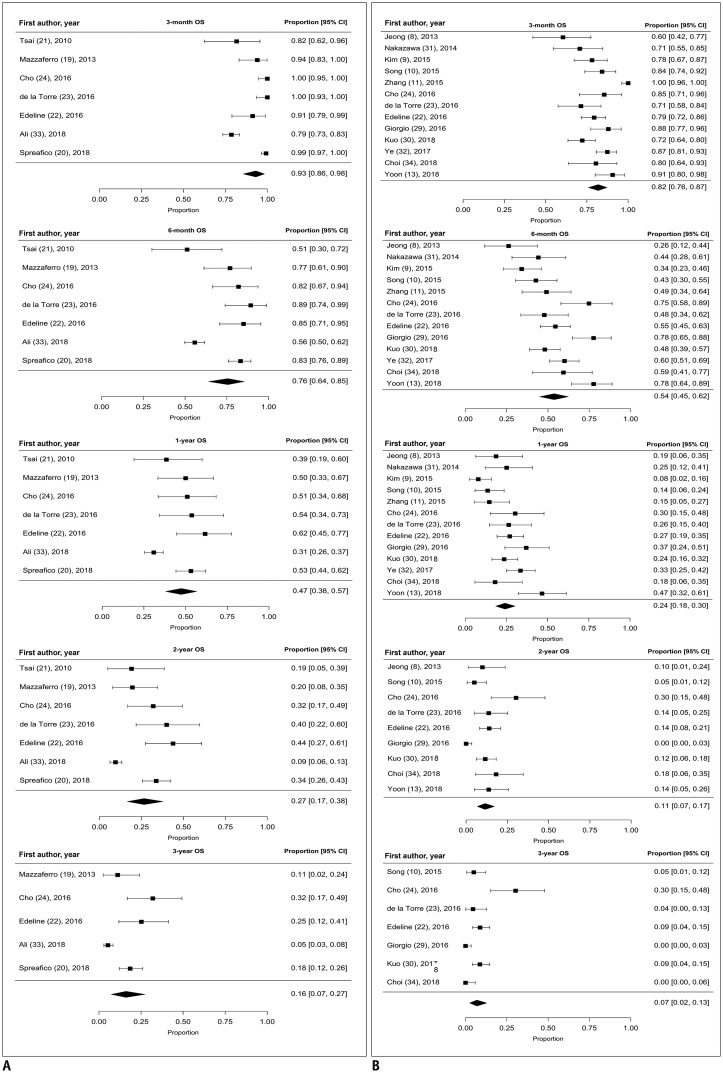
OS: Meta-Analysis
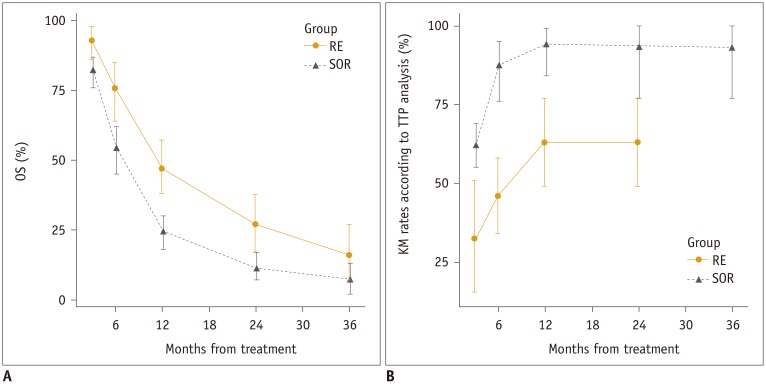
TTP: Meta-Analysis

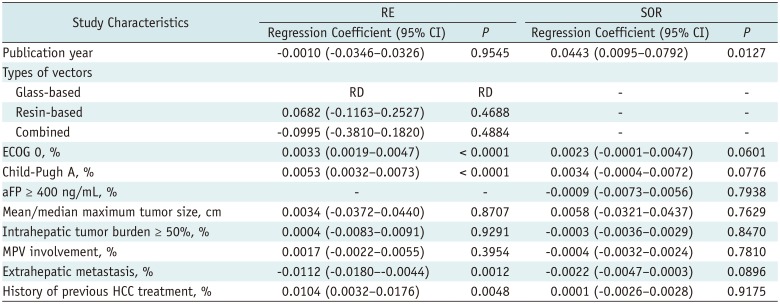
Meta-Regression Analysis for 1-Year OS
Table 2
Summary of Meta-Regression Analyses of 1-Year Overall Survival Data
![]()
AEs
Table 3
Summary of Adverse Events Following RE
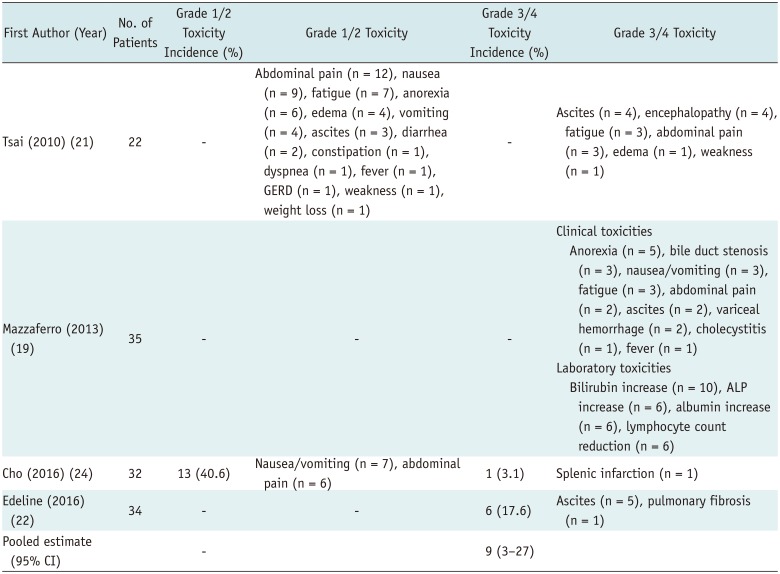
| First Author (Year) | No. of Patients | Grade 1/2 Toxicity Incidence (%) | Grade 1/2 Toxicity | Grade 3/4 Toxicity Incidence (%) | Grade 3/4 Toxicity |
|---|---|---|---|---|---|
| Tsai (2010) (21) | 22 | - | Abdominal pain (n = 12), nausea (n = 9), fatigue (n = 7), anorexia (n = 6), edema (n = 4), vomiting (n = 4), ascites (n = 3), diarrhea (n = 2), constipation (n = 1), dyspnea (n = 1), fever (n = 1), GERD (n = 1), weakness (n = 1), weight loss (n = 1) | - | Ascites (n = 4), encephalopathy (n = 4), fatigue (n = 3), abdominal pain (n = 3), edema (n = 1), weakness (n = 1) |
| Mazzaferro (2013) (19) | 35 | - | - | - | Clinical toxicities Anorexia (n = 5), bile duct stenosis (n = 3), nausea/vomiting (n = 3), fatigue (n = 3), abdominal pain (n = 2), ascites (n = 2), variceal hemorrhage (n = 2), cholecystitis (n = 1), fever (n = 1) Laboratory toxicities Bilirubin increase (n = 10), ALP increase (n = 6), albumin increase (n = 6), lymphocyte count reduction (n = 6) |
| Cho (2016) (24) | 32 | 13 (40.6) | Nausea/vomiting (n = 7), abdominal pain (n = 6) | 1 (3.1) | Splenic infarction (n = 1) |
| Edeline (2016) (22) | 34 | - | - | 6 (17.6) | Ascites (n = 5), pulmonary fibrosis (n = 1) |
| Pooled estimate (95% CI) | - | 9 (3–27) |
Adverse events were defined and categorized in accordance with NCI-CTCAE version 5.0; meta-analytic pooled estimates were based on inverse variance method for calculating weights with random-effects model. ALP = alkaline phosphatase, GERD = gastroesophageal reflux disease, NCI-CTCAE = National Cancer Institute-Common Terminology Criteria for Adverse Events
![]()
Table 4
Summary of Adverse Events Associated with SOR Treatment
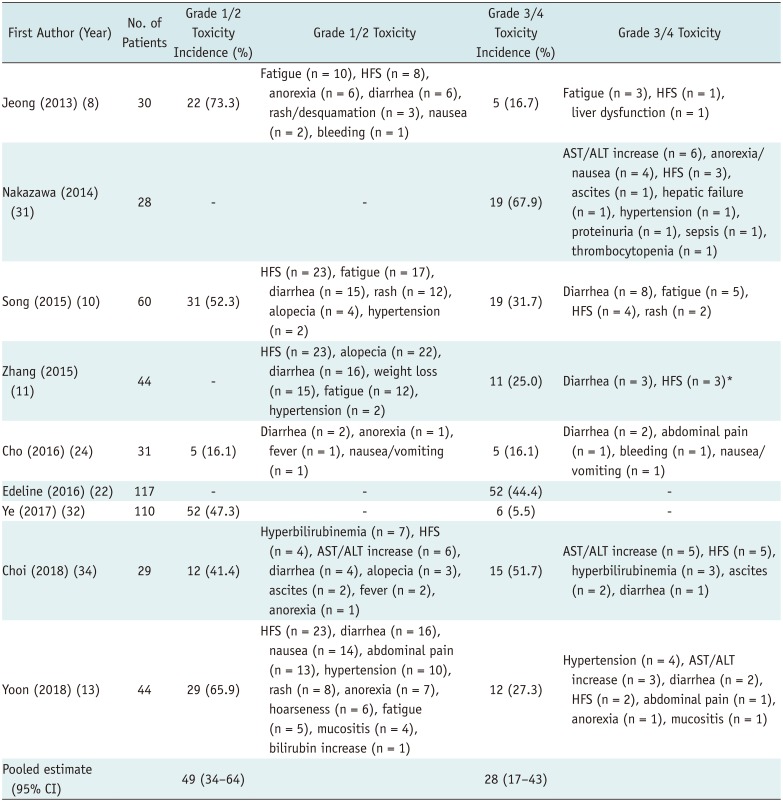
| First Author (Year) | No. of Patients | Grade 1/2 Toxicity Incidence (%) | Grade 1/2 Toxicity | Grade 3/4 Toxicity Incidence (%) | Grade 3/4 Toxicity |
|---|---|---|---|---|---|
| Jeong (2013) (8) | 30 | 22 (73.3) | Fatigue (n = 10), HFS (n = 8), anorexia (n = 6), diarrhea (n = 6), rash/desquamation (n = 3), nausea (n = 2), bleeding (n = 1) | 5 (16.7) | Fatigue (n = 3), HFS (n = 1), liver dysfunction (n = 1) |
| Nakazawa (2014) (31) | 28 | - | - | 19 (67.9) | AST/ALT increase (n = 6), anorexia/nausea (n = 4), HFS (n = 3), ascites (n = 1), hepatic failure (n = 1), hypertension (n = 1), proteinuria (n = 1), sepsis (n = 1), thrombocytopenia (n = 1) |
| Song (2015) (10) | 60 | 31 (52.3) | HFS (n = 23), fatigue (n = 17), diarrhea (n = 15), rash (n = 12), alopecia (n = 4), hypertension (n = 2) | 19 (31.7) | Diarrhea (n = 8), fatigue (n = 5), HFS (n = 4), rash (n = 2) |
| Zhang (2015) (11) | 44 | - | HFS (n = 23), alopecia (n = 22), diarrhea (n = 16), weight loss (n = 15), fatigue (n = 12), hypertension (n = 2) | 11 (25.0) | Diarrhea (n = 3), HFS (n = 3)* |
| Cho (2016) (24) | 31 | 5 (16.1) | Diarrhea (n = 2), anorexia (n = 1), fever (n = 1), nausea/vomiting (n = 1) | 5 (16.1) | Diarrhea (n = 2), abdominal pain (n = 1), bleeding (n = 1), nausea/vomiting (n = 1) |
| Edeline (2016) (22) | 117 | - | - | 52 (44.4) | - |
| Ye (2017) (32) | 110 | 52 (47.3) | - | 6 (5.5) | - |
| Choi (2018) (34) | 29 | 12 (41.4) | Hyperbilirubinemia (n = 7), HFS (n = 4), AST/ALT increase (n = 6), diarrhea (n = 4), alopecia (n = 3), ascites (n = 2), fever (n = 2), anorexia (n = 1) | 15 (51.7) | AST/ALT increase (n = 5), HFS (n = 5), hyperbilirubinemia (n = 3), ascites (n = 2), diarrhea (n = 1) |
| Yoon (2018) (13) | 44 | 29 (65.9) | HFS (n = 23), diarrhea (n = 16), nausea (n = 14), abdominal pain (n = 13), hypertension (n = 10), rash (n = 8), anorexia (n = 7), hoarseness (n = 6), fatigue (n = 5), mucositis (n = 4), bilirubin increase (n = 1) | 12 (27.3) | Hypertension (n = 4), AST/ALT increase (n = 3), diarrhea (n = 2), HFS (n = 2), abdominal pain (n = 1), anorexia (n = 1), mucositis (n = 1) |
| Pooled estimate (95% CI) | 49 (34–64) | 28 (17–43) |
*Details of adverse events were incomplete in study. Adverse events were defined and categorized in accordance with NCI-CTCAE version 5.0; meta-analytic pooled estimates were based on inverse variance method for calculating weights with random-effects model. ALT = alanine aminotransferase, AST = aspartate aminotransferase, HFS = hand-foot syndrome
![]()
 XML Download
XML Download