

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ovarian cancer (OC) is the fifth cause of cancer related death in the United States and Europe [1]. Residual disease following surgery is the strongest independent prognostic factor for survival [2]. To achieve a complete resection (CR), multi-visceral pelvic and abdominal surgery is often necessary [345].
Neoadjuvant chemotherapy (NACT) followed by interval debulking surgery (IDS) has lately emerged as an alternative strategy to primary debulking surgery (PDS) [67] and its use is increasing worldwide [8]. The expectation on NACT is to shrink the tumour, decrease the surgical morbidity and increase the CR rate, however, these advantages were not consistently confirmed in the setting of ultra-radical surgery [91011]. Unfortunately, the 2 large clinical randomized trials published reported a CR rate of 17% and 19.4% after PDS and 39% and 51.2% following IDS, respectively [67]. Also, they reported a very low rate of bowel resection (8.7% and 15.5%) and multi-visceral surgery. Thus, it is difficult to infer from these studies the peri-operative morbidity of women needing multi-visceral surgery and rectosigmoid resection (RSR) during IDS.
To achieve CR multi-visceral resections, including bowel resection are still needed in 30%–40% of the patients undergoing IDS with an alleged increased surgical morbidity [1213].
Not surprisingly, gastrointestinal complications are the most common adverse events, accounting for 9%–26% of the overall morbidity in PDS and IDS [14151617]. It is well known that RSR is an independent risk factor for all and major complications after OC surgery [1819].
In this study, we investigate the related and not-related morbidity associated to RSR in patients with stage IIIC–IV OC undergone debulking surgery and compare the rate between patients undergone to PDS vs. IDS.
MATERIALS AND METHODS
This study was a service evaluation project and obtained Trust approval (No. 3265). Since 2009, we utilised a dedicated database to prospectively collect surgical and histological data of all patients with stage IIIC–IV OC who undergo surgery at the Department of Gynaecologic Oncology of the Oxford University Hospital NHS Foundation Trust.
The current investigation focused on patients who had bowel surgery with RSR between January 2009 and March 2016. Before September 2011 upfront surgery was offered to all patient considered fit for surgery with CR as the only acceptable target. Starting from September 2011, after the publication of the European Organization for Research and Treatment of Cancer (EORTC) trial [6], all patients with stage IIIC–IV OC were electively treated with NACT and IDS. Over the study period, there were no significant differences in the facilities available for patient care and in the referral patterns of our service.
We define the type of surgery as multi-visceral surgery and non-multi-visceral, the latter being limited to hysterectomy, bilateral salpingo-oophorectomy and supracolic omentectomy. The techniques and outcomes of multi-visceral surgery (named Visceral-Peritoneal Debulking) were previously reported [10].
The triage process elected patients to multi-visceral surgery if: 1) The performance status was scored as American Society of Anesthesiologists <3 at pre-operative assessment; 2) Computerized tomography (CT) review showed no lung or multiple parenchymal liver metastases; 3) Explorative laparoscopy demonstrated no small bowel serosal disease or porta hepatis encasement. Surgery was performed 7 days after the laparoscopy. IDS was offered to patients showing partial response or stable disease at CT scan. Patients with progressive disease on chemotherapy were not offered surgery. Patients with recurrent OC or low-grade tumours were also excluded from the present analysis.
The indication for RSR was suggested by CT scan and the decision was ultimately based on finding the sigmoid-rectum involved by disease at surgery. The RSR was part of an en-bloc pelvic resection including the reproductive organs and the pelvic peritoneum. The techniques of RSR and bowel diversion have been previously described [520]. The level of the anastomosis was assessed at time of surgery and confirmed by pre-chemotherapy CT scan. All our patients received mechanical bowel preparation with Bisacodyl 20 mg the day prior to the operation.
The criteria for a bowel diversion were as following: 1) Multiple bowel resections; 2) Anastomosis ≤6 cm from the anal verge; 3) Tension on the anastomosis; 4) Air spillage at time of air test; 5) Intra-operative assessment of the bowel tissues before and after the anastomosis based on the surgeon's experience and perception such as vascularity, colour (pink vs. pale), bleeding edges of resected margins, pulsation, elasticity and temperature [2122].
Primary end points were to compare the rate of 30-day not-related and related complications (anastomosis breakdown, prolonged ileus, stoma retraction, pelvic abscess, or enteric fistula) and the rate of bowel diversion amongst the patients who received RSR between the 2 groups (PDS vs. IDS). Clavien-Dindo classification was used to grade surgical-related complications [23]. Only grade >2 complications within 30 days from surgery were registered.
Descriptive statistics for continuous and categorical variables have been reported as absolute number, rate, and percentage (%). A normality test (D'Agostino-Pearson test) was used to determine whether sample data followed a Gaussian distribution. Comparison between IDS and PDS groups was performed using the χ2 test or Fisher's exact test for categorical variables, and the Student's t-test or Wilcoxon rank-sum tests for continuous variables. All calculated p-values were 2-sided, and p-values less than 0.05 were considered statistically significant were performed with Graph Pad Prism version 6.0 (Graph Pad Software, San Diego, CA, USA).
RESULTS
Over the study period, 371 patients with stage IIIC–IV OC underwent surgical treatment. One hundred and twenty-six (34.0%) had PDS and 245 (66.0%) underwent IDS. Sixteen patients in the PDS group (16/126, 12.7%) vs. 76 patients (76/245, 31.0%) in IDS group did not require multi-visceral surgery as part of their treatment (p<0.001).
The flow chart is reported in Fig. 1. Overall, fifty-two patients in the PDS group (52/126, 41.3%) had RSR compared with 65 patients (65/245, 26.5%) in the IDS group (p=0.004).
 | Fig. 1Flow chart of the study population who underwent surgery and RSR during debulking for stage IIIC–IV OC: PDS vs. IDS post NACT.FIGO, International Federation of Gynecology and Obstetrics; IDS, interval debulking surgery; NACT, neoadjuvant chemotherapy; OC, ovarian cancer; PDS, primary debulking surgery; RSR, rectosigmoid resection.
|
Complete data were available for 112 patients: 49 (43.7%) in the PDS and 63 (56.3%) in the IDS group. The 2 groups were well comparable in terms of patient's baseline characteristics and tumour features (Table 1).
Table 1
Baseline and tumour characteristics of patients undergoing bowel surgery during debulking for stage IIIC–IV OC: PDS vs. IDS post NACT

Data are shown as mean±standard deviation or number (%).
CA125, cancer antigen 125; FIGO, International Federation of Gynecology and Obstetrics, IDS, interval debulking surgery; NACT, neoadjuvant chemotherapy; OC, ovarian cancer; PDS, primary debulking surgery; Pre-op, preoperative data within 30 days of surgery.
![]()
Results related to surgical procedures and outcomes are detailed in Table 2. More radical procedures were performed (mean 7.9±6.2 vs. 6.6±4.4, p=0.041) during PDS vs. IDS, respectively. However, operative time, blood loss and hospital stay were similar between the groups (p>0.05) (Table 2).
Table 2
Surgical procedures and outcomes in patients undergoing debulking for stage IIIC–IV OC: PDS vs. IDS post NACT
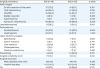
Data are shown as mean±standard deviation or median (range) or number (%).
CR, complete resection; IDS, interval debulking surgery; NACT, neoadjuvant chemotherapy; OC, ovarian cancer; PDS, primary debulking surgery; SD, standard deviation; USO/BSO, unilateral or bilateral salpingo-oophorectomy.
*Pelvic and/or para-aortic lymphadenectomy/enlarged lymph node(s) removal.
![]()
In the IDS group, 48 patients (76.2%) received Platinum and Taxol. Nine patients (14.6%) also received Bevacizumab and 6 patients (9.5%) platinum alone as part of their NACT treatment. All patients in IDS group underwent surgery after at least 3 cycles of platinum NACT. Surgery was performed between 4 and 6 weeks after the last cycle of NACT.
CR was achieved in 43 (87.7%) PDS and 56 (88.8%) IDS patients (p=0.761) (Table 2).
1. Assessment of postoperative complications
The 30-day not related complication rate (Clavien-Dindo≥2) was 38.8% in PDS and 28.6% in IDS (Table 3, p=0.312). Related-RSR specific complications occurred to 9 patients in the PDS group and 7 in the IDS group (18.4% vs. 11.1%, p=0.292). All patients with anastomosis breakdown (4/112, 3.6%), except one (1/112, 0.9%), were managed with surgical re-exploration and bowel diversion as they became septic after the leakage. This patient was treated with intravenous antibiotics and total parenteral nutrition. One patient (1/112, 1.8%) in PDS (diagnosed at day 7 with anastomosis breakdown), who was found with a pelvic abscess at time of surgical re-exploration, subsequently succumbed to pulmonary embolism.
Table 3
Incidence of post-operative overall and bowel specific complications in patients undergoing bowel surgery during debulking for stage IIIC–IV OC: PDS vs. IDS post NACT
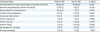
Values are presented as number (%).
IDS, interval debulking surgery; NACT, neoadjuvant chemotherapy; OC, ovarian cancer; PDS, primary debulking surgery.
![]()
The rate of 90-day mortality was 2.0% and 1.6% in PDS and IDS, respectively (Table 3).
With regards to the specific types of bowel surgery, we did not find any statistical differences between the groups in the rate of small and multiple bowel resections (Table 4). The sigmoid-rectal anastomoses were averagely 8 cm from the anal verge (range 3–12) in PDS and 7 cm (range 4–11) in IDS (p=0.743). No statistical differences were noted between the groups in terms of the staplers used for the RSR (Table 3).
Table 4
Specific bowel surgery procedures and instruments used for the RSR in patients undergoing debulking for stage IIIC–IV OC: PDS vs. IDS post NACT
Values are presented as median (range) or number (%).
GIA, Gastrointestinal anastomosis; IDS, interval debulking surgery; NACT, neoadjuvant chemotherapy; OC, ovarian cancer; PDS, primary debulking surgery; RSR, rectosigmoid resection; TA, transverse anastomosis.
![]()
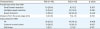
Patients in IDS had a slightly higher rate of bowel diversion compared to patients in the PDS group (46.0% vs. 26.5%, p=0.048) (Table 4). Of note patients in IDS were more likely to receive a bowel diversion due to impaired tissue quality (44.8% vs. none, p<0.001) while patients in PDS were more likely to receive a bowel diversion when receiving multiple bowel resection (92.3% vs. 34.5%, p<0.001).
Other reasons for bowel diversion did not statistically differ between the 2 groups (Table 5) and were stated as following: level of the anastomosis <6 cm from the anal verge in 4 patients (6.7%, 1/12 PDS and 10.3%, 3/29 in IDS; p=0.127); non-tension-free anastomosis in 2 patients (none in PDS and 6.9%, 2/29 in IDS; p=0.892), spillage at air test (none in PDS and 3.4%, 1/29 in IDS; p=0.498).
Table 5
Reasons for bowel diversion in patients undergoing bowel surgery during debulking for stage IIIC–IV OC: PDS vs. IDS post NACT

Values are presented as number (%).
IDS, interval debulking surgery; NACT, neoadjuvant chemotherapy; OC, ovarian cancer; PDS, primary debulking surgery.
![]()
Amongst the patient that received Bevacizumab, 6 of them received a bowel diversion (66.7%, 6/9).
DISCUSSION
In our study, the use of NACT for stage IIIC–IV OC was associated to a lower rate of patients needing multi-visceral surgery and bowel resection. However, when a RSR was required, no significant difference was recorded in the rate of overall and bowel specific complications between PDS and IDS. Of note, NACT increased the rate of bowel diversion following RSR.
A few studies in OC reported that NACT decreases the complexity of the debulking procedure, the operative time and the overall morbidity [67]. This is particularly true in patients who display a complete response to chemotherapy. However, complete responders to chemotherapy in OC represent a small group of patients, usually 15% if measuring clinical response and 5% if measuring histopathological response [672425].
In this study, 68.9% of patients (169/245) with IIIC–IV OC still required multi-visceral surgery due to partial response to NACT.
Interestingly when a RSR is performed, we failed to prove any advantage in favour of IDS over PDS with regards to surgical complexity, morbidity, as well as operative time. The rate of complications related to bowel surgery in the present investigation compares favourably to the results of previous studies [15262728].
Among 112 patients with RSR, we observed 5 anastomotic leaks (4.5%) and 1 recto-vaginal fistula (0.9%). While our rate of overall postoperative morbidity (not-related to RSR), is comparable to other International centres adopting aggressive cytoreductive surgery with similar high rate of CR [293031].
Two randomized clinical trials (RCTs) showed lower morbidity rate of surgery after NACT group when compared to upfront surgery group in stage IIIC–IV OC. Interestingly, in both these trials, the rate of bowel resection was low: 15.5% in upfront surgery and 8.7% during surgery after NACT in the EORTC trial, and 11% in upfront surgery vs. 8% during surgery after NACT in the chemotherapy or upfront surgery (CHORUS) trial [67]. Not surprisingly also the rate of CR rate was low in both trials. Concurrently, centres that adopted aggressive surgical debulking reported [10121332] rate of bowel resection between 40% and 80% irrespective of the surgical timing and higher rate of CR than in the2 RCT [67]. It seems therefore fair to say that the figures on morbidity reported by the EORTC and the CHORUS trials are not reflective of an aggressive surgical practice and not representative of the real peri-operative morbidity of most patients undergone to IDS.
Previous study suggested that bowel resection is associated to increased post-operative complications in the context of both PDS and IDS [1830]. In our study, with a CR rate of nearly 90% and despite more radical procedures where performed during PDS than IDS (mean SCS 7.1 vs. 6.3, p=0.041), we found no differences in post-operative complications when RSR was performed.
A recent French study assessing the morbidity of RSR amongst PDS and IDS showed higher morbidity in the latter group [28]. However, as mentioned by the authors, they were given NACT not to all patients with stage IIIC–IV but to selected patients with unfavourable risk factors such as old age or multiple comorbidities [28]. We believe that this finding, consistent with our previous report, confirms that the reduction of surgical morbidity attributed to NACT in an unselected population is limited to patients with complete or good response to chemotherapy.
Another interesting finding of the present study is that patients requiring RSR during IDS had an increased rate of bowel diversion compared to patients who had PDS. We investigated the presence of factors previously associated to anastomotic leak (age, level of haemoglobin, albumin, cancer antigen 125, and ascites) in the study groups [33].
The impaired quality of the tissues was the main factor associated with to the formation of a bowel diversion. Clearly this is a subjective decision of the surgeon at the time of operation. Some studies suggested that cytotoxic agents, including those used in patients with OC such as carboplatin, paclitaxel and bevacizumab, could heavily affect both normal epithelium and stroma and worsen the tissue quality and the elasticity of the bowel segments [34353637]. We postulated that this might have affected the decision towards a diversion during the surgery.
The strength of our study is the consistency of the protocol, the inclusion of all consecutive patients who had RSR in the study period, the provision of the same surgical expertise to both groups and the homogeneity of the groups. Moreover, timing was the only factor associated to switch from PDS to IDS, which means that no preoperative selection was performed. Clearly, the retrospective nature of the study implies a risk of selection bias.
The main study limitations are the retrospective design and the small number of patients with anastomotic leakage or bowel specific complications, which precluded the identification of risk factors.
In conclusion, our study suggests that NACT is associated to a reduced rate of multi-visceral surgery and RSR. However, when a RSR is performed in the context of IDS, this study failed to show any significant difference in terms of overall surgical-related and bowel specific morbidity compared to PDS. When bowel resection is required, IDS increases the risk of bowel diversion if compared with PDS.
This information might be useful during preoperative counselling and to tailor the most appropriate perioperative care in patients undergoing likely RSR for advanced OC during IDS.
 XML Download
XML Download