

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Human papillomavirus (HPV) is the most common sexually transmitted disease, worldwide, with more than 14,000 newly diagnosed infections every year [12]. HPV infections generally involved the lower genital tract and they rarely might determinate occurrence of dysplasia and cancer arising into the superficial epithelium.
Cancer of the uterine cervix is the most common malignancy caused by HPV infection in women [2]. Moreover, there is a strong evidence linking HPV with cancer of the head and neck district, as well as anus, vulva and vagina [12].
In particular, vaginal dysplasia represents a relative rare entity when compared to cervical dysplasia, representing about 0.4% of all intraepithelial neoplasia of the lower female genital tract. In fact, it is estimated to occur in 0.2 to 0.3 per 100,000 women, being its incidence approximately 100-fold lower than cervical counterpart [345]. According to the American Society for Colposcopy and Cervical Pathology and the College of American Pathologists vaginal dysplasia can be classified as low-grade vaginal intraepithelial neoplasia (VaIN) and high-grade VaIN [6].
Although the diagnosis of vaginal dysplasia is increased in the recent years [789], only few studies evaluated outcomes of women affected by VaIN [8910111213141516]. There is no consensus about the optimal treatment modality for women affected by high-grade VaIN. Treatments' modalities included: medical treatments with topical application of imiquimod or 5-fluorouracil (5-FU), as well as ablative and excisional procedures executed via surgery, diathermocoagulation and carbon dioxide (CO2) laser [458910111213141516]. However, regardless treatment modality used, patients affected by high-grade VaIN (also known as vaginal high-grade squamous intraepithelial lesion) are at high risk of recurrence and are at risk of developing invasive disease [8910111213141516]. No clear data about women developing recurrent high-grade VaIN are available. Moreover, there are no data supporting the execution of a treatment modality rather than another in the setting of recurrent high-grade VaIN. In the present paper we aimed to report outcomes of a large series of women having treatments for recurrent high-grade VaIN. As secondary endpoint, we sought to investigate the efficacy of various treatment modalities for women affected by recurrent high-grade VaIN. Additionally, we aimed to assess a possible correlation between primary treatment modality and the outcomes of secondary treatments.
MATERIALS AND METHODS
The Institutional Review Board (IRB) of National Cancer Institute (NCI)–Milan approved this study (IRB No. INT/MI/006812). We retrospectively reviewed records of consecutive women undergoing treatments for recurrent high-grade VaIN between 1998 and 2017 at Gynecologic Oncology Unit of NCI–Milan, Italy.
Primary endpoints measures were to describe outcomes of a large series of patients affected by recurrent VaIN. Secondary endpoint was to assess efficacy of various treatments modalities for patients affected by recurrent high-grade VaIN. Demographic details, data about HPV type(s) detected as well as data on treatment and follow-up were searched in order to identify predictors for recurrence of high-grade VaIN. Inclusion criteria were: 1) histologically confirmed recurrent high-grade VaIN, 2) data about primary, and 3) secondary treatments. Exclusion criteria were: 1) age younger than 18-years, 2) withdrawal of consent, 3) presence of invasive lower genital cancer at the time of primary treatment, and 4) and/or before recurrence of high-grade VaIN.
During the whole study period, laser treatment represents the standard treatment modality for patients affected by high-grade VaIN; while, medical and other surgical treatment modalities were offered in selected cases. Generally, medical treatments were prescribed in case of focal high-grade VaIN or small and /or multifocal lesions. No specific guidelines are available for patients with recurrent high-grade VaIN.
Histological diagnosis of high-grade VaIN was defined as the presence of moderate or severe vaginal intraepithelial dysplasia arising into the native squamous epithelium of the vagina, without invasion. A pathology review conducted by 2 dedicated gynecologic pathologists (MLC, BP) and was performed for all vaginal specimens. All patients were evaluated colposcopically in outpatients' clinic. A dedicated team of gynecologic oncologists performed all gynecologic and colposcopic examinations as well as vaginal samples collection (including vaginal smear, HPV DNA test and vaginal biopsies when indicated).
Generally, CO2 laser treatment included the execution ablative procedures. Laser surgery allows simultaneous photo-thermal ablation and coagulation. Combination between power of laser (i.e., watts) and spot diameter determines the effect between laser and vaginal tissues. Power density (i.e., intensity) is expressed in watts/cm2. During laser ablative procedures power density might range between 500 (having a power of 20 watts and a spot diameter of 2 mm) to 12,000 (having a power of 30 watts and a spot diameter of 0.5 mm) watts/cm2. Wavelength of 10,600 nm, depth of penetration of 0.1–0.5 mm and 0.5 mm of lateral thermal damage characterize CO2 laser. All procedures were performed under direct colposcopic examination. Before undergoing either laser ablation or medical treatments patients had at least 1 vaginal biopsy, in order to exclude the presence of an invasive carcinoma. Generally, medical treatment included the use of 5-FU (1 application/week per 6 weeks).
A new (second) recurrence was defined by the presence of biopsy-proven diagnosis of moderate/severe vaginal dysplasia (i.e., high-grade VaIN). Follow-up were scheduled every 6 months during the first 2 years after treatment and annually thereafter. During follow-up, clinical and colposcopic examinations as well vaginal/cervical smear were carried out at every examination. Usually, HPV testing was recommended before treatment and at the time of first post-treatment follow-up (at 6-month) and when indicated by treating physicians. For the detection of HPV infection, vaginal or cervical specimens taken with a brush or cotton swab were resuspended in a tube containing 3 mL of 0.9% Sodium Chloride Solution and stored at −20°C until use. The tests were performed by the Clinical Array Technology HPV 2 kit (Genomica, Madrid, Spain), which combines highly specific and highly sensitive polymerase chain reaction with the technology of low-density arrays. Details of this method are reported elsewhere [1718].
1. Statistical analysis
Data are summarized using basic descriptive statistics. Normality testing (D'Agostino and Pearson's χ2 test) was performed to determine whether data were sampled from a Gaussian distribution. Ten-year survival outcomes were evaluated with both Kaplan–Meier and Cox models. Hazard ratio (HR) and 95% confidence interval (CIs) were calculated for each comparison. Univariate and multivariate analysis were performed when appropriate, using Cox proportional hazard model. All covariates with a p-value less than 0.10, based on univariate analysis were included in the multivariate model. All p-values were 2-sided. The p-values <0.05 were statistically significant. Statistical analyses were performed using GraphPad Prism version 6.0 (GraphPad Software, San Diego, CA, USA) for Mac and IBM-Microsoft SPSS version 20.0 (IBM Corp., Armonk, NY, USA) for Mac.
RESULTS
Data of 117 women were available for the analysis. At primary diagnosis, 41 (35%), 4 (3.4%), and 72 (61.6%) patients had had laser, pure surgical and medical treatments, respectively (Fig. 1). The majority of patients (56 out of 72, 77.7%) who had primary medical treatments were referred to our unit from other centers after failure.

Mean (standard deviation [SD]) patients age was 56.3 (11.9) years. Table 1 reports baseline characteristics of the study population. Median time from primary treatment and diagnosis of recurrent high-grade VaIN was 18 (range, 3–56) months. Patients having primary laser therapy had longer progression-free survival (p<0.001). In fact, median time from primary laser treatment and recurrent high-grade VaIN was 20 (range, 5–42) months; while, median time from primary medical treatment and recurrent high-grade VaIN was 13 (range, 3–56) months. Secondary treatments included: CO2 laser ablation and medical treatment in 95 (81.2%) and 22 (18.8%) cases, respectively. Patients having primary medical treatments are more likely to have secondary treatment with laser ablation in comparison with patients who already had laser as primary treatment modality (94.4% vs. 53.7%; p<0.001).
Table 1
Baseline patients' characteristics

Data are shown as number (%).
HPV, human papillomavirus; HR, high-risk; HSIL, high-grade squamous intraepithelial lesion.
![]()
After a mean (SD) follow-up of 72.3 (39.5) months, 37 (31.6%) out of the entire cohort of 117 patients developed a second recurrence. Median time to recurrence was 20 (range, 5–42) months. As reported in Fig. 2, patients with recurrent high-grade VaIN undergoing medical treatments were at higher risk of developing second high-grade VaIN recurrence in comparison to women having laser treatment (p=0.013, log-rank test). Considering the subgroup of 41 patients having primary laser treatment, the execution of medical treatments at the time of high-grade VaIN recurrence is associated to a slightly but not significant increased risk of recurrence (p=0.148, log-rank test) (Fig. 3). Laser treatment was offered to all patients having recurrence after primary medical treatment. Two patients refused and had another attempt with medical treatments (these 2 patients were disease-free at 32 and 24 months). Fifteen (21.4%) out of 70 patients having laser after primary medical treatments developed second recurrence.
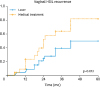 | Fig. 2Risk of developing second recurrence in patients with recurrent VaIN (vagina HSIL).HSIL, high-grade squamous intraepithelial lesion; VaIN, vaginal intraepithelial neoplasia.
|
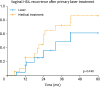 | Fig. 3Risk of developing second recurrence in patients with recurrent VaIN (vagina HSIL) treated with laser at diagnosis.HSIL, high-grade squamous intraepithelial lesion; VaIN, vaginal intraepithelial neoplasia.
|
Polling together data of the entire cohort (n=117), after we corrected our results for type of treatment used for recurrent high-grade VaIN, we observed that the execution of primary laser treatment was independently associated with a slightly risk of developing second recurrence (HR=0.46; 95% CI=0.21–0.99; p=0.050). The other variable that is independently associated with second recurrence is the persistent infection from HPV 16 or 18 (HR=3.87; 95% CI=1.15–13.0; p=0.028). Additionally, an increase in patients' age is associated with a slightly (non-significant) lower risk of developing recurrence (HR=0.61; 95% CI=0.37–1.006; p=0.053). Table 2 reports results from multivariate analysis. In our series 9 (7.7%) cases of cancers arising in the lower genital tract were detected. Invasive malignancies included: vaginal cancer (n=2), cervical cancer (n=3), vulvar cancer (n=2), and anal cancer (n=2).
Table 2
Predictors of high-grade VaIN second recurrence

CI, confidence interval; HPV, human papillomavirus; HR, hazard ratio; HSIL, high-grade squamous intraepithelial lesion; VaIN, vaginal intraepithelial neoplasia.
*HR per 10-year increase.
![]()
DISCUSSION
The present paper reported outcomes of a large cohort of women affected by recurrent high-grade VaIN, thus reporting a number of noteworthy findings. First, we observed that patients affected by recurrent high-grade VaIN are at high risk of developing vaginal dysplasia persistence. Second, about 1 patient out of 10 with recurrent high-grade VaIN is at risk of developing invasive cancer of the lower genital tract. Third, we observed that laser treatment is more effective than medical treatments in reducing the risk of developing second recurrence. Fourth, treatment of high-grade VaIN at it first presentation impacts on outcomes of further treatments. In our series, patients receiving laser treatments (as first line) experienced better outcomes than patients having medical and other surgical treatments, regardless the treatment modality utilized at the time of recurrence.
VaIN is a rare entity. Few studies investigated outcomes of newly diagnosed high-grade VaIN, reporting non-conclusive results [458910111213141516]. There is no consensus about the preferred treatment modality for these patients. Fiascone et al. [4] evaluated the efficacy of various treatment modalities in 137 women affected by high-grade VaIN. Among those, 47, 35, and 22 patients treated with 5-FU, excision and laser ablation, respectively. The treatments result to be effective (no recurrence detected) in 35 (74%; 95% CI=62%–87%), 20 (57%; 95% CI=41%–74%), and 9 (41%; 95% CI=20%–61%) patients having 5-FU, excision and laser ablation, respectively [4]. In a large experience on 576 patients VaIN (including 397 cases of high-grade vagina dysplasia), Kim et al. [19] observed that laser treatments are the most effective treatment modality for this condition. In this study, the rate of progression/persistence of was 62.5%, 26.4%, and 32.7% following medical treatment, laser ablation and excision, respectively [19]. These data are confirmed by our previous experiences focusing on newly diagnosed high-grade VaIN [820]. In a research focusing on 77 patients we observed that the execution of laser instead of medical treatments is associated with a lower recurrence rate and a higher HPV clearance [20]. In another larger studies collecting data of 204 women, we observed that laser treatment is effective, being recurrence rate relative low 20%. In this study we compared outcomes of patients having ablative and excisional procedures [8]. Using a propensity-score matching we observed that type of procedure has not impact on recurrence rate and risk of developing lower genital tract malignancies [8]. Interestingly, in our series patients having primary medical treatments were more likely to the submitted to laser procedures in comparison to patients having laser at primary diagnosis. Although no specific guidelines are available in our centre we are likely to try other treatment modalities after a primary ineffective treatment. Our study showed that treatment of high-grade VaIN at it first presentation impacts on outcomes of further treatments. Patients having VaIN after primary laser approach are at lower risk of developing second recurrence in comparison to patients having medical treatment. Owing the retrospective nature of the study, we can speculate that this finding might express a selection bias; probably, medical treatments would be proposed much more in patients multifocal or extensive disease; while laser treatment would be offered in patients with more localized disease. However, further attention is needed to better understand this possible association.
Another interesting point is the risk of developing vaginal and other lower genital tract invasive cancer among patients affected by high-grade VaIN. Combined data from the Centre of Disease Control's National Program of Cancer Registries and the NCI's Surveillance, Epidemiology, and End Results underlined the rarity of vaginal cancer its rate being approximately 0.5/100,000 women [2]. According to what we observed in our previous publications, the risk of developing invasive cancer of vagina and of the lower genital tract an is lower than 2% and 10%, respectively [820]. Recently, another Italian study, published by Sopracordevole et al. [12], reported a quite higher risk of occult cancer into vaginal specimens of women affected by high-grade VaIN. The authors reported 6 (10.5%) cases of occult cancers in a series of 57 patients having laser excision [12]. However, the low rate invasive cancer is supported by other larger studies. Piovano et al. [16] analyzed data of 285 patients with VaIN and observed that no patient progressed to vaginal cancer. Ratnavelu et al. [10] evaluated a series of 31 patients with high-grade VaIN managed with surveillance only, they reported that no cancers were diagnosed after a median follow-up of 35 (range, 2–230) months. Zeligs et al. [9] did not observe the occurrence of any invasive vaginal cancer in a series of 127 women affected by low (n=75) and high-grade (n=52) VaIN. Dodge et al. [21] reported a 2% of risk of developing vaginal cancer among 121 women. Potentially, the growing adoption of vaccination against HPV might reduce the risk of developing recurrent VaIN. Findings observed among patients having treatments for cervical intraepithelial neoplasia, highlighted that vaccination might reduce the risk of recurrence [22]. Although these data should be validated in patients with vaginal dysplasia, we might expect similar results.
The inherent biases related to the single centre, retrospective study design represent main weaknesses of the present study. Therefore, our results have to be confirmed by other studies. Another weakness regards the possible association with VaIN and the risk of developing invasive cancers. Although we can speculate an association between VaIN and invasive carcinomas of the lower genital tract, patients with cancers are not routinely tested for HPV presence. Moreover, we have no data regarding types of HPV involved in VaIN and invasive carcinomas.
In conclusion, the present paper reported outcomes of one of the largest series focusing on recurrent high-grade VaIN. In agreement with the background our data highlight the high recurrence rates of VaIN after treatments. Interestingly, we observed that laser ablation is associated to a lower risk of recurrence in comparison to medical treatments. More important, we observed that the execution of laser treatment as primary treatment improve response rate of recurrent disease. The risk of progression from high-grade VaIN to invasive cancer is relative low, even in the setting of recurrent VaIN. Further studies are needed to identify the preferred treatment modality of newly diagnosed and recurrent high-grade VaIN.
 XML Download
XML Download