

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Intertrochanteric hip fractures in the elderly are an important orthopedic problem globally due to the aging population and the increasing incidence of osteoporosis. Intertrochanteric hip fractures have a high rate of fusion, but the subsequent functional outcome is poor, and the mortality rate within 1 year after the injury has been reported to be as high as 12% to 36%.1) Surgical treatment is the most important method in the intertrochanteric hip fractures. The goal of the treatment is to restore preoperative function and mobility in a short time. As an operative treatment for intertrochanteric hip fractures, extramedullary fixation and intramedullary fixation have been used. Among these, intramedullary fixation is increasingly used for biomechanical advantages and less invasiveness.234)
One of the most important factors in intramedullary fixation is the quality of reduction. In varus reduction, the force applied to the implant increases, and the stability of the fracture is decreased, leading to a loss of reduction.5) Therefore, many surgeons use valgus reduction to increase the compressive force between the bone fragments and reduce the force between the bones and the implant to prevent loss of reduction.67) Another important factor in intramedullary fixation for intertrochanteric hip fractures is the position of the blade at the femoral head.8) In this regard, attempts have been made to decrease the tip-apex distance (TAD), which emphasizes positioning as deeply as possible in the center of the femoral head. In recent years, the concept of calcar referenced tip-apex distance (calTAD) has emerged on the grounds that placing the blade in the inferior part of the femoral neck and head is more biomechanically and clinically advantageous.9101112) Therefore, non-varus reduction and the good position of the blade, the two important factors in intramedullary fixation, should always be kept in mind during the surgery.
However, there is no study that explains the relationship between the status of reduction and the position of the blade. We hypothesized that the status of reduction would affect the position of the blade. The purpose of this study was to investigate the relationship between the status of reduction and the position of the blade when proximal femoral nail antirotation (PFNA) was used in intertrochanteric hip fractures.
METHODS
Patients and Exclusions Criteria
A total of 585 patients who were treated with PFNA among patients who visited Inje University Sanggye Paik Hospital for intertrochanteric hip fractures from March 2009 to April 2015 were retrospectively reviewed. We conducted this study in compliance with the principles of the Declaration of Helsinki. The protocol of this study was reviewed and approved by the Institutional Review Board of Sanggye Paik Hospital (IRB No. 2018-05-022).
Of these, 30 patients were excluded because they underwent arthroplasty or internal fixation for proximal femoral fractures and measurement of the contralateral neck-shaft angle were not available. In addition, 25 patients were excluded because the distance from the blade tip to the subchondral bone was more than 15 mm or less than 10 mm. Ultimately 530 patients were included in this study. Their mean age was 78.7 ± 10.6 years, and there were 133 males and 397 females (Fig. 1).
Surgical Technique
All patients underwent surgery under epidural or general anesthesia. One single surgeon (YBS) performed the same valgus reduction procedure for all the patients to compare the neck shaft angle with that of the uninjured femur. First, external rotation of the affected leg was performed, followed by traction, abduction, adduction, and internal rotation in the described order. The reduction of the fracture site was confirmed by an image amplifier.13)
If the femoral head center was located higher than the greater trochanter tip in the preoperative radiographs, 130° PFNA was used; if not, 125° PFNA was used. The surgeon positioned the blade tip within 10–15 mm of the subchondral bone on the anteroposterior and lateral views of the image amplifier in all patients (Fig. 2).14) Care was taken not to place the blade in the superior portion of the femoral neck in all cases.
Radiological Assessment
We compared the femoral neck-shaft angle of the injured side with the contralateral side in the radiographs taken immediately after the operation, and patients were divided into the valgus-reduced group (group 1) and the non-valgus reduced group (group 2). The “valgus reduced” was defined as valgus reduction over 5°. In cases where contralateral proximal femoral fracture operation was also performed and it was difficult to check the neck-shaft angle of the contralateral side, any radiography performed in a previous study was used to check the neck-shaft angle on the contralateral side. Pelvis anteroposterior plain radiographs were taken at 10° internal rotation with half of the lesser trochanter shown.
To measure how far down the blade tip was located in the femoral head, the calTAD was measured on pelvis anteroposterior and lateral plain radiographs taken immediately after the operation (Fig. 3).1015)
In addition, in order to determine how close the position of the blade to the medial femoral neck, the area between the blade and the medial femoral neck was calculated. On simple radiographs taken immediately after the operation, two inflection points where the femoral neck and the femoral head meet were connected by a line. Then, the line was moved in parallel to pass the inflection point where the femoral neck and the greater trochanter meet. The area of trapezoidal shape between the blade and the medial femoral neck was created. To correct for differences in the femoral neck length, the area was divided by the square of the height of the trapezoid (Fig. 4). The picture archiving and communication system (PACS; Marosis M-view 5.4, Marotech, Korea) was used for all measurements.
Statistical Analysis
The valgus-reduced group (group 1) and the non-valgus reduced group (group 2) were set as independent variables, and the calTAD and the area between the blade and the medial femoral neck were set as dependent variables. It can be assumed that both dependent variables have a normality of more than 30 samples, and independent sample t-test was performed to determine whether there was a significant difference between the two groups. The difference between the two groups was judged to be significant when the p-value was less than 0.05. The statistical analysis was performed using IBM SPSS ver. 24.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Preoperative Evaluation
Female patients were dominant in both group 1 (male:female, 94:322) and group 2 (male:female, 39:75). The mean age was 79.0 ± 10.1 years in group 1 and 77.6 ± 12.0 years in group 2. Both groups used 130° PFNA implants more than 125° PFNA implants. Preoperative demographic data are summarized in Table 1.
Radiological Outcomes
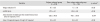
The valgus reduced group (group 1) had 418 cases and the non-valgus reduced group (group 2) had 112 cases. In group 1, the mean valgus reduction was 8.7° ± 6.5° and in group 2, the value was 1.7° ± 1.8°. The calTAD was measured as 22.5 ± 4.1 mm in group 1 and 24.9 ± 3.7 mm in group 2 (p < 0.05). The area between the blade and the medial femoral neck was measured as 135.5 ± 49.8 mm2 in group 1 and 145.0 ± 55.1 mm2 in group 2. The correction of the difference in the femoral neck length was 0.55 ± 0.16 in group 1 and 0.79 ± 0.19 in group 2 (p < 0.05) (Table 2).
DISCUSSION
The principal finding of this study is that in the valgusreduced group, the calTAD was decreased and the blade position was located inferiorly in the femoral neck, resulting in firmer fixation at the femoral head and neck. Treatment of intertrochanteric hip fractures is important to improve the prognosis in patients with early ambulation. Currently, internal fixation with PFNA and several valgus reduction techniques have been widely used to decrease the risk of varus deformity due to flexion moment that occur during early gait. Laskin et al.16) reported satisfactory results using the Wayne-County reduction method, which is a valgus reduction method that overlaps the medial and posterior cortices of the proximal femur in unstable intertrochanteric hip fractures with posteromedial bone defect. Choi et al.6) also reported that the Wayne-County reduction method was superior to the anatomic reduction method in terms of radiographic and clinical outcomes in unstable intertrochanteric hip fractures. Chang et al.17) reported that radiologically excellent results were obtained using positive medial cortical support, which is a nonanatomic reduction method that locates the medial cortex of proximal fragment superomedial to the medial cortex of distal fragment. Park et al.7) and Jiamton et al.18) also reported that valgus reduction was an effective treatment to decrease the failure of internal fixation, especially in unstable intertrochanteric hip fractures and to obtain good radiological and clinical results.
When PFNA is used, the blade may cause major complications such as perforation of the femoral head, so the positioning of the blade is very important. Jiamton et al.18) reported that the risk of perforation of the femoral head was decreased when the tip of the blade was located in the inferior half of the femoral head. Kashigar et al.,10) Caruso et al.,15) and Puthezhath and Jayaprakash12) reported that the risk was decreased when the calTAD decreased. In addition, according to Stiehl et al.,9) the inferior side of the femoral neck is a dense trabecular structure, which is more resistant to loading stress than other parts of the femoral neck. Therefore, positioning the blade at the inferior half of the femoral head and the inferior side of the femoral neck during internal fixation is advantageous for obtaining stable fixation. However, there was no study on the relationship between the status of reduction and the position of the blade of the PFNA. Therefore, this study has significance as the first study to quantify the relationship between the two.
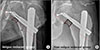
In this study, 418 of 530 cases were group 1 and 112 cases were group 2. The calTAD was significantly smaller in group 1 than in group 2, indicating that valgus reduction is advantageous for positioning the blade tip in the inferior half of the femoral head. There is no quantification method available for proximity of the blade to the medial femoral neck, so we measured the area between the blade and the medial femoral neck under the assumption that the blade was located near the medial femoral neck when the area was small. In group 1, the area was smaller than that in group 2, indicating that the blade was located closer to the medial femoral neck and the firm fixation force could be obtained (Fig. 5).
There are limitations of this study. First, there may be bias inherent to the retrospective design. To overcome this limitation, we measured the calTAD and the area between the blade and the medial femoral neck in a blinded manner before groups. Second, we did not investigate the clinical outcome. In previous papers, the impact of blade position on the clinical outcome was already addressed.10121518) Therefore, we focused on assessing the quality of reduction and the position of the blade radiologically in this study. We think that it will be also meaningful to follow the clinical outcomes of each group. Valgus reduction resulted in less calTAD and inferior position of the blade at the femoral neck in the treatment of intertrochanteric hip fractures with PFNA. In addition, it seems to provide firm fixation at the femoral head and neck.





 XML Download
XML Download