

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The acetabular labrum is a triangular fibrocartilaginous tissue located between the acetabulum articular cartilage and the joint capsule, which increases the stability of the hip joint.1) Inside the acetabular labrum, there are nerve endings involved in proprioception and nociception; thus, pain can occur when the labrum is damaged.2) It was reported that pathological changes in the acetabular labrum lead to chronic acetabular pain and limited quality of life.34) In the past, Altenberg3) also suggested labral tears as a cause of hip joint pain not related to trauma in 1977. He reported that severe pain and mechanical symptoms occurred due to a translocated acetabular labrum and symptomatic relief could be obtained immediately after removal of the acetabular labrum. However, once resected, the labrum is not regenerated; thus, the role of acetabular labrum in the hip joint has been extensively studied. Recently, there has been remarkable improvement in hip arthroscopy instruments and skills related to labral tears. In addition, the acetabular labral tear has become of great interest due to its relation with hip arthritis.5)
It has been reported that arthroscopic acetabular labral resection, effective for immediate pain relief, could damage the inherent physiological function of the labrum.6789) There is no literature on the long-term outcome of labral repair in hip arthroscopy especially in the Asian population. The purpose of this study was to analyze the long-term follow-up results of arthroscopic acetabular labral repair and to determine the effectiveness of labral repair in Asian femoroacetabular impingement (FAI) patients.101112)
METHODS
We conducted this study in compliance with the principles of the Declaration of Helsinki. The protocol of this study was reviewed and approved by the Institutional Review Board of Chungnam National University Hospital Institutional Review Board (IRB No. CNUH 2018-08-032). All of the patients provided informed consent.
Patient Selection
A retrospective review of all cases that underwent hip arthroscopy at our institution from January 2008 to December 2010 was performed. The procedure was performed by the same senior surgeon (DSH) in all cases. Only patients with complete medical records including operation records, follow-up scores and preoperative, postoperative and follow-up radiographs were included. Patients who had the following hip conditions previously were excluded: Legg Calves-Perthes disease, infectious hip disease, avascular necrosis, rheumatic disease, pyogenic and tuberculous arthritis diffuse idiopathic skeletal hyperostosis, ankylosing spondylitis, and severe dysplasia. Patients with preoperative Tönnis osteoarthritis (OA) grade 2 or more were also excluded. A total of 45 patients were found to satisfy the inclusion and exclusion criteria. Additional three-dimensional computed tomography (3D-CT) and magnetic resonance imaging (MRI) were performed in patients with chronic hip pain suspected of an acetabular labral tear based on medical history taking, physical examination, and plain radiography.
History taking performed during the first visit three included the onset, cause and aggravation of pain. Physical examinations such as log rolling, Patrick test and impingement test were performed.1314) Simple radiography was performed to obtain the pelvic anteroposterior view, frog-leg side view, false-profile view and cross-table view to confirm the acetabular or femoral bony deformities, femoral-acetabular dysplasia and bump formation in the femoral neck. In addition, 3D-CT and MRI were performed to check bony deformities and labral pathologies. All the radiographs were evaluated by two orthopedic surgeons (JWL and JMH) and one orthopedic radiologist (STK) working at the same hospital. Because of the low sensitivity of MRI for detection of labral tears, we did not depend on MRI but relied on physical examinations and duration of symptoms to determine surgical indications. Hip arthroscopy was performed under general or epidural anesthesia. Arthroscopic findings of labral tears were classified with respect to radial fibrillation, peripheral longitudinal tears, bucket-handle tears, complete detachment, atrophy or absence and mixed type according to the classification of Lage et al.15) FAI was confirmed by checking impingement during hip motions in arthroscopy.
There were 22 males and 23 females, and their mean age at the time of surgery was 33.0 years (range, 16 to 54 years). The lesion was located on the right side in 28 cases (62%) and the left side in 17 cases (38%). Of the 45 patients, four patients (one male and three females) were not available for a long-term follow-up. Thus, the remaining 41 cases followed up for 85–117 months (mean, 92.4 months) were reviewed for analysis. Ultimately, patients included consisted of 21 males and 20 females with a mean age of 34.6 years (range, 16 to 54 years). The mean bodymass index was 24.3 ± 3.3 kg/m2 (range, 18.6 to 38.5 kg/m2). Patient demographics are summarized in Table 1.
Surgical Technique and Postoperative Care
Standard portals were used with the patient lying on the fracture table. First, capsulotomy was performed between the anterior and anterolateral parts of the femur neck using an arthroscopic knife (Banana blade, 254 mm; Arthrex, Singapore) to handle the arthroscope easily. After confirming the lesion through arthroscopy, acetabular cartilage debridement was performed and suture was performed using a nonabsorbable suture anchor as descried by Kelly et al.16) Labral repair was achieved with sutures looped around the torn segments or placed through the torn labrum (looped stitch technique) and performed usually using 2–3 stitches for each torn labrum at 1-cm intervals. Each suture was anchored to the acetabular rim, with the suture anchor (2.3 mm Osteoraptor; Smith & Nephew, Andover, MA, USA) placed approximately 2 to 3 mm above the cartilage surface. Then, femoroplasty was performed in the femoral neck after flexion of the hip if a bump formed at the femoral head-neck junction.
From the first postoperative day, the pendulum movement of the hip joint and partial weight-bearing using crutches were allowed, but more than 90° of hip flexion motion was prohibited. Around three days after the operation, the patient was discharged and follow-up in the outpatient clinic to monitor the clinical outcome. Full weight-bearing of the hip joint was allowed 4 weeks after the operation.
Clinical Outcomes Measurement and Statistical Analyses
Clinical and radiographic follow-up evaluations were performed at 6 weeks; 3, 6 and 12 months; and every 1 year thereafter. Patients who did not attend regularly scheduled visits were contacted by telephone. Clinical assessment was performed using a modified Harris hip score (MHHS), visual analog scale (VAS), hip outcomes score (HOS), and patient satisfaction score (0–10 scale; 10, very satisfied). The last long-term follow-up clinical results were compared with preoperative values and short-term follow-up results. Tönnis grade was classified by simple radiological changes. Statistical analysis was conducted using repeated measures analysis of variance test with Scheffe's post hoc test for MHHS, VAS and HOS and a paired t-test for Tönnis grade in IBM SPSS ver. 21.0 (IBM Corp., Armonk, NY, USA). A p-value < 0.05 was considered statistically significant for all differences.
RESULTS
For evaluation of clinical outcomes, preoperative values, short-term (2–5 years) follow-up results and last long-term follow-up (7–10 years) results were compared. The mean VAS score significantly improved from 6.4 points (range, 2 to 9 points) preoperatively to 2.5 points (range, 0 to 7 points) at the short-term follow-up, and then to 1.8 points at the last long-term follow-up (p < 0.01). The mean mHHS score improved from 59.5 (range, 37.5 to 82) preoperatively to 85.4 (range, 60 to 94.6) in short-term and then to 86.8 (range, 61 to 95.7) in long-term follow-up (p < 0.01). Activities of daily living HOS was significantly improved from 58.3% (range, 20% to 80%) preoperatively to 83.0% (range, 45% to 95%) in the short-term and then to 85.2% (range, 45% to 95%) in the long-term follow-up (p < 0.01); sports-related activities of HOS was also improved from 51.2% (range, 10% to 80%) to 79.8% (range, 50% to 95%) and then to 82.4% (range, 50% to 95%; p < 0.01) in the respective period. At the last follow-up, the mHHS was more than 80 points (satisfied or very satisfied) in 35 cases (78.8%) and less than 70 points (dissatisfaction) in three cases (6.7%). The mean patient satisfaction score was 7.6 ± 2.2. The average Tönnis grade based on the last follow-up simple radiography was 0.67 (range, 0 to 3), which showed no statistically significant difference from the initial average grade of 0.51 (range, 0 to 1; p = 0.227) (Fig. 1).
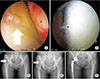
Six patients (14.6%) underwent reoperation due to complications. No other complications were noted. Five cases (12.2%) underwent revisional arthroscopic procedures and one case (2.4%) had conversion to total hip arthroplasty (THA). Secondary arthroscopic procedures were performed at a mean of 26.6 months after surgery (range, 15 to 49 months). There were three cases of labrosynovial adhesions due to synovial hyperplasia in the acetabular region, one case of pullout of the suture anchor and one case of heterotopic ossification. The one case of conversion to THA occurred at 86 months postoperatively. The Tönnis grade was 1 preoperatively in the patient, but due to joint space narrowing and degenerative changes, the grade at the last 86 months of follow-up was 3, which required THA (Fig. 2). Data on all revisional arthroscopic procedures and conversion to THA are summarized in Table 2.
DISCUSSION
Larson et al.11) compared the arthroscopic results of debridement and labral repair in cases of FAI and observed better results with repair. The mean mHHS of the repair group was 64.5 before surgery and 94.3 in the final evaluation, which was 9.4 points higher than that in the debridement group. Jackson et al.17) evaluated 54 patients who had undergone arthroscopic labral repair. They observed significant improvement in the four scores at 2.4 years after the procedure; the mean mHHS was 63.7 preoperatively and 89.9 at the final evaluation. Furthermore, 85.2% of the patients had good or excellent results. Similarly, three functional scores, VAS and satisfaction were used in our study and we also had favorable results.
Repair of labral tears is preferred than resection of labral tears for preservation of the function of the joint. Many clinical outcome studies have provided supporting biomechanical data and conclusions. Multiple comparative cohort studies and one prospective randomized study have demonstrated that patients undergoing labral repair have significantly better outcomes than labral debridement.111819) The systematic review by Ayeni et al.,20) which includes most of these studies as well as the outcomes of open procedures, found similar results favoring repair over debridement. Other recent studies also discovered labral debridement procedures caused micromotions in the hip joint, contributing to the development of OA.21) With these reports in mind, we repaired acetabular labrum tears whenever possible, considered that the labrum is essential for joint-cartilage protection.
Arthroscopic labral repair outcomes in our study were favorable. Compared with the short-term results in the same patient group published 5 years ago,22) the VAS, mHHS, HOS were not improved significantly at the long-term follow-up. Scheffe's post hoc test revealed that the mHHS and HOS more significantly improved during the short-term follow-up (p < 0.05). Of note, however, is that there was improvement in outcomes in a slow and continuous manner. On the other hand, improvement in clinical outcomes of the arthroscopic labral resection group published previously by our study team23) was not the same. The mean mHHS in this group was 58.9 preoperatively, 81.9 in the short-term follow-up and 79.3 at the final follow-up. Similarly, the hip outcome score-activity of daily living (HOS-ADL) and sport-specific subscale (HOS-SSS) that improved in the short-term period slightly decreased at the final mid-term follow-up. So labral repair procedures could be more conducive to long-term improvement of the patient's functional scores than labral resection procedures.
There are not many studies on the long-term results of arthroscopic operation for FAI. Menge et al.24) reported 10-year outcomes and the hip survival rate of hip arthroscopy for FAI to compare labral resection with labral repair. In the study, significant improvement in clinical outcomes (HOS-ADL, HOS-SSS, mHHS, short form 12 health survey and physical composite scores) was obtained regardless of the labral procedure. Seven of the 154 patients (4.5%) underwent revisional hip arthroscopy, two of whom were in the labral resection group and the other were in the labral repair group. They reported that 34% of the patients had a THA within 10 years following the arthroscopy and the rate of conversion to THA was not related to the labral treatment method. Our study is a case series report of a labral repair group, so we could not compared with a labral resection group. However, the significance of this study can be found in the fact that there have been no other studies in Asia reporting the long-term follow-up outcomes in FAI.
Except for the case that required conversion THA, all revisional arthroscopic procedures were performed in the short-term follow-up period. There was no case that required a revisional arthroscopic procedure in the mid-term and long-term follow-up periods. Therefore, it could be interpreted that the hip joint is more stabilized after a short-term period following arthroscopic labral repair.
In this study, the most common cause of second-look hip arthroscopy was incomplete osteoplasty for FAI.25) Incomplete osteoplasty means that the femoral neck junction is less shaved than the length of the burr of 5 mm, and the femoral head is hooked to the acetabular labrum when the hip is flexed 70°–80°. It can be also assessed with postoperative radiographs where the alpha angle is > 55° and offset is ≤ 9 mm. In cases of labro-synovial adhesion in revisional arthroscopic procedures, incomplete femoroplasty with an alpha angle of 64.5° and offset of 7.8 mm was shown in radiographs after primary arthroscopic procedure; this, it is considered that complete femoroplasty may be important to prevent labro-synovial adhesion (Fig. 3).
Several studies have described failure rates of labral tear repair. Gupta et al.26) reported a 9% conversion to THA following hip arthroscopy. Sawyer et al.27) reported the rate of conversion to THA was 2% in patients with > 2 mm of joint space who underwent labral repair. Harris et al.28) reported a 2.9% conversion to THA following hip arthroscopy. Menge et al.24) reported that 34% of patients had conversion to THA due to < 2 mm of joint space preoperatively. On the other hand, our THA conversion rate (2.4%) was very low compared to others. In our THA conversion case, the patient already had early osteoarthritic changes (Tönnis grade 1) with cartilage defect and had a borderline dysplasia of the hip where the lateral center edge angle was 24.8°, which could have affected the development and progression of OA. Unlike other studies, we narrowed indications for arthroscopic treatment. Only those with normal or below Tönnis grade 1 were included, which could be the reason to have a lower THA conversion rate in our study.
Except the one THA conversion case, other cases did not have significant changes in the Tönnis grade in the long-term follow-up (Fig. 4). Therefore, it could be estimated that the arthroscopic labral repair technique could help stabilize the hip joint and delay progression of osteoarthritic changes in the long-term follow-up. Additional revision arthroscopic procedures and conversion to THA were performed, but the survivorship rate remained above 85% at the last follow-up. Theses outcomes demonstrated the effectiveness of the arthroscopic labral repair technique.
Our study has a few limitations. First of all, this study does not have a control or comparison group who underwent labral debridement or conservative therapy. Second, after arthroscopic labral repair, we educated the patients on life style modifications (downgrade for activities and exercise sports). That may also be related to the improvement in clinical scores and delay of the progression of OA. Last, we performed not only labral repair but also femoroplasty or acetabuloplasty, synovectomy, ligamentum teres debridement and so on. In particular, femoroplasty or acetabuloplasty could affect clinical results during the follow-up because it is effective for improving range of motion and decreasing symptomatic pain caused by impingement.
The clinical and radiological long-term follow-up revealed that most cases of arthroscopic management of FAI and labral tears maintained improvement of outcome without progression of significant arthritis. Because of the importance of the main function of the labrum, we recommend labral repair for symptomatic acetabular labral tears. Anatomical recovery of acetabular labrum was associated with the improvement of clinical symptoms.





 XML Download
XML Download