

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Acetabular labral and cartilage lesions in femoroacetabular impingement are considered causal factors of early-onset osteoarthritis.1) Recent improvements in the quality of computed tomography (CT) arthrography (CTA) with multi-detector CT (MDCT) with submillimeter spatial resolution has increased the use of CTA for evaluating the cartilage, ligament, and labral lesions in various joints.234) Although several recent studies have documented the use of magnetic resonance imaging (MRI) for diagnosing acetabular labral and chondral lesions, validation data have been inconsistent.567) In addition, there has been only one study examining the diagnostic sensitivity and specificity of MRI and CTA in dysplastic hip joints.4) The purpose of this study was to investigate the sensitivity, specificity, and accuracy of MRI and CTA for diagnosing acetabular labral tears using the Lage classification system8) and chondral lesions compared with arthroscopic findings.
METHODS
The design and protocol of this retrospective study were approved by the Institutional Review Board of Chung-Ang University Hospital (IRB No. C2014078(1274)) and informed consent was waived.
Patient Selection
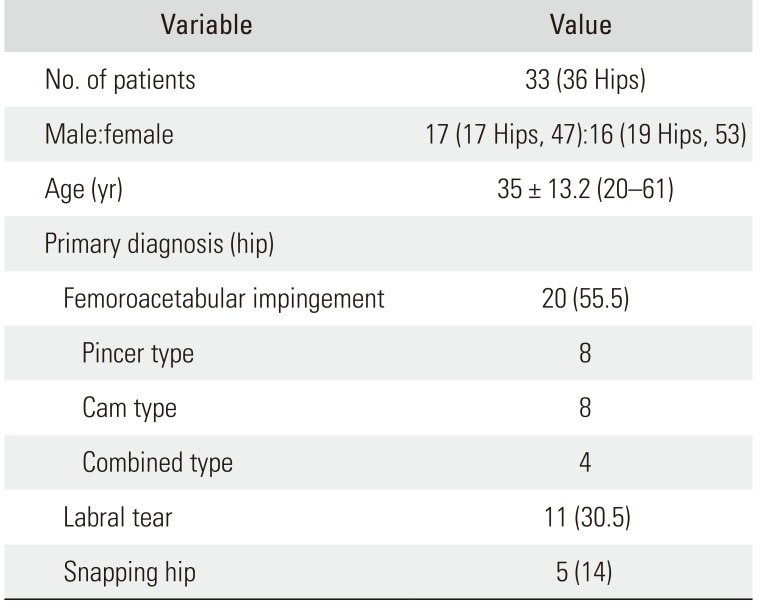
A retrospective review of 33 patients (36 hips) who underwent MRI and direct CTA of the hip and arthroscopic surgery from January 2010 to December 2014 was conducted. The inclusion criteria were patients who had groin pain and positive results on the impingement test or the flexion, abduction, and external rotation test and patients who underwent arthroscopic surgery within 2 months after CTA. The 33 patients (36 hips) comprised 17 males (17 hips, 47%) and 16 females (19 hips, 53%). The mean age of the patients at the time of diagnosis was 35 years (range, 20 to 61 years). None of the patients had previously undergone surgery on the ipsilateral hip joint. The demographic features of the patients including age, sex, and primary diagnosis are presented in Table 1.
MRI Protocol
MRI was performed on a 1.5-T (20 patients; Philips Medical Systems, Best, the Netherlands; Siemens Medical Solutions, Erlangen, Germany; GE Healthcare, Milwaukee, WI, USA) or 3.0-T (13 patients; Philips Medical Systems) scanner. The MRI protocol included three imaging planes except one patient. Axial, sagittal, and coronal images were obtained with T1-weighted image (T1WI) or T2WI or proton density weighted image (PDWI) sequences. T2WI and PDWI were with or without fat saturation. The ranges of repetition time and echo time were variable (404–1,041/8–20 ms for T1WI, 2,120–9,063/23–118 ms for T2WI fat spin echo and 1,700–3,500/10–40 ms for PDWI). Other imaging parameters were as follows: matrix, 224 × 224–512 × 512; field of view, 22–43 cm; slice thickness, 3–8 mm; and number of signals averaged, 1 or 2.
CTA Protocol
Under ultrasound guidance, a 21-G spinal needle was placed in the hip joint by an anterior approach using a standardized aseptic technique. A total of 10–12 mL mixture of 10 mL iopamidol and a solution of 5 mL of normal saline and 0.3 mL 2% lidocaine was injected into the hip joint. CT scans were obtained with a 16-slice MDCT or 256-slice MDCT with standard acquisition protocols as follows: for 16-channel MDCT, pitch, 0.938; current, 10–40 mAs; voltage, 120 kVp; collimation, 10 mm; field of view at acquisition, 15–20 cm; slice thickness, 2.5 mm without section overlapping; and matrix size, 512 × 512; for 256-channel MDCT, pitch, 0.579; current, 200–300 mAs; voltage, 120 kVp; collimation, 40 mm; field of view at acquisition, 15–20 cm; slice thickness, 2.5 mm without section overlapping; and matrix size, 512 × 512. Coronal, sagittal, and oblique axial images (parallel to the femoral neck axis) were routinely reconstructed using an EBW 4.5 workstation after axial scanning.
Image Analysis
Two experienced musculoskeletal radiologists (GYL and SK) independently reviewed the MRI and CTA scans in random order. After two radiologists came to consensus during review sessions, each examiner was blinded to other measurements and arthroscopic findings. The observers repeated the measurements in separate sessions.
MRI Interpretation
All images were evaluated for the presence of a labral tear and cartilage lesion. Labral abnormalities were classified into three types using an established classification system2910) as follows: type 1 (radial flap tear), a tear with a discrete linear high signal intensity extending either partially or all the way through the labral substance, creating a flap; type 2 (radial fibrillated tear), irregular margins of the labrum without a discrete tear; and type 3 (longitudinal peripheral or base tear), a tear with a linear high signal intensity extending partially or completely between the labral base and acetabulum labral detachment. The cartilage lesion was graded using a 3-point scale: 1, complete visualization-sharp edges; 2, blurred edges fissuringpartial defects; and 3, exposed bone.11)
CTA Image Interpretation
An acetabular labral abnormality was diagnosed when the inflow of contrast medium was observed to be continuous with the joint space at the base of the acetabular labrum.12) Labral blunting, displacement, or intrasubstance contrast material were also considered a tear. Linear contrast material at the acetabular-labral junction also indicated a tear if the margins were irregular or a sublabral sulcus if the margins were smooth.
Each labral tear or detachment on CTA was then classified by Blankenbaker modification of the Lage arthroscopic classification.289) Tears were classified as arthrographic Lage type 1, 2, 3, or 4. A type 1 tear (radial flap tear) was diagnosed on CTA if a discrete contrast cleft was seen extending either partially or all the way through the labral substance creating a flap. A type 2 tear (radial fibrillated) was diagnosed if there was irregularity of the labral outline, but no discrete cleft within the labrum. A type 3 tear (longitudinal peripheral) was diagnosed when there was contrast extending through the labrum either very near or at the junction between the labrum and the acetabulum. A type 4 unstable tear was diagnosed if the labrum had a thickened and distorted appearance. These criteria have their limitations because a torn labrum often becomes thickened and distorted when it is unstable, whereas not all unstable tears are thickened. Such tears were classified into the most closely appropriate type.
Arthroscopy
Thirty-six hips underwent arthroscopic surgery within 2 months after CTA. A single arthroscopic surgeon (YCH) performed all operations using a technique described by Byrd.1314) A tear was identified by passing a hook between the labrum and the subchondral bone. Two experienced orthopedic surgeons who were not involved in the preoperative image evaluations (SHB and ECJ) took part in each operation and arrived at a consensus on the interpretation of the arthroscopic findings during and after surgery using movie clips and photos.
Statistical Analyses
Both orthopedic surgeons who were not involved in the image evaluation assessed the arthroscopic findings and compared with the MRI findings and CTA findings to evaluate sensitivity, specificity, and accuracy of MRI and CTA. Inter- and intraobserver reliabilities for the measured parameters including labral tears and chondral lesions in 36 hips were assessed using Kappa coefficients. These were interpreted as follows: 0.00–0.20, poor; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, substantial; and > 0.80, almost perfect agreement.15) The Kappa coefficient method was used for statistical analysis of comparison of MRI classification and modified CT classification of the Blankenbaker with the arthroscopic findings of the Lage arthroscopic classification.
Chi-square or Fisher exact test was used to compare arthroscopic findings with the acetabular labral lesions and chondral lesions observed on CTA and MRI. We used SAS ver. 6.2 (SAS Institute, Cary, NC, USA). Statistical significance was defined as a p-value < 0.05.
RESULTS
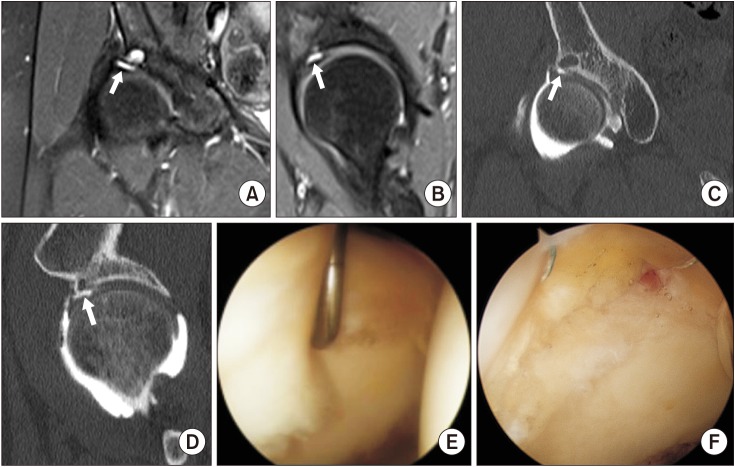
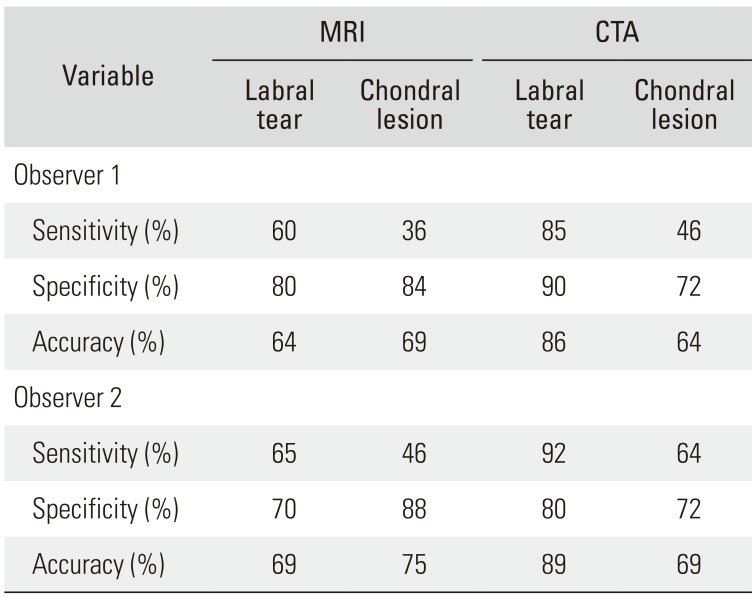
Arthroscopy of the 36 hips revealed an acetabular labral tear in 26 hips and no abnormality in 10 hips. MRI and CTA of the 36 hips revealed an acetabular labral tear in 17 hips and 23 hips, respectively, for observer 1 (p = 0.032) and in 21 hips and 26 hips, respectively, for observer 2 (p < 0.001). The sensitivity, specificity, and accuracy of MRI for detection of labral tears were 60%, 80%, and 64%, respectively, for observer 1 and 65%, 70%, and 69%, respectively, for observer 2 (Table 2). The sensitivity, specificity, and accuracy of CTA for detection of labral tears were 85%, 90%, and 86%, respectively, for observer 1 and 92%, 80%, and 89%, respectively, for observer 2 (Table 2 and Fig. 1).
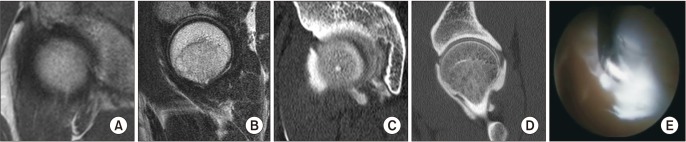
Arthroscopy of the 36 hips revealed chondral lesions in 11 hips, including a carpet lesion without cartilage defect in two hips and cartilage defects in seven hips. On MRI and CTA of 36 hips, a chondral lesion was found in eight hips and 12 hips, respectively, for observer 1 (p = 0.369) and in eight hips and 14 hips, respectively, for observer 2 (p = 0.050). The sensitivity, specificity, and accuracy of MRI for detection of chondral lesions were 36%, 84%, and 69%, respectively, for observer 1 and 46%, 88%, and 75%, respectively, for observer 2 (Table 2). The sensitivity, specificity, and accuracy of CTA for detection of chondral lesions were 46%, 72%, and 64%, respectively, for observer 1 and 64%, 72%, and 69%, respectively, for observer 2 (Table 2 and Fig. 2).
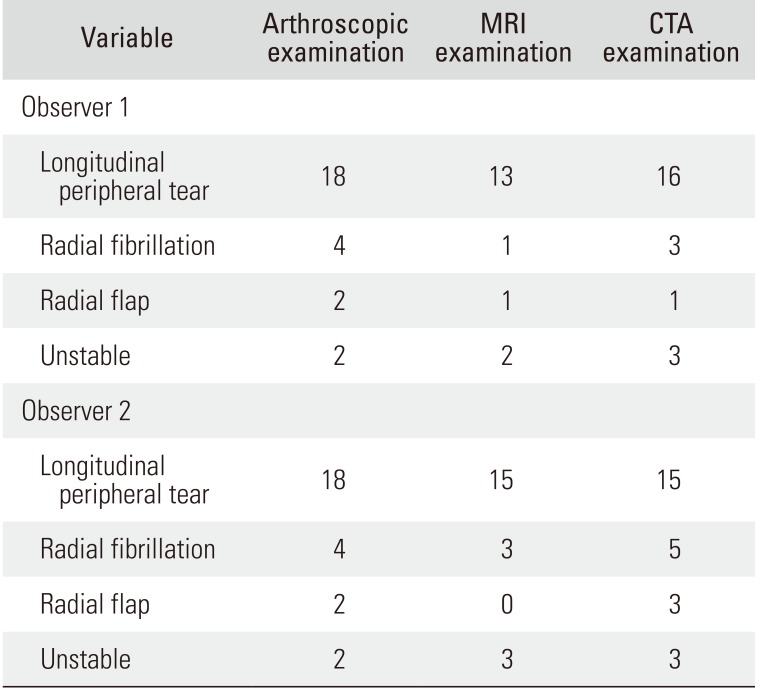
According to the Lage morphologic classification, arthroscopic examination revealed longitudinal peripheral tears in 18 hips, four radial fibrillated tears, two radial flaps, and two unstable tears. The MRI findings of observer 1 include 13 hips with longitudinal peripheral tears. The CTA findings of observer 1 include 16 hips with longitudinal peripheral tears, three radial fibrillated tears, one flap tear, and three unstable tears (Table 3). Compared to the morphologic classification based on arthroscopic findings, the accuracy of MRI was 53% for observer 1 and 62% for observer 2; the accuracy of CTA was 65% for observer 1 and 72% for observer 2.
Intraobserver reproducibility for MRI detection of labral tears and chondral lesions was substantial (κ = 0.756 and κ = 0.693, respectively). Interobserver reliability for MRI detection of labral tears and chondral lesions was substantial (κ = 0.700 and κ = 0.875, respectively). Intraobserver reproducibility for CTA detection of labral tears and chondral lesions was substantial (κ = 0.832 and κ = 0.774, respectively). Interobserver reliability for MRI detection of labral tears and chondral lesions was substantial (κ = 0.886 and κ = 0.596, respectively).
DISCUSSION
Many clinicians recommend MRI for evaluating hip pathologies due to the convenience of the examination and less invasiveness than magnetic resonance arthrography (MRA).5111617) However, the diagnostic value of MRI for acetabular labral and chondral lesions is not consistent.56717) CTA has high merits for diagnosing acetabular labral lesions.23) This is the first study that compared CTA with MRI. This comparative study has demonstrated higher sensitivity, specificity, and accuracy of CTA than MRI for detection of acetabular labral lesions. However, the diagnostic value of both CTA and MRI for detection of chondral lesions was unsatisfactory.
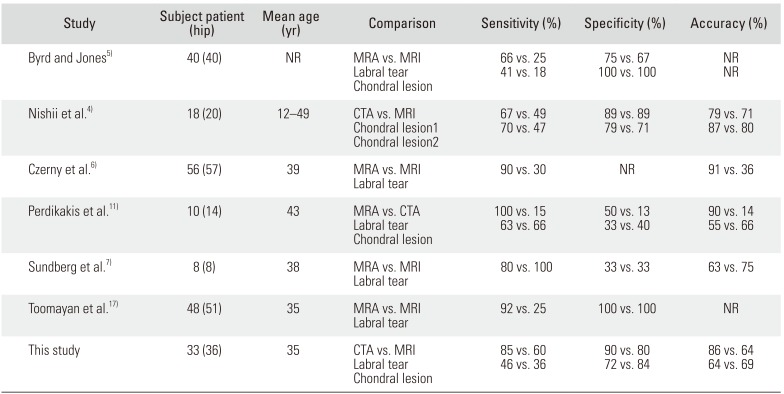
Sundberg et al.7) reported that the diagnostic value of MRI for acetabular labral lesions was comparable to MRA. They performed a comparative study using 1.5-T MRA and 3.0-T MRI for evaluating the acetabular labrum. They reported 100% sensitivity for MRI and 80% sensitivity for MRA. However, other studies have reported better sensitivity (range, 66% to 100%) and specificity (range, 50% to 100%) of MRA than MRI for acetabular labral lesions.5617) In addition, there is no comparative study between CTA and MRI for acetabular labral lesions. Our results show that the diagnostic value of CTA is significantly better than MRI for acetabular labral tears.
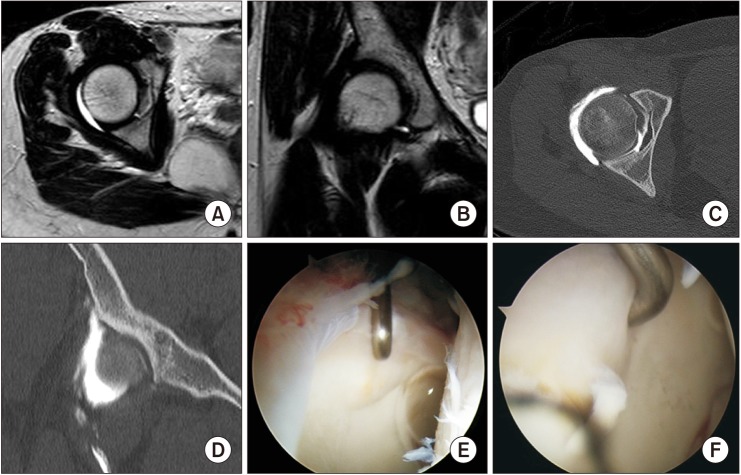
Many studies have reported better outcomes of early surgical intervention in patients with early-stage osteoarthritis.181920) Therefore, detecting acetabular cartilage lesions at an early stage is important to establish an appropriate treatment plan. Although MRI and MRA remain the imaging techniques of choice to detect cartilage lesions, their diagnostic values to detect chondral lesions were limited (Table 4). In our study, the sensitivity and accuracy of CTA to detect chondral lesions were better than those of MRI. However, the sensitivity and accuracy of CTA for evaluating chondral lesions were 50% and 70%, respectively (Table 4). We performed an evaluation to identify the reasons. Two hips showed normal cartilage conditions on both CTA and MRI. However, arthroscopic findings showed no cartilage defects or loss but carpet lesions (Fig. 3).21) Nishii et al.4) performed a comparative study using fat-suppressed three-dimensional fast spoiled gradientecho MRI and MDCTA. They evaluated cartilage lesions of 20 hips with acetabular dysplasia and reported that sensitivity and specificity of MRI and CTA for detecting any cartilage disorder without cartilage defects were 49% and 67%, and 89% and 89%, respectively, and sensitivity and specificity of MRI and CTA for detecting cartilage lesions with substance loss were 47% and 70%, and 92% and 93%, respectively. Therefore, conventional methods including MRA, MRI, and CTA may not be appropriate diagnostic methods if there were not cartilage defects.
Several limitations in this study should be noted. First, this study is a retrospective review of 36 hips that has a relatively low number of cases, and there is a possibility of selection bias. Second, all patients were symptomatic with mechanical hip pain and had a clinical suspicion of labral tears and chondral lesions. Therefore, the two radiologists may have presumed the presence of an acetabular labral tear or a chondral lesion during interpretation. Finally, MRI on nine patients (nine hips) performed at outside institutions may not have the same quality, negatively influencing the results.
This study demonstrated that the accuracy of MRI to evaluate an acetabular labral tear and chondral lesion of the hip joint was not sufficient. CTA was a reliable method in the diagnosis of acetabular labral tears. However, CTA and MRI are also of limited value to detect chondral lesions.
 XML Download
XML Download