

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is regarded as a major cardiac arrhythmia that is characterized by very fast and irregular heartbeats of the atria. AF prevalence is estimated at 2.3 million in the US and 4.5 million in the European Union,1 and it is expected that the number of AF patients in the US will increase by 2.5 times by 2050. Undiagnosed and untreated AF can be a risk factor for dizziness,2 dyspnea,3 or stroke.4 In the worst possible case, AF patients may die due to a sudden cardiovascular problem. Furthermore, the economic and clinical burden of AF is substantial due to the hospitalization and healthcare service. Therefore, the prediction of AF is significant clinically and economically.56
There are three types of AF: paroxysmal, persistent, and chronic. Paroxysmal and persistent AF show similar occurrences during several minutes to days. The difference being that paroxysmal AF can self-terminate, but persistent AF cannot stop by itself without treatment. The heartbeat cannot return to normal after chronic AF, even with treatment.7 An electrocardiogram (ECG) is vital for objectively representing the presence or absence of AF. To diagnose and predict the AF, an ECG signal is collected during the long-term (less than 48 hours) by cardiac monitoring devices, such as event recorders or/and a Holter monitor. After recording the subject's ECG signal, it is visually inspected by a certified clinician to determine the AF-related patterns or abnormal waveforms in morphology.8 However, there are limitations in the automatic prediction of AF, including the fact many AF patients display no symptoms, paroxysmal and persistent AF patients can be missed in many studies, visual inspection is time consuming, and an accurate annotation of an ECG requires extensive training and experience.9
In recent years, several studies have proposed methods for the automatic prediction of AF using an ECG signal. All of these proposed methods attempt to solve the drawbacks of the conventional methods used for the automatic prediction of AF. In general, they analyzed the characteristics of an ECG, including the P-waves,101112 R-R interval,13141516 and both the P and R waves,1718 to extract the parameters and features that rely on AF episodes. Then, the extracted parameters were applied to various classifiers, such as a support vector machine (SVM), and a generic algorithm was used to predict or/and diagnose the AF. However, all the parameters and features related to AF were hand-crafted. In addition, P-waves and R-R intervals are easily contaminated with motion and noise artifacts, leading to a reduction in the performance of the algorithms that predict AF. Finally, there are few studies that analyze the short-term ECG (less than 60 seconds), however their results were not satisfactory.
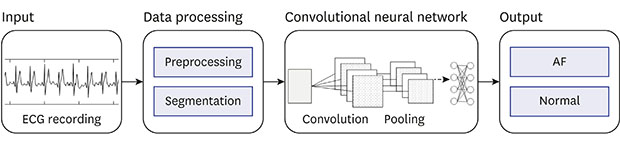
The convolutional neural network (CNN) method is the most well-known model of deep learning. Recently, the robust performances of various applications of biomedical engineering have been demonstrated, including medical imaging,19 gene recognition,2021 speech processing,22 and sleep apnea detection.23 CNN can analyze the morphological characteristics and learn the slit variation of an input signal during a short-term ECG.24 Therefore, we propose a method for the automatic prediction of AF based on the CNN model using a short-term normal ECG signal (Fig. 1). The proposed method can predict the subject who is AF patient or normal by using short-term normal ECG signal. For this, short-term normal ECG signal was randomly selected at the arbitrary section of ECG recording from the three different databases. In addition, the proposed CNN model will evaluate the lengths and numbers of normal ECG segments. Finally, the results of the evaluation performances for the proposed CNN model will be compared with those of the conventional methods.

METHODS
Data collection
The short-term normal ECG signal is the main input of the proposed method for the automatic prediction of AF based on the CNN model. The inputted ECG signal was collected from two AF datasets and one normal ECG dataset, including the MIT-BIH Atrial Fibrillation Database (AFDB), the Paroxysmal Atrial Fibrillation Prediction Challenge Database (PAFDB), and the MIT-BIH Normal Sinus Rhythm Database (NSRDB) provided by PhysioNet.25 The AFDB consists of 23 annotated records of ECGs from a Holter monitor of AF patients with a sampling frequency of 250 Hz. Each record has a duration of about 10 hours and the total dataset has less than 230 hours of data. The database contains 605 annotated episodes, including 317 AF episodes with an average duration of 115 seconds and 288 normal rhythms with an average duration of 174 seconds. However, two records were excluded since there was not enough information about the annotation. The PAFDB is used to develop the prediction algorithm of AF and comprises ECG records with 30 minutes prior to a sudden AF occurrence. The NSRDB has ECG records from 18 normal subjects with a 25 hours duration. Detailed information of the three datasets is presented in Table 1.
Table 1
Dataset information in detail

| Databases | Time, min | AF, records | Normal, records | Sampling, Hz |
|---|---|---|---|---|
| MIT-BIH AFDB | 600 | 21 | 0 | 250 |
| PAFDB | 30 | 53 | 47 | 128 |
| MIT-BIH NSRDB | 1,500 | 0 | 18 | 128 |
| Total | 2,130 | 74 | 65 | - |
AF = atrial fibrillation, AFDB = Atrial Fibrillation Database, PAFDB = Paroxysmal Atrial Fibrillation Prediction Challenge Database, NSRDB = Normal Sinus Rhythm Database.
![]()
Data processing and segmentation
The ECG signals were preprocessed for the training and evaluation of the proposed method for the automatic prediction of AF based on the CNN model. For preprocessing, a band-pass filter and discrete wavelet transform were used to eliminate the baseline wandering and high-frequency components of the ECG signals.26 A ‘haar’ mother wavelet was employed for the wavelet generating function.27 The sampling rate of the ECG signals matched 120 Hz, since these were from three different ECG datasets, then all ECG signals were segmented into a 30 seconds duration. The short-term normal ECG signal contains approximately fifteen normal heart beats as the presented Fig. 2. After segmentation, we obtained 19,804 short-term normal ECG segments that consisted of 11,882 segments from AF records and 7,922 segments from normal records, respectively. Then 80% of the total ECG segments were used for the training set, and 20% of the total segments were used as the test set. All procedures of signal processing and segmentation for the dataset were performed randomly using MATLAB 2017a (Mathworks, Natick, MA, USA).

CNN
CNN model was designed for the automatic prediction of AF using a short-term normal ECG. The CNN consists of three major layers: a convolutional layer, a pooling layer, and fully-connected layers. First, the convolutional layer generates intermediate feature maps by combining the whole input signal using various kernels. In the convolutional layer, we used one-dimensional (1D) convolution since the input ECG signal is a 1D time series. 1D convolution can be expressed by equation 1 as below:

where xk is the k-th feature map, bk is the bias of the k-th feature map, wk is the k-th convolutional kernel from all features of the k-th feature map, and yi represents the i-th feature map. Secondly, the pooling layer reduces the size of the intermediate feature maps to select representative features. We used the max-pooling in all pooling layers to reduce the intermediated feature maps. Lastly, the fully-connected layer consists of a fully-connected multilayer perceptron (MLP) and softmax activation function to final discrimination of the CNN model.28
In addition, we used some other functions for designing the CNN model to avoid divergence and optimization including batch-normalization, dropout, and a rectified linear unit (ReLU). Batch-normalization was applied to the input ECG records before training the CNN model,29 as presented in equation 2:

Where ε- is a small random noise, μ- is the mini-batch mean, σ- is the mini-batch variance, α denotes a scale parameter, and β represents a shift parameter. Both α and β are trainable and updated in an epoch-wise manner. Dropout is a technique used to avoid overfitting and divergence.30 ReLU is used as the function of the activation layer, which robustly improved the activation function of the deep learning. ReLU showed a robust training performance and consistent gradients, thereby aiding gradient-based learning.31
Implementation and optimization
To implement the proposed deep CNN model, the software Python 3.5 on the Keras library (Tensor-Flow background) was used. Then, the implemented deep CNN model was trained and evaluated using graphics processing unit (GeForce GTX1080 TI; Nvidia, Santa Clara, CA, USA) computing in a Windows 10 environment. The training of the implemented deep CNN model for AF prediction was fully-supervised, back-propagating the gradients from the fully-connected layer through to the convolutional layers. The model parameters were optimized by minimizing the binary cross-entropy as a loss function that used gradient descent with the Adam update rule.32
Optimal architecture selection
For the proposed CNN model for the automatic prediction of AF using a short-term normal ECG, an optimal architecture of CNN model was selected thru the heuristic experiments. To find the optimal architecture of the proposed CNN model, three to thirteen layers of convolutional, pooling, and MLP were designed. According to the results of the experiments for optimal architecture selection, the CNN model shows a greater performance in deeper architecture, as shown in Table 2.
Table 2
Performances of CNN model according to the number of convolutional layers

| Measures, % | No. of layers | |||||
|---|---|---|---|---|---|---|
| 3 | 5 | 7 | 9 | 11 | 13 | |
| Sensitivity | 88.0 | 91.0 | 99.0 | 99.0 | 100.0 | 100.0 |
| Specificity | 87.0 | 88.0 | 99.0 | 99.0 | 100.0 | 100.0 |
| Accuracy | 87.4 | 88.2 | 99.3 | 99.0 | 99.6 | 99.7 |
![]()
In Fig. 3, the optimal architecture (seven-layer) of the proposed CNN model is presented, including the detailed parameters in each layer. It used a short-term normal ECG segment length of 30 seconds (900 × 1) duration as the input of the first layer. Batch-normalization was used to reduce the internal covariance shift prior to the input data to the first layer, and 1D convolution (kernel 8 and stride 1) was applied to the first and second layers. Next, in the following order, max-pooling, 1D convolution, 1D convolution, max-pooling, and MLP, was iterated twice. For all the max-pooling, kernel size 2 and stride 2 were applied, and then dropout was used with a 25% ratio. In the first iteration, kernel size 4 and stride 1 convolution was applied, whereas, in the second iteration, kernel size 2 and stride 1 convolution was applied. In the last layer, softmax was used for the final classification, and the AF was predicted via the inputted short-term normal ECG. The number of all parameters after passing through all layers was 11,150; moreover, 200 epochs were used in the training process, and the batch size used was 2.

Data analysis
The accuracy, the sensitivity, and the specificity were calculated as the data analysis to compare the performance of the proposed CNN model. A cross-validation was performed to evaluate the proposed method for the short-term normal ECG dataset. The evaluation measures are expressed as follows: Accuracy = (TP + TN)/(TP + TN + FP + FN); Sensitivity = TP/(TP + FN); Specificity = TN/(TN + FP), where a true positive (TP), true negative (TN), false positive (FP), and false negative (FN) refer to the number of events in which normal is classified as normal, abnormal as abnormal, abnormal as normal, and normal as abnormal, respectively.
RESULTS
The results of the performance evaluation of the proposed method for the automatic prediction of AF based on the CNN model are presented as below. The performances were evaluated on the records of 74 subjects, and were tested on 65 subject's records. The short-term normal (less than 60 seconds) ECG signal was analyzed to find the optimal length and number of segments, the experiment results of which are shown in Tables 3 and 4. At first, the proposed CNN model was trained by training segments of different lengths as 10–60 seconds with 10 seconds interval. Then, we trained the proposed CNN model by increasing the number of training sets. The results show a relatively high performance at 30 seconds duration segments, and more training segments increases the performance.
Table 3
Performances of CNN model according to the length of training segments

| Measures, % | Length of segments, sec | |||||
|---|---|---|---|---|---|---|
| 10 | 20 | 30 | 40 | 50 | 60 | |
| Sensitivity | 82.5 | 90.0 | 90.9 | 85.6 | 90.6 | 94.1a |
| Specificity | 83.9 | 82.6 | 92.7a | 92.4 | 90.0 | 90.1 |
| Accuracy | 83.4 | 84.9 | 92.2a | 90.3 | 90.2 | 91.4 |
![]()
Table 4
Performances of CNN model according to the number of training segments

| Measures, % | No. of segments | ||||
|---|---|---|---|---|---|
| 400 | 800 | 1,500 | 2,200 | 3,000 | |
| Sensitivity | 94.5 | 92.4 | 97.4 | 98.8 | 99.2 |
| Specificity | 94.5 | 98.0 | 99.4 | 99.6 | 99.8 |
| Accuracy | 92.5 | 94.4 | 97.4 | 98.8 | 99.2 |
![]()
Seven-layer architecture was selected as an optimal architecture of the proposed CNN model for the automatic prediction of AF. Our final results were performed by the optimal architecture of the proposed CNN model for the automatic prediction of AF, as presented in Table 5. For the training set, evaluation measures showed with an accuracy of 99.2%, a sensitivity of 99.8%, and a specificity of 99.2%; 98.7%, 98.6%, and 98.7% for the test set, respectively. According to the Table 2, the proposed CNN model achieved a 100% performance at more than 11-layer architecture in training set but not test set. Therefore, more simple and robust architecture was selected as an optimal architecture of the CNN model for AF prediction. That is why a final performance of the training set is not achieved 100%.

DISCUSSION
In this study, we investigated the method for automatic prediction of AF based on CNN model using a short-term normal ECG signal. The arbitrary normal ECG signal was applied to the proposed CNN model and automatically predicting that the source of the ECG signal was an AF or a normal subject. We obtained the performances with a mean sensitivity of 98.7%, specificity of 98.6% and accuracy of 98.7% for the automatic prediction of AF, demonstrating the usefulness of the CNN model for AF prediction and detection.
Several methods have been presented to predict AF by analyzing ECG related parameters including the P-wave, RR interval, and heart-rate variability (HRV). Most studies analyzing various handcrafted features used HRV obtained through a single-lead ECG signal. Table 6 summarizes the performances of the previous studies and the proposed method for the prediction of AF. A previous study33 predicted AF using 14 features from HRV including spectrum, bispectrum, and non-linear features. Then, the SVM was used as classifier, which is popular machine-learning method, and they obtained a sensitivity, specificity, and accuracy of 96.2%, 93.1%, and 94.5%, respectively. However, their results were obtained using only 30 minutes data that were obtained prior to the rapid AF occurrence, whereas the present study can be more effective since we analyzed short-term normal ECG segments where no AF occurred. In addition, the proposed CNN model does not use the handcrafted features from HRV and obtained higher performances.
Table 6
Performance comparison between the proposed method and previous studies

| Studies | Method | Duration | Sensitivity, % | Specificity, % | Accuracy, % |
|---|---|---|---|---|---|
| Thong et al.8 | PACs analysis | 30 min | 89.0 | 91.0 | 90.0 |
| Mohebbi et al.33 | HRV features, SVM | 30 min | 96.2 | 93.1 | 94.5 |
| 10 min | 75.1 | 64.3 | 69.6 | ||
| Boon et al.34 | HRV features, SVM | 15 min | 85.2 | 82.1 | 83.9 |
| 30 min | 96.4 | 71.4 | 83.9 | ||
| This study 2018 | CNN | 30 sec | 98.7 | 98.6 | 98.7 |
![]()
In study,34 10, 15, and 30 minutes ECGs were analyzed based on the HRV analysis with genetic algorithm and SVM. They extracted 55 features from HRV using time domain, frequency domain, and non-linear analysis. The genetic algorithm was used to optimize the feature selection for enhancement of discrimination power. Finally, they obtained relatively good performances for the 30 minutes ECG analysis. However, they showed lower performances with a sensitivity, specificity, and accuracy of 75.1%, 64.3%, and 69.6%, respectively, for the 10 minutes ECG analysis. In contrast, the proposed CNN model showed superior performances than the results of the previous studies.
In this study, we propose a CNN model for the automatic prediction of AF using a short-term normal ECG, found an optimal architecture of the CNN model, and demonstrated the optimal length of short-term ECG segments. The proposed CNN model can eliminate not only the handcrafted feature extraction from HRV using complex and various domain analyses but is also easy to implement and performs robustly for the automatic prediction of AF. However, there are some limitations in the proposed CNN model. First, we cannot detect the starting point of AF, we can predict AF segment before the 30 seconds. Second, only potential AF for the subjects could be predicted by the proposed method. Finally, we used small dataset that provided MIT-BIH database.
In conclusion, we demonstrated a method for the automatic prediction of AF using a short-term normal ECG based on the CNN model. We obtained a high prediction accuracy of 98.7%. This result presented the possibility of a more accurate prediction and diagnosis for AF patients. In further studies, the proposed CNN model should be trained with various types of ECGs from patients suffering from arrhythmia as well as a large number of patients' ECGs.
 XML Download
XML Download