

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Tuberculosis (TB) has remained a serious public health issue in the Korea.1 Despite the public health authority's efforts to control TB, the incidence rate in 2017 was 77/100,000. This is about 25 times the incidence rate in the United States and about 5 times that in Japan.2 About 90% of TB patients in the Korea are undergoing proper treatment at a health care institution; however, a considerable number of healthcare workers (HCWs) and patients are consistently exposed to TB, owing to the high density of the country's population with active TB.3
Exposure to TB in a healthcare institution may be a result of the high prevalence of visitors to the institution with infectious TB; over-crowding; the effectiveness of institutional preparedness; and the lack of prompt microbiological identification, patient isolation, and TB treatment by the TB infection control program.4 Since 2006, our university hospital has run a multidisciplinary team called the “Soonchunhyang Committee for the Control and Elimination of TB (SCET),” a specialized group in institutional TB control that collaborates with the government (Public-Private Mix [PPM]). SCET interventions include notification of any new positive culture for TB, monitoring the initiation of anti-TB medication, and compliance of treatment.5 Despite the work of SCET to minimize exposure associated with the unexpected confirmation of TB among patients presenting with non-tuberculous clinical manifestations, continuous in-hospital exposure to TB still exists.
In this study, we present the results of an aggressive contact investigation strategy in a university hospital after in-hospital exposure of inpatients, visitors, and HCWs to active pulmonary TB, allowing us to determine the rate of newly identified latent tuberculosis infection (LTBI) and active pulmonary TB. In addition, we investigated the workload of infection control practitioners (ICPs) for this contact investigation.
METHODS
Characteristics of our institution
Soonchunhyang University, Seoul Hospital is a 734-bed teaching university hospital located in Seoul, Korea. There is a 28-bed intensive care unit (ICU) and an 8-bed neonatal ICU. At the time of study initiation (August 2016), the total number of HCWs in our hospital was 1,538. The infection control team consists of 5 ICPs.
SCET is a multidisciplinary team for sustained action against TB that consists of infectious disease specialists, pulmonologists, clinical microbiologists, pediatricians, microbiologists, family medicine physicians, laboratory technicians, PPM nurses, and ICPs. As we previously reported, about 90 patients with culture-positive pulmonary TB were admitted to our institution each year.5 Our institution has an air exchanging system that is used more than 6 times an hour in patient rooms and 20 times an hour in the ICU.
Identification of index patients
As part of infection control practice, we prospectively screened all adult patients with active pulmonary TB who were admitted to our hospital between August 2016 and April 2017. Active pulmonary TB was microbiologically diagnosed by a positive acid-fast bacilli (AFB) stain, confirmation of Mycobacterium tuberculosis in culture, or positive TB polymerase chain reaction (PCR) of respiratory specimens.6 If the diagnosis came from a positive TB PCR result, a pulmonologist validated the clinical significance and infectivity of the case. Close contact was defined as a person (patient, visitor, or HCW) exposed to an active pulmonary TB patient for more than 8 consecutive or 40 cumulative hours, or a person engaged in an aerosol production procedure without respiratory protection for any duration.78 The definition of time to isolation was the interval from admission of the index patient to isolation.
Identification of TB exposure and intervention
In August 2016, we initiated an investigation of all inpatients, visitors, and HCWs exposed to TB. This new strategy was far more aggressive than previous ones which only investigated exposed HCWs and immunocompromised patients. Patients were considered immunocompromised if they were on anti-cancer treatment; had received a stem-cell transplantation within the past year or a solid organ transplant; had a hematologic malignancy or undergone a splenectomy; were human immunodeficiency virus infected with CD4 cells/mm3 < 200; exposed to steroids for more than 2 weeks at a prednisolone dose > 40 mg per day or equivocal; or under the age of 12.
The infection control team investigated all exposure events among HCWs, inpatients, and visitors. Chest radiographs were advised to all close contacts immediately and 3 months following exposure (Supplementary Fig. 1). A tuberculous skin test (TST) or interferon gamma releasing assay (IGRA) was additionally recommended for all close contact HCWs and immunocompromised patients immediately and 3 months following exposure.9 When an exposed HCW demonstrated a positive result of TST or IGRA without active TB lesions in chest radiographs within 3 months, we considered it an immediate LTBI test result.
All exposed patients and visitors were interviewed, examined by 3 infectious disease specialists, and had chest radiographs 3 months following exposure. Any HCWs with a positive IGRA or TST conversion were referred to a pulmonologist to exclude active pulmonary TB and to begin treatment for LTBI.
TST and IGRA
The TST was performed according to the Mantoux method. A 2-tuberculin unit of tuberculin purified protein derivative (Statens Serum Institute, Copenhagen, Denmark) was injected intradermally and the induration size was read after 48 to 72 hours by a trained technician. A TST conversion was defined as an erythematous induration ≥ 10 mm and an increase ≥ 6 mm after the baseline negative TST result.10 An IGRA, the QuantiFERON-TB Gold in-tube (QFT-GIT) test, was performed according to the manufacturer's instructions. A positive result was defined as an interferon-concentration ≥ 0.35 IU/mL and ≥ 25% of the negative control.11
Estimation of ICP's work load for contact investigation
Two ICPs investigated all close contact inpatients, visitors, and HCWs during the study period, but the amounts of time the 2 ICPs worked were calculated only from March to April 2017. The ICPs attempted to directly communicate with the exposed contacts via phone call, text message, and e-mail. Attending or responsible physicians who were involved in index patients' care were also contacted by phone call or e-mail in cases when the exposed contacts could not be reached. Patient and visitor emotional responses to the contact investigation team were classified as follows: no-response, appreciative, accepting, and angry. We evaluated the time needed to review medical records, manage exposure files, and communicate with the contact persons, in addition to managing each ward and attending institutional SCET meetings for TB control.
Statistical analysis
A Spearman correlation analysis was used to analyze the association between the total number of close contacts and time to isolation or number of beds in a room. All statistical analyses were performed and figures were made using R software (version 3.1.2; R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was defined by a two-tailed P value of ≤ 0.05.
RESULTS
Identification of unexpected active pulmonary TB among hospitalized patients
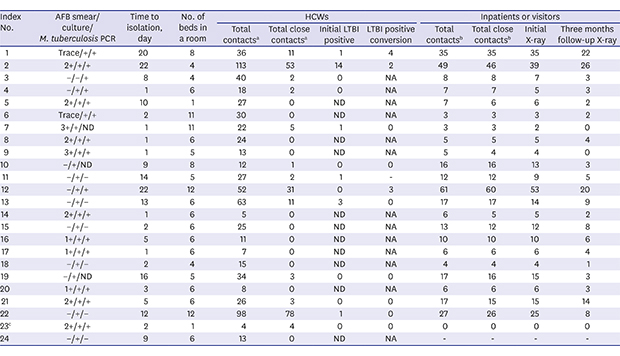
During the study period, 24 index patients were unexpectedly diagnosed with active pulmonary TB after admission to the hospital with non-tuberculous diseases. The median time from admission to TB diagnosis was 5 days (range, 1–22 days). Detailed clinical characteristics of the 24 index patients are shown in Supplementary Table 1. Of the 24 patients, 23 were diagnosed by a positive AFB stain or culture, while the remaining patient was diagnosed by a positive TB PCR result with clinical findings for active pulmonary TB (Table 1).
Table 1
Characteristics of index patients and effects of unexpected TB exposure on HCWs and inpatients or visitors
Data are number unless otherwise specified.
TB = tuberculosis, HCW = healthcare worker, AFB = acid-fast bacilli, PCR = polymerase chain reaction, LTBI = late tuberculosis infection, ND = note done, NA = not available.
aTotal number of contacts in HCWs were 723 and close contacts were 206; bTotal number of contacts in inpatients or visitors were 334 and close contacts were 322; cNo inpatient or visitor exposures were found in a single sterile room.
![]()
Initial contact investigation of close contact patients, visitors, and HCWs
There were 1,057 people who had contact with the 24 index cases. Of these 1,057 contacts, 528 (50%; 206 events in 157 HCWs and 322 inpatients or visitors) were defined as close contacts. There was a strong correlation between the time to isolation and total number of close contacts both in HCWs (r = 0.589; P = 0.002) and inpatients or visitors (r = 0.818; P < 0.001); however, there was no significant relationship between the number of beds in a room and total number of close contacts both in HCWs (r = 0.211; P = 0.32) and inpatients or visitors (r = 0.259; P = 0.23) (Supplementary Fig. 2). There was one immunocompromised close contact patient with chronic myeloid leukemia. We followed him for 9 months, but he is still not infected with TB. A total of 32 HCWs experienced repeated exposures (2 times for 15 HCWs and 3 times for 17 HCWs, respectively). Among these 32 HCWs, 25 experienced repeated exposure in the ICU, 5 in the emergency department, one nurse during a bronchoscopy, and one anesthesiologist in the operating room. Among the 157 close contact HCWs, 21 had a history of TB and 15 refused examination for latent TB. Of the 157 close contact HCWs, 23 (14.6%) had immediate LTBI (20 diagnosed with TST and 3 with IGRA).
Three-month follow-up investigation of close contact patients, visitors, and HCWs
Three months following exposure, 9 (9.2%) of the 98 TB-naïve close contact HCWs developed LTBI. Among them, 8 patients have completed LTBI treatment (Table 2). There was no documented active pulmonary TB among the 65 close contact patients or visitors who agreed to visit the hospital 3 months after exposure.
Table 2
Detailed results of LTBI conversion in HCWs after close exposure to active pulmonary TB

LTBI = latent tuberculosis infection, HCW = healthcare worker, TB = tuberculosis, TST = tuberculous skin test, IGRA = interferon gamma releasing assay.
![]()
Estimation of ICPs' work load for contact investigation
The ICPs' work load associated with the contact investigation was measured from March to April 2017. A total of 92 communication attempts (57 phone calls, 34 text messages, and 1 e-mail) were made to 60 close contact patients or visitors by 2 ICPs. The total amount of time to investigate 60 close contact patients or visitors was 472 minutes (median, 7 minutes per case). Among the 48 people who were reached by phone, the emotional response of the patients or visitors was no-response (n = 31), appreciation (n = 14), acceptance (n = 2), and anger (n = 1). The amount of time needed to investigate the exposed HCWs was 1,199 minutes (median 88 minutes per case) (Supplementary Tables 2 and 3).
DISCUSSION
Our aggressive contact investigation provided information on the extent of exposure in HCWs, as well as in inpatients and visitors, in an institution with mostly multi-bed rooms in an intermediate TB-burden country. Although there was no newly acquired active pulmonary TB among exposed patients, visitors, or HCWs 3 months following exposure, an aggressive contact investigation after the unexpected in-hospital diagnosis of active pulmonary TB showed a high incidence of newly acquired LTBI among TB-naïve HCWs who had contact with the index patients. Further, HCWs in the ICU and emergency department were prone to repeat TB exposure. In addition, we gathered information about compliance in close contact patients and visitors after exposure to active pulmonary TB. The considerable work load for ICPs might be the limitation for the proper maintenance of in-hospital TB control.
We found that the influence of unexpected TB exposure on HCWs in medical institutions is substantial. The annual incidence of LTBI among HCWs in the Korea was at least 3%, based on findings from both the TST and QFT-GIT,12 or ranging from 3.3% to 5.7%, based on serial QFT-GITs.13 In the present study, during the 9-months periods, approximately 10% (157/1,538) of HCWs were classified as close contact with active pulmonary TB. The conversion rate of LTBI in TB-naïve close contact HCWs, at 3 months following exposure, was 9.3%. Most HCWs were first tested for the LTBI when exposed to active pulmonary TB. Since May 2017, our hospital examined LTBI for all HCWs irrespective of TB exposure and began treatment for it. Because the risk of TB exposure is very high in the hospital environment, it is important to check and treat HCWs for LTBI at the time of hospital entry.
Unfortunately, there is no conclusive definition of close TB contact that can be applied to all circumstances. The National Health Service states that patients who spend more than 8 hours in the same hospital bay with a patient with a smear-positive TB and a cough have a risk of infection. If exposed patients are known to be particularly susceptible to infection, we must manage their TB risk as close contacts.6 The Tuberculosis Network European Trials Group defined a close non-household contact as a person with cumulative exposure time to a patient with a positive sputum smear index of 8 hours or 40 hours with a patient with a positive sputum culture index, adopting previous guiding principles.810 Exposure time may have a recall bias, which can be inaccurate. Therefore, it is important to consider the situation in which TB exposure has occurred. Our research has determined the range of close contacts, considering both cumulative exposure time and aerosol induced procedures.
We found that delayed TB diagnosis increases the extent of TB exposure significantly more than a multi-bed room hospital environment. In our previous study, we found that between 2003 and 2006, the time it took from hospital admission to TB diagnosis was 12 days. Between 2006 and 2008, we found that intervention by SCET reduced the time to TB diagnosis by 5.6 days.5 We have continued this same intervention since 2008. In this study, the diagnosis time was 5 days; however, 5 days of health system delay is relatively short compared to the 28.5 days reported by previous studies.14 Moreover, early diagnosis and prompt treatment of TB is significantly associated with good prognosis.15 Among our 24 patients with active pulmonary TB, 13 had a positive AFB stain. Even with this positive stain, 3 patients were not isolated for 10 days. We then began notifying the medical staff to a positive AFB smear immediately, as well as a positive AFB culture by a laboratory technician. Further analysis of the index cases to identify factors associated with delayed isolation of active pulmonary TB is needed.
Our study had some limitations. Following hospital policy, we performed both TST and IGRA tests on exposed HCWs for the detection of latent TB. However, there was a discrepancy in the results from these tests, making them difficult to interpret. Though we can use both TSTs and IGRAs for the detection of latent TB, we believe that the IGRA test should be used because it will reduce the multiple visits needed for the TST and is more likely to reflect the transmission of TB in HCWs.16 We do not have results from the baseline two-step TST; thus, it is difficult to know whether the positive result from the secondary TST is boosted by the two-step TST or is newly triggered after exposure. However, the two-step TST is not mandatory at the time of TB exposure investigation for the purpose of detection and treatment of latent TB.17 Lastly, we restricted the LTBI test subjects to only close contact HCWs and immunocompromised patients with limited follow-up visits among close contact patients or visitors in approximately 20% (65/322), despite active contact by ICPs. To our knowledge, our strategy was the most aggressive investigation in Korea with intermediate TB burden. However, further studies are needed in this field to better understand the whole picture of TB transmission in hospital settings.
In conclusion, the incidence rate of LTBI was 9.2% among 98 TB-naïve close contact HCWs after three months post-exposure. To effectively prevent the transmission of active pulmonary TB, a well-organized system for prompt diagnosis, patient isolation, and treatment of active pulmonary TB, in addition to enough well trained ICPs for massive contact management and investigation, are needed.
 XML Download
XML Download