

 PDF
PDF Citation
Citation Print
Print



The varicella-zoster virus is highly contagious, and secondary attack rates of varicella are 60%–90% for susceptible household contacts.1 Varicella is one of the most common infectious diseases in preschool-aged children and can be caused by contact at day-care centers, kindergartens, and schools. Varicella vaccination has been introduced in many countries, which has led to a marked decrease in its incidence.2 It was introduced in the National Immunization Program (NIP) of Korea from 2005. A one-dose varicella vaccine has been recommended for all children aged 12–15 months. Since 2010, the rate of varicella vaccination has reached more than 97% nationwide.3 However, despite the high vaccination rate, the national notifiable diseases surveillance system reported that the incidence of varicella has been continuously rising, from 11,027 cases in 2006 to 80,091 cases in 2017. As a result, several papers have raised awareness of the occurrence of varicella in Korea. Lee et al.4 reported that the varicella vaccine used in Korea was not effective in preventing varicella infection. Kim et al.5 suggested that careful attention needs to be paid to the occurrence of infectious diseases in Korea due to increased reporting of varicella, mumps, and scarlet fever.
The purpose of our study was to evaluate whether the increase in number of varicella cases reported to the National Infectious Disease Surveillance (NIDS) system reflects a true increase in the number of varicella cases by using national health insurance claims data. In addition, we used a series of birth cohorts to assess the effectiveness of varicella vaccination before and after its introduction in the NIP.
We evaluated the incidence of varicella using surveillance data from the NIDS and compared it to claims data from the National Health Insurance Service (NHIS), which is considered the gold standard for certifying the number of hospital visits of patients with varicella. The NIDS is a passive surveillance system, managed by the Korea Center for Disease Control and Prevention, which monitors the incidence of national notifiable infectious diseases of which notification by physicians is mandated legally.6 Varicella was added to the list of notifiable diseases in 2005, the same year when its vaccination was introduced to the NIP. Korea has a single payer, universal coverage national health insurance scheme managed by the NHIS. The NHIS claims data contains information on the whole population of Korea, which includes information regarding medical utilization, diagnoses of patients based on the International Classification of Disease, 10th revision (ICD-10), prescription records, and patient characteristics.7 Claimed varicella cases were identified based on the time of the first diagnosis for each individual. The monthly number of claimed cases with a diagnosis of varicella (ICD-10: B01) was evaluated by age. We compared the varicella surveillance reports and claims data on a monthly basis. For evaluating the reporting rate, we calculated the ratio of these two indices; NIDS reports per NHIS claims.
To evaluate the effect of varicella vaccination in different birth cohorts, we calculated the incidence and cumulative incidence rate of varicella in each birth cohort according to age. The total number of births per year between 2002 and 2012 was obtained from the birth statistics maintained by the Korea National Statistical Office. The incidence rate was calculated as the number of varicella claims according to age divided by the number of births in each birth cohort. Because life-long protective immunity develops after varicella infection, the cumulative incidence rate was calculated by dividing the cumulative number of varicella claims (the total varicella claims from previous ages) by the number of births in each birth cohort.
Because this study used secondary data obtained from the NHIS and NIDS and contained no personal information, informed consent was waived, and the study protocol was approved by the Institutional Review Board (IRB) of Korea University (IRB No. KU-IRB-18-EX-51-A-1).
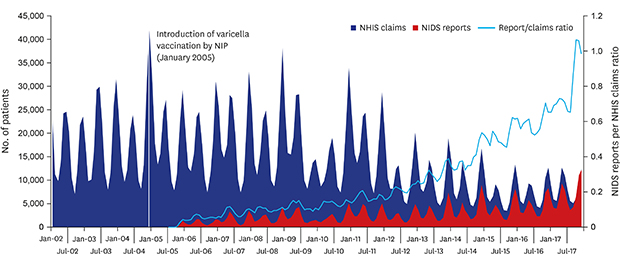
The incidence of varicella in Korea showed a bimodal pattern, reflecting seasonal variations, as observed with both the NHIS claims data and NIDS data (Fig. 1). Reports of varicella in the NIDS system have steadily increased, but NHIS claims for medical utilization of varicella treatment gradually decreased since 2012. The ratio between NHIS claims and NIDS reports was greater than 80% since the second half of 2017.
The incidence of varicella infection at each age was evaluated according to the birth year (Fig. 2). The incidence rate in children aged 4–6 years, the age at which varicella infection is most common, decreased to about one third in the birth cohort born after 2009 compared to those born before 2005. Approximately, 27% of all babies born before 2005 were diagnosed with varicella at least once before 6 years of age. However, the cumulative incidence rate of varicella infection among children born after 2009 was approximately 11%.
The yearly patterns of varicella incidence were similar between the NHIS claims data and NIDS data, showing seasonal variation. However, the trends of varicella reports in NIDS and claims in NHIS differed over time. Although varicella reports in NIDS have steadily increased, claims for medical use of varicella treatment in NHIS has gradually reduced since 2012. Since clinicians are required to report both suspected and confirmed varicella cases to the NIDS, all claims related to varicella cases should be reported to NIDS. The ratio between NHIS claims and NIDS reports indirectly reflects this reporting rate, as has been reported by Tan et al.8 for varicella. Therefore, the increase in NIDS varicella reports is likely due to an improvement in the reporting rate, rather than an actual increase in varicella incidence. Kim et al.9 also reported that the incidence of scarlet fever in Korea increased with improved reporting rates.
The cumulative incidence rate of varicella among children below 6 years in the birth cohort born after the NIP introduced the varicella vaccine was approximately 60% lower than among children born before introduction of the varicella vaccine. This reduction might be due to the effect of vaccination.
The delayed reduction in incidence after the introduction of varicella vaccination was due to both the length of time from vaccination age to school age and the varicella vaccination rate. Since a majority of varicella cases occur at 4–6 years of age, it takes at least 4–5 years to reduce the occurrence of varicella after vaccination. Moreover, the vaccination rate rose gradually until 2009. There has not been a nationwide survey of varicella vaccination rates before 2009; however, in a single region, the vaccination rates for varicella in 2007, 2008, and 2009 were 78.3%, 89.3%, and 99.0%, respectively.10 In the United States, it took 4 years to reduce the incidence of varicella by half after varicella vaccination was recommended.2 However, considering that the current reduction in varicella infection rate was insufficient for varicella outbreak control, and that there was no difference in the incidence rate between pre-vaccination and post-vaccination birth cohorts after 8 years of age, a discussion to introduce a boosting vaccination of varicella is needed.11
Our study had several limitations. We did not evaluate the association between individual vaccination history and the occurrence of varicella, so we could not directly estimate the effectiveness of vaccination. In addition, it was not possible to determine whether the varicella cases were due to breakthrough infection after varicella vaccination. Since the incidence rate was defined as the number of varicella cases relative to the number of births in each birth cohort, it could reflect changes in population by age due to death or emigration. However, Korea has not been affected by any sudden population changes in recent years. Furthermore, the national health insurance data used in this study are basically designed for billing and there may have been various changes over time. However, the diagnostic criteria and claim behavior of healthcare providers did not appear to have changed considerably.
In conclusion, the increase in the reported incidence of varicella in Korea was inconsistent with insurance claims data, which suggests an improvement in reporting rather than a true increase in incidence. The varicella incidence in post-vaccination birth cohorts was lower than that in pre-vaccination birth cohorts. Further studies are needed to assess the effectiveness of varicella vaccination.

 XML Download
XML Download