

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Postoperative pain can have a considerable influence on quality of life [1], and develops following endodontic treatment in between 3% and 58% of cases [2]. According to a study by Çiçek et al. [3] the pain prevalence in the first 24 hours was 40%, and decreased to 11% after 7 days. Successful management of postoperative pain is an important issue for the clinician. Although postoperative pain is multifactorial, the instrumentation technique is thought to play a major role [34]. Depending on the technique used, infected debris and bacterial extrusion may be transported to periapical tissues during chemomechanical preparation and induce an acute inflammatory response [56]. Although all instrumentation techniques are associated with extrusion of debris, the quantity of extruded debris can vary, depending on the technique used and the file design [7].
The use of a glide path facilitates cleaning and shaping processes with nickel titanium (NiTi) instrumentation [8910]. Preliminary canal enlargement may substantially decrease the occurrence of transportation and ledge formation, the frequency of strip perforation, and the incidence of NiTi instrument fracture [11]. It also contributes to a reduction in apical extrusion during root canal preparation, while preserving the original root canal morphology. Glide path preparation can be carried out manually or using engine-driven systems. Previous research showed that when a glide path was formed using NiTi rotary instruments, the preservation of the original canal anatomy was better than when the glide path was formed using stainless-steel manual instruments [12].
One G (OG; Micro-Mega, Besancon, France) which is produced from a conventional NiTi alloy, uses continuous rotation and results in improved glide path creation. It has a 0.14 mm tip diameter and constant 3% taper, asymmetric cross-section, and 3 cutting edges. According to the manufacturer, the cutting edges have diverse radii, resulting in improved debris elimination. The OG has a varying pitch among its cutting blades, with the aim of reducing its screwing efficacy [10]. R-Pilot [RP] files (VDW, Munich, Germany), which are made of M-wire alloy, are designed for glide path preparation. The RP is the first engine-driven glide path instrument to be used in a reciprocating movement. It has a 12.5 tip diameter, constant 4% taper and an S-shaped cross-section [13].
To the best of our knowledge, no studies have compared postoperative pain intensity after using reciprocating versus continuous rotary glide path systems. Therefore, the objective of this randomized clinical trial was to compare postoperative pain intensity using 2 glide path systems (OG and RP) and no glide path system (without a glide path [WGP]). Analgesic (tablet form) intake by the patients was also evaluated. The null hypothesis tested was that there would be no difference in postoperative pain intensity or analgesic consumption.
MATERIALS AND METHODS
This single-center, randomized controlled clinical trial was carried out between January 2018 and April 2018 at the Department of Endodontics, Hatay Mustafa Kemal University. This in vivo study was conducted after obtaining approval from the Ethics Committee of Mustafa Kemal University (IRB No. 2018/07). All the patients were informed about the indications for endodontic treatment, the benefits and risks associated with treatment procedures.
Participants
This randomized controlled clinical trial included the first or second mandibular premolars of 93 patients aged between 20 and 65 years (Figure 1). Healthy study subjects were recruited from a pool of patients referred to the Mustafa Kemal University, Department of Endodontics from January 2018 to April 2018. Demographic data on the subjects were recorded after intraoral examinations. The subjects had first or second single-canaled mandibular premolars with a diagnosis of asymptomatic non-vital pulp. The mandibular premolars were radiographed preoperatively to verify the presence of a single root and single canal. In each subject, the pulpal diagnosis was performed using a heat test, cold test, palpation, and percussion. The heat test was performed using a pre-heated gutta-percha cone placed on the middle third of the buccal surface of the teeth, and the cold test was performed with the aid of a cold spray (Endo-Frost; Coltène-Whaledent, Langenau, Germany) placed on a cotton pellet on the middle third of the buccal surface of the tooth. If no response was seen after 10 seconds, the test result was considered negative. The diagnosis was also supported by the absence of bleeding in the root canals after the access cavity was made. Only 1 tooth per subject was included in the study.

The exclusion criteria were systemic diseases, allergic reactions, sinus tract, a periapical abscess or resorption in a relevant tooth, a severely damaged tooth, consumption of analgesics within the past 24 hours, or an inability to understand the study instructions.
Randomization
To ensure random selection, prior to the initiation of the study, all the patients' names were written on pieces of paper. These were then folded, mixed, and placed in a sealed box. A clinical assistant then blindly removed the pieces of paper from the box until all the patients had been assigned to 3 groups according to the glide path system to be used.
Treatment protocol
One specialist performed all the treatments in a single visit. All the teeth were anesthetized using a local anesthetic solution containing 4% articaine with 1:100,000 epinephrine (Ultracain DS Forte; Sanofi-Aventis, Bridgewater, NJ, USA) by inferior alveolar nerve block. After anesthesia, the relevant tooth was isolated with a rubber dam, and a standard access cavity was prepared using diamond burs.
WGP group
The root canals were explored with sizes 10 or 15 K-file hand files. The working length (WL) was determined by inserting a size 15 K-file up to the apical foramen and using a Root ZX apex locator (J. Morita Co., Tustin, CA, USA). The WL was supported radiographically, and it was repeatedly checked during the treatment procedure. The root canals were prepared using Mtwo rotary files (VDW) to size 30/0.05 according to the manufacturer's instructions, using a torque-limited handpiece powered by an electric motor (Silver Reciproc; VDW). Using a gentle in-and-out motion, the Mtwo systems were operated using sizes 15/0.05, 20/0.06, 25/0.06, and 30/0.05 instruments/taper, respectively. The canals were irrigated with 5 mL of 2.5% NaOCl and 5 mL of 17% ethylenediaminetetraacetic acid (EDTA) solution after each instrument change. Lastly, the canals were irrigated, rinsed with distilled water, and dried with paper points. The canals were filled with gutta-percha and AH Plus sealer (Dentsply, Konstanz, Germany) using the lateral condensation technique. Following radiographic confirmation of the obturation, the coronal seal was maintained with a resin-modified glass ionomer and then a nanohybrid composite resin.
OG group
The WL was determined using the same apex locator as in the WGP group. The OG (size 14/0.03) instrument was operated with the electric motor (Silver Reciproc) in continuous rotation at 300 rpm and 1.2 Ncm of torque, according to the manufacturer's instructions. Each file was used only once (single use). The root canal was irrigated with 5 mL of 2.5% NaOCl and 5 mL of 17% EDTA after instrument use. The Mtwo rotary file preparation and obturation procedures were performed as in the WGP group.
RP group
The WL was determined using the same apex locator as in the previous groups. The RP (size 12.5/0.04) instrument was used for glide path creation using a reciprocating motion. The RP instrument was used with the same endodontic motor in the ‘Reciproc all’ mode. The instrument was moved using a slow in-and-out pecking motion, not exceeding an amplitude of 2–3 mm, with light apical pressure. After 3 motions, the file was cleaned, and the root canal was irrigated with 5 mL of 2.5% NaOCl and 5 mL of 17% EDTA. The procedures were repeated until the exact WL was reached. After creating the glide path, the same Mtwo shaping and filling procedures as executed in the WGP and RP groups were carried out.
Pain assessment
Postoperative pain intensity was evaluated using a visual analogue scale (VAS), ranging from 0 to 10. All the patients recorded the incidence of pain at 24, 48, and 72 hours post-treatment on the VAS. For intolerable pain after the procedure, ibuprofen (400 mg) was prescribed. The subjects were instructed to record post-treatment pain on the VAS, as well as analgesic intake. On the VAS, pain intensity was categorized as no pain (0), mild pain (1–3), moderate pain (4–6), and severe pain (7–10) [14]. All the subjects completed the pain VAS. On the first, second, and third day after the procedure, a clinical assistant from the Department of Endodontics contacted the patients by telephone and questioned them about their pain scores based on the VAS and their analgesic intake at 24, 48, and 72 hours post-treatment.
Statistical analysis
The data were analyzed using SPSS version 20.0 (IBM Corp., Armonk, NY, USA). The normality of the distribution of the variables was tested using the Shapiro-Wilk test. The Friedman, Kruskal-Wallis, and Mann-Whitney U tests were conducted to compare the influence of glide path systems on postoperative pain, and the χ2 test was applied to compare demographic data and analgesic intake across the 3 groups.
RESULTS
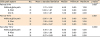
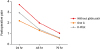
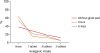
In total, 93 patients were enrolled in this study. No patient was lost to follow-up in any group (Figure 1). The demographic data, analgesic intake, and postoperative pain levels of the study groups are presented in Tables 1, 2, 3. There were no between-group differences in demographic data (age, sex, and type of teeth) (p > 0.05). Postoperative pain decreased significantly at each time interval in all groups (p < 0.05) (Figure 2). The most severe postoperative pain was recorded at 24 hours after the root canal treatment. At 24 hours, the OG group had less postoperative pain than the WGP group (p < 0.05). However, no significant difference was found between the RP group and the others. There were no statistically significant differences in postoperative pain scores at 48 or 72 hours, or in analgesic intake at the 3 assessed time intervals among the 3 groups (p > 0.05) (Figure 3).
Table 1
Demographic data of each group

![]()
Table 2
Mean VAS scores of postoperative pain at different time intervals for each group
![]()
Table 3
Frequency and percentage of analgesic intake according to group

![]()
DISCUSSION
Postoperative pain management is very important in endodontic practice. Many variables influence the sense of postoperative pain, including patient-specific factors and the characteristics or status of the teeth. Differences in the factors that affect postoperative pain make it challenging for clinical studies to relate pain incidence to its probable causes. Thus, several strategies have been used to evaluate postoperative pain. These include patient communication, explaining the procedure with the aim of reassuring the patient; the use of nonsteroidal anti-inflammatory drugs [15] and occlusal reductions [16]; the application of several techniques and instrumentation kinematics [17]; the creation of a glide path [18].
The incidence of canal aberrations and fractured instruments can be reduced by creating a glide path. Glide path formation may be an important factor in postoperative pain. In a previous study, Pasqualini et al. [18] showed that the creation of a glide path with a NiTi rotary instrument led to less postoperative pain than hand instrumentation. Glide path systems with different kinematics may also be an important factor in the occurrence of postoperative pain.
The creation of a glide path reduces possible operational failures during root canal treatment. The OG and RP are engine-driven glide path instrument systems consisting of a single file that use different kinematics (continuous motion vs. reciprocating motion). These systems were introduced to simplify and accelerate glide path preparation as compared to hand files [19]. There is no information in the literature on postoperative pain intensity after using reciprocating and continuous rotary glide path systems. The OG and RP glide path instruments were used in the present study due to this difference in their kinematics.
In this study, only asymptomatic teeth with non-vital pulp were selected and no preoperative pain was present in any of the patients. Teeth with periapical lesions were excluded to eliminate other factors that could cause postoperative pain. Single-visit treatments were carried out to reduce the number of variables and to prevent potential problems that may occur between 2 visits. Randomization ensured that demographic variables and tooth-related factors were similarly allocated among the glide path groups in this study. The VAS was chosen because of its documented validity and reliability in postoperative pain measurement [220].
Ibuprofen is one of the most frequently used analgesics after root canal treatment [1]. In many studies, ibuprofen has been used as the first choice of analgesic [121]. Ibuprofen was selected in the present study to reduce postoperative pain. No statistically significant differences were found among the WGP, OG, and RP groups in analgesic intake at the 3 assessed times (p > 0.05).
The present study compared postoperative pain intensity using the OG and RP glide path systems. There was no statistically significant difference in postoperative pain intensity among the 3 groups (WGP, OG, and RP) at 48 or 72 hours (p > 0.05). However, the OG group had less postoperative pain at 24 hours than the WGP group (p < 0.05). Postoperative pain decreased significantly at each time point (24, 48, and 72 hours) (p < 0.05). Thus, the null hypothesis was rejected. Previous studies have also demonstrated that the prevalence and intensity of postoperative pain significantly decreased after root canal treatment, in accordance with the passage of time. In a systematic review, Pak et al. [22] found that postoperative pain prevalence decreased significantly during the first 48 hours after root canal treatment and dropped to 10% or less after the first week. The findings of their study are in accordance with those of the present study.
In the current study, the OG and RP systems were similar regarding postoperative pain intensity. As no published studies have investigated the impact of these glide path systems on postoperative pain, a comparison with prior studies is not possible. However, several studies have investigated the effects of postoperative pain associated with instruments that used different motions [17]. These studies have reported contradictory results, with some concluding that instruments that used a reciprocating or rotary motion had no effect on postoperative pain [15], but others coming to the opposite conclusion [2023]. At present, there is no clear consensus on this issue. Postoperative pain is generally associated with instrumentation kinematics, over-instrumentation, extruded debris, or filling materials [1].
All instrumentation processes generate some debris extrusion, but the amount of extruded material can vary, depending on the motion, cross-sectional design, and taper of the instrument system. Bürklein et al. [24] indicated that systems that used rotary instrumentation were associated with less debris extrusion than one that employed reciprocating motion, and proposed that this may have been associated with less postoperative pain. Similarly, Lu et al. [25] concluded that Reciproc (VDW) instruments led to a significantly greater quantity of extruded debris during retreatment than the Mtwo R (VDW) instrument system. In contrast, Üstün et al. [26] compared the amount of debris extrusion of the ProTaper Next (Dentsply Sirona, Ballaigues, Switzerland), Twisted file (SybronEndo, Orange, CA, USA), and WaveOne (Dentsply Sirona) systems and demonstrated that the WaveOne system extruded less debris than was extruded by the other 2 systems. Dincer et al. [6] reported that the Reciproc system resulted in less apical extrusion than the ProTaper (Dentsply Sirona) and Mtwo systems. There are differences of opinion on the impact of the reciprocating and continuous systems on apical extrusion. Although there was no statistically significant difference in the present study, postoperative pain was somewhat lower in the OG group than in the RP group. This finding may be explained by differences in the kinematics of these 2 systems.
The size and cross-sectional design of the glide path instruments used also need to be considered, and such differences may have affected the results of the present study. The present study tested an OG glide path file (size 14/0.03) and RP glide path file (size 12.5/0.04). The OG system has an asymmetric cross-section, whereas the RP system has an S-shaped cross-section.
 XML Download
XML Download