

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Case summary
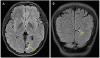
A 23-year-female was referred to our clinic because of a visual field defect incidentally discovered during preoperative evaluation for refractive surgery at another clinic. However, she did not report any symptoms. She had no systemic diseases. Visual acuity was 20/20 in both eyes, and the color vision test was normal. Both pupils exhibited normal responses to light and near stimulations. In fundus examinations, the right optic disc was normal and the left contained drusen. Automated perimetry revealed right lower homonymous quadrantanopia with macular sparing. Brain magnetic resonance imaging revealed areas of ulegyria involving the left occipital lobe, consistent with the visual field defect. A follow-up visual field test performed 5 months later yielded the same result.
Figures and Tables
Figure 1
Images of the fundus photograph at the initial visit. The right eye showed normal appearance of optic disc (A). The left eye showed optic disc drusen (B).


References
1. Miller NR, Subramanian PS, Patel VR. Walsh and Hoyt's clinical neuro-ophthalmology: the essentials. 3rd ed. Philadelphia: Lippincott Williams & Wilkins;2016. p. 209–241.
2. Fraser JA, Newman NJ, Biousse V. Disorders of the optic tract, radiation, and occipital lobe. Handb Clin Neurol. 2011; 102:205–221.


3. Ogawa K, Ishikawa H, Suzuki Y, et al. Clinical study of the visual field defects caused by occipital lobe lesions. Cerebrovasc Dis. 2014; 37:102–108.
4. Lee HJ, Maeng YH, Jeong J, et al. Occipital lobe metastasis of hepatocellular carcinoma presenting as homonymous hemianopia. J Korean Ophthalmol Soc. 2017; 58:488–492.
5. Liu G, Volpe N, Galetta S. Liu, Volpe, and Galetta's neuro-ophthalmology. 3rd ed. Philadelphia: Elsevier;2019. p. 293–339.
6. Pane A, Miller N, Burdon M. The neuro-ophthalmology survival guide. 2nd ed. Beijing: Elsevier;2017. p. 92–98.
7. Gil-Nagel A, García Morales I, Jiménez Huete A, et al. Occipital lobe epilepsy secondary to ulegyria. J Neurol. 2005; 252:1178–1185.
8. Kim HW, Cho KY, Lee MC, et al. A study of ulegyria as pathognomonic aspects of congenital bilateral perisylvian syndrome. J Korean Neurosurg Soc. 2005; 37:124–128.
9. Nikas I, Dermentzoglou V, Theofanopoulou M, Theodoropoulos V. Parasagittal lesions and ulegyria in hypoxic-ischemic encephalopathy: neuroimaging findings and review of the pathogenesis. J Child Neurol. 2008; 23:51–58.
 XML Download
XML Download