

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) has been a curative modality for various non-malignant diseases, including bone marrow failure syndromes (BMFS), primary immunodeficiency diseases, hemophagocytic lymphohistiocytosis, inherited metabolic disorders, and many other hematologic disorders.1234 Analysis of the chimerism status has become an important diagnostic tool for post-transplant investigation of engraftment and prediction of disease recurrence. Previous reports showed that a malignant disease with increasing mixed chimerism (MC) after allo-HSCT had the highest risk of relapse, and an early intervention could improve the transplant outcomes.56 In contrast to malignant diseases, stable MC even with a high degree of residual recipient hematopoiesis, allows for the correction of the underlying non-malignant diseases.78 However, because MC may progress to graft rejection, early detection of the chimerism status after allo-HSCT might be important to prevent graft loss in non-malignant diseases. Moreover, early analysis of the chimerism status could provide information for subsequent interventions, such as rapid withdrawal of immunosuppression, donor lymphocyte infusion, or stem cell boost.9
The initial time point of chimerism analysis has differed among previous studies.1011121314 Conventionally, the first analysis of chimerism status has been performed approximately 1 month after allo-HSCT because the remaining recipient cells are frequently detected in the samples obtained too early after transplantation.1112141516 However, to the best of our knowledge, studies comparing transplant outcomes according to day 14 chimerism status after allo-HSCT in patients with non-malignant disease have not yet been reported. Therefore, the main aim of this study was to determine the impact of day 14 peripheral blood chimerism status on the transplant outcomes in patients who underwent allo-HSCT for non-malignant diseases.
METHODS
Patients
We retrospectively reviewed the medical records of 56 patients with non-malignant disease who received allo-HSCT at the Samsung Medical Center between April 2007 and March 2016. Non-malignant diseases included severe aplastic anemia, pure red cell aplasia, congenital dyserythropoietic anemia, severe congenital neutropenia, hemophagocytic lymphohistiocytosis, and primary immunodeficiency disease. The patients with X-linked severe combined immunodeficiency were excluded because they received allo-HSCT without conditioning.
Chimerism analyses
Chimerism analyses were performed using short-tandem repeat (STR) polymerase chain reaction (PCR). STR markers were evaluated in a given patient-donor pair using the fluorescence PCR technique. PCR was performed on the GeneAmp PCR system 9700 (Applied Biosystems, Foster City, CA, USA), and amplicon sizes were resolved by electrophoresis. One or two informative STR markers were selected for follow-up in a given patient-donor pair. Quantification of recipient DNA was performed by calculating areas under the peaks using GeneMapper software (Applied Biosystems) as previously described.17 We regarded it as complete donor chimerism (CC) if ≥ 99% of the cells were of donor origin. MC was defined if > 1% of the cells were recipient-derived in the presence of donor-origin hematopoiesis which was further categorized into low-level MC (> 1% and < 15% of recipient-derived cells) and high-level MC (≥ 15% of the recipient-derived cells). Chimerism status was evaluated at day 14 after allo-HSCT in peripheral blood and at 1 month in BM aspirates. Thereafter, chimerism status was evaluated at 3 months, 6 months, and 1 year post-transplant in BM aspirates.
Conditioning regimens and graft-versus-host disease (GVHD) prophylaxis
Patients received allo-HSCT with various myeloablative conditioning (MAC) or reduced-intensity conditioning (RIC) regimens depending on their disease or pre-transplant performance status. Prophylaxis against GVHD was based on cyclosporine (3 mg/kg per day) or tacrolimus (0.03 mg/kg per day) with or without short-term methotrexate, and mycophenolate mofetil replaced methotrexate for cord blood (CB) transplants. Initial drug levels were adjusted to maintain cyclosporine concentration within 200–300 ng/mL, and tacrolimus within 15–20 ng/mL.
Statistics
The probabilities of overall survival (OS) and event-free survival (EFS) rates were estimated by the Kaplan-Meier method, and comparisons between survival curves were performed using the log-rank test. OS was defined as the time from transplantation to death from any cause. Event was defined as death, primary engraftment failure, late rejection, or progression of primary disease, whichever occurred first. Primary engraftment failure was defined as failure to achieve a neutrophil count greater than 0.5 × 109/L after transplantation. Patient characteristics and clinical outcomes were compared using linear by linear association or Fisher's exact test for binary variables and Kruskal-Wallis test or Mann-Whitney U test for continuous variables. Pearson correlation analysis was used to observe the relationships between two continuous variables. Statistical differences were considered significant if P < 0.05.
RESULTS
Patients
Fifty-six patients with non-malignant disease underwent allo-HSCT with a median follow-up of 49 (range, 12–107) months, and the 5-year OS and EFS rates were 79.4% ± 5.6% and 75.8% ± 5.9%, respectively. Severe aplastic anemia (n = 25) was the most common disease followed by chronic granulomatous disease (n = 10), hemophagocytic lymphohistiocytosis (n = 6), Wiskott-Aldrich syndrome (n = 4), Fanconi anemia (n = 3), other BM failures (n = 5), and other primary immunodeficiency diseases (n = 3).
Chimerism
Because all 56 patients showed > 1% donor-derived hematopoiesis according to their day 14 peripheral blood chimerism analyses, they were able to be allocated into one of the 3 groups at day 14 post-transplant: CC (n = 36; 64.3%), low-level MC (n = 14; 25.0%), or high-level MC (n = 6; 10.7%). Of 36 patients with day 14 CC, 6 patients had MC at 1 month (donor range, 84.5%–98.8%), among whom 5 patients achieved CC again at 3 months and beyond until 1 year, while the remaining 1 patient who showed low-level MC (95.5% donor cells) at 1 month died due to septicemia at 3 months. Of 30 patients who showed CC at both day 14 and 1 month, 25 maintained CC until 1 year, 1 maintained CC until 6 months but then showed low-level MC (donor 98.8%) at 1 year. The remaining 4 patients died before the next evaluation of chimeric status.
Of the 14 patients with day 14 low-level MC (donor range, 85.6%–98.9%), 1 maintained stable MC (donor 97.9%) at 1 year, and 12 patients showed CC by 1 year; 5 achieved CC at 1 month, 4 at 4 months, 1 at 6 months, and 2 at 1 year. One patient with day 14 low-level MC (92.6% donor cells) who achieved CC at 3 months died due to systemic fungal infection at 4 months.
Of the 6 patients with day 14 high-level MC (donor range, 23.7%–82.7%), 3 patients (donor 23.7%, 31.6%, and 68.3%, respectively) failed primary engraftment, 1 patient achieved CC at 1 month but died due to cytomegalovirus pneumonia at 2 months, and 2 patients remained stable MC (donor 96.3% and 97.7%, respectively) at 1 year post-transplant. The chimeric status of patients with day 14 high-level MC is shown in Fig. 1.

Transplant characteristics and outcomes
Table 1 shows the differences in the transplant characteristics among the day 14 CC, low-level MC, and high-level MC groups. There were no statistical differences among the 3 groups in diseases, donors, and stem cell sources, but RIC regimens were more frequent in the day 14 CC or low-level MC group than in the day 14 high-level MC group (CC vs. high-level MC, 61.1% vs. 0%, P = 0.007; low-level MC vs. high-level MC, 50.0% vs. 0%, P = 0.049). There was a positive correlation between the degree of day 14 donor chimerism and the number of infused CD34+ cells (r = 0.302, P = 0.027) (Fig. 2). Table 2 shows the post-transplant outcomes according to the day 14 peripheral blood chimerism status. Neutrophil engraftment was faster in the day 14 CC group compared with that of the day 14 high-level MC group (12 vs. 16 days, P = 0.006). Notably, 3 patients in the day 14 high-level MC group but none in the day 14 CC or low-level MC group developed primary engraftment failure (P < 0.001). There was no difference in the incidence of grade II–IV acute GVHD (P = 0.486) or chronic GVHD (P = 0.683) among the 3 groups.
Table 1
Demographic and transplant characteristics according to day 14 chimerism status

Data are presented as median (range) or number (%).
CC = complete donor chimerism, MC = mixed chimerism, BM = bone marrow, PBSC = peripheral blood stem cell, CB = cord blood, GVHD = graft-versus-host disease, CsA = cyclosporine, TNC = total neutrophil count.
aThe conventional conditioning regimens for severe aplastic anemia were regarded as reduced-intensity conditioning.
![]()
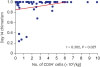 | Fig. 2Pearson correlation analysis between day 14 chimerism level and the number of infused CD34+ cells.
|
Table 2
Post-transplant outcomes according to day 14 chimerism status
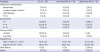
Data are presented as number (%).
CC = complete donor chimerism, MC = mixed chimerism, CMV = cytomegalovirus, PTLD = post-transplant lymphoproliferative disease, GVHD = graft-versus-host disease, ANC = absolute neutrophil count, PLT = platelet.
![]()
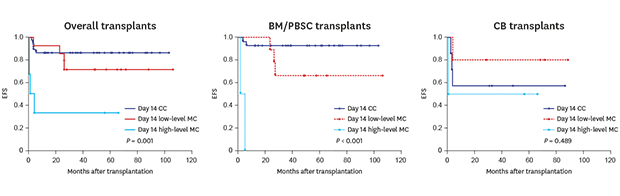
In the day 14 CC group, five deaths occurred caused by septic shock (n = 2), fungal pneumonia (n = 1), cytomegalovirus pneumonia (n = 1), and veno-occlusive disease (n = 1). In the day 14 low-level MC group, four deaths occurred caused by septic shock (n = 2) and chronic GVHD (n = 2). In the day 14 high-level MC group, 3 patients failed primary engraftment and one died of septic shock. Of the 3 patients with primary engraftment failure in the high-level MC group, 2 patients received second allo-HSCT and the remaining one patient died of septic shock. Although the 5-year OS was comparable among the day 14 CC, and low-level MC, and high-level MC groups (86.1% vs. 71.4% vs. 66.7%, P = 0.371) (Fig. 3A), the 5-year EFS was significantly higher in the day 14 CC or low-level MC group than in the day 14 high-level MC group (86.1% vs. 71.4% vs. 33.3%, P = 0.001) (Fig. 3B).
 | Fig. 3OS and EFS rates according to day 14 chimerism status. All P values were determined by the log-rank test. (A) The 5-year OS were similar among the day 14 CC and low- and high-level MC groups (86.1% vs. 71.4% vs. 66.7%, P = 0.371). (B) The 5-year EFS was higher in patients with CC or low-level MC than those with high-level MC (86.1% vs. 71.4% vs. 33.3%, P = 0.001).OS = overall survival, EFS = event-free survival, CC= complete donor chimerism, MC = mixed chimerism.
|
Outcomes according to graft source
The primary engraftment failure rates according to the graft source showed 0% (0/5) with BM, 2.9% (1/35) with peripheral blood stem cells (PBSC), and 12.5% (2/16) with CB. The median times to neutrophil and platelet engraftment were faster in BM/PBSC transplants than in CB transplants (neutrophils: 12 vs. 17 days, P < 0.001; platelets: 17 vs. 42 days, P = 0.001, respectively). The 5-year OS and EFS rates were not statistically different between donor graft sources (OS: BM/PBSC 83.1% vs. CB 68.8%, P = 0.160; EFS: BM/PBSC 80.6% vs. CB 68.8%, P = 0.082, respectively). In transplants with a BM/PBSC graft, although the 5-year OS was comparable among the day 14 CC, low-level MC, and high-level MC groups (93.1% vs. 66.7% vs. 50.0%, P = 0.060) (Fig. 4A), the 5-year EFS was significantly higher in the day 14 CC or low-level MC group than in the day 14 high-level MC group (93.1% vs. 66.7% vs. 0%, P < 0.001) (Fig. 4B). However, in CB transplants, the 5-year OS and EFS rates according to the day 14 peripheral blood chimerism did not reach statistical significance (OS: 57.1% vs. 80.0% vs. 75.0%, P = 0.662; EFS: 57.1% vs. 80.0% vs. 50.0%, P = 0.489).
 | Fig. 4OS and EFS rates according to day 14 chimerism status in transplants with BM/PBSC. (A) The 5-year OS were comparable among the day 14 CC and low- and high-level MC groups (93.1% vs. 66.7% vs. 50.0%, P = 0.060). (B) The 5-year EFS was higher in patients with CC or low-level MC groups than those with high-level MC (93.1% vs. 66.7% vs. 0%, P < 0.001).OS = overall survival, EFS = event-free survival, BM/PBSC = bone marrow or peripheral blood stem cell, CC = complete donor chimerism, MC = mixed chimerism.
|
DISCUSSION
Allo-HSCT has been a curative treatment modality for various non-malignant diseases. However, graft rejection has been an important problem in allo-HSCT for non-malignant diseases in which immune function is active and there was no previous chemotherapy, for which even MAC regimens may be insufficient to achieve CC.18 Therefore, monitoring hematopoietic chimerism after allo-HSCT is important for assessing engraftment and graft rejection in non-malignant diseases.1920 Previous studies revealed that the early analysis of chimerism after allo-HSCT could be used to predict graft rejection, but the earliest time point of chimerism analysis varied among these studies.10202122 Therefore, in this study, we aimed to determine whether the analysis of peripheral blood chimerism status at day 14 could help predict transplant outcomes including graft rejection in patients who underwent allo-HSCT for non-malignant diseases.
In this study, we found that the 5-year EFS was higher in the day 14 CC or low-level MC group than in the day 14 high-level MC group among BM/PBSC transplants, whereas there were no statistical differences in survival rates according to day 14 chimerism status in CB transplants. This might be explained by the difference in engraftment kinetics between BM/PBSC and CB transplants. In this study, hematologic recovery was delayed in CB transplants compared with BM/PBSC transplants, which might be associated with a lower infused number of CD34+ cells in the CB transplants than in the BM/PBSC transplants. Given that the median time to neutrophil recovery in CB transplants was 17 days in our cohort, day 14 may be too early for the chimerism status to have an impact on the transplant outcomes. On the contrary, hematologic recovery after BM/PBSC transplants was relatively faster enough for the early chimerism to be served as a predictor of transplant outcomes.
Full donor chimerism, in general, is not essential for curing non-malignant diseases because stable MC is frequently adequate for functional correction of the underlying disease.18 However, as MC may progress to graft rejection, determining post-transplant chimerism could help identify patients at an increased risk of graft rejection and could be used as a guide for initiating active interventions.119 In the current study, all of the primary engraftment failures occurred in patients with day 14 high-level MC, which suggests that those patients are at greater risk of graft loss and require a prompt intervention such as rapid reduction of immunosuppression. Previous studies also showed that high-level MC correlated with an increased risk of rejection.101316 Breuer et al.10 reported that a high level of recipient-derived T and NK cells heralded graft loss in pediatric patients undergoing allo-HSCT. In a study by Ozyurek et al.,13 33% of children with non-malignant diseases who underwent allo-HSCT showed increasing MC up to 30% of recipient-derived cells and they were at a greater risk of graft loss. Similar findings were noted in a study by Svenberg et al.16 in which graft rejection was found exclusively among patients with high-level MC. On the other hand, none of the patients with day 14 CC/low-level MC experienced primary engraftment failure in the present study. This result is similar to that of a previous study in which patients who showed CC or low-level MC at 1 month after allo-HSCT indicated low risk for graft rejection.22 Notwithstanding the previous studies, we proved that earlier assessment of chimerism status using recipients' peripheral blood is also useful, which enables us to intervene more promptly following BM/PBSC transplants.
In the current study, we observed that the number of infused CD34+ cells was positively correlated with the degree of day 14 donor chimerism. Although a study by Lawler et al.11 showed that there was no correlation between the number of cells infused and chimerism status in allo-HSCT for severe aplastic anemia, other studies revealed that a higher number of infused CD34+ cells was associated with CC.2023242526 Perez-Simon et al.26 reported that 100% of patients receiving a higher dose of CD34+ cells reached CC by days 21–28, but only 44% of patients who received a lower dose of CD34+ cells achieved CC. Another study showed that a greater number of CD34+ cells was associated with higher levels of donor chimerism and rapid achievement of CC on day 28.23 Our results are in line with those reports showing that a higher CD34+ cell dose is associated with a higher probability of achieving better chimerism. Further studies are required to determine the optimal number of CD34+ cells needed to improve the outcomes.
Several studies have used RIC regimens in allo-HSCT for non-malignant diseases.47272829 In one of these studies, Marsh et al.7 reported that MC developed more frequently in the RIC group than in the MAC group (65% vs. 18%, P = 0.011) in patients with hemophagocytic lymphohistiocytosis. In another study, 55 patients with non-malignant disease underwent allo-HSCT with RIC or MAC regimens, and 41% of patients in the RIC group, but 66% of those in the MAC group, achieved CC (P = 0.01).29 However, RIC regimens were more frequently used in the day 14 CC and low-level MC groups than in the high-level MC group in the current study. This may partly be explained by the fact that we regarded conventional conditioning regimens used for severe aplastic anemia as RIC which practically had myeloablative effects for those patients. In addition, because we used various conditioning regimens depending on patients' underlying diseases or pre-transplant performance status, we were not able to conclude the association between day 14 chimerism status and conditioning intensity in this study.
Our study has several limitations such as its retrospective nature, a relatively small population, and heterogeneity in the underlying diseases and transplant types. Nevertheless, given the rarity of transplant candidates with non-malignant disease in the pediatric population, our results may provide useful insight about the impact of early chimerism on the transplant outcomes in pediatric non-malignant diseases.
In conclusion, our data suggest that analysis of post-transplant peripheral blood chimerism on day 14 may predict transplant outcomes in patients with non-malignant diseases after BM/PBSC transplantation. In CB transplants, however, the earliest clinically relevant time point should be defined in further studies. Larger multicenter prospective studies are required to verify the relationship between early chimerism and transplant outcomes.
 XML Download
XML Download