

 PDF
PDF Citation
Citation Print
Print



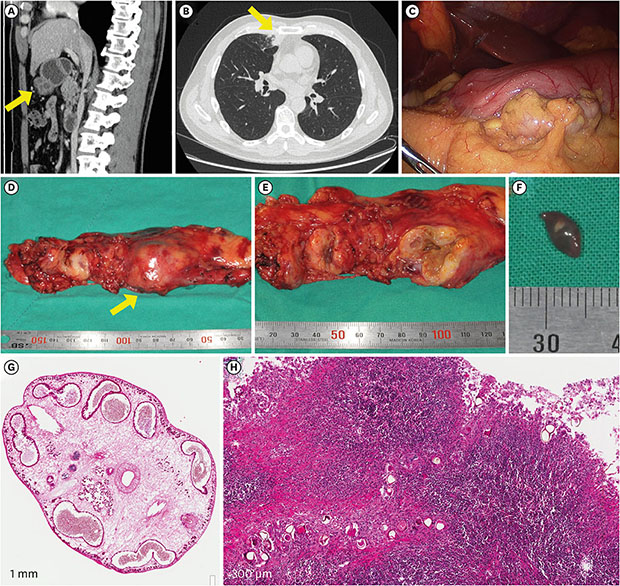
A previously healthy 49-year-old man was referred to the hospital for a symptomatic gastric submucosal tumor that was detected in the computed tomography (CT) during a health screening in July 2017 (Fig. 1A). There was incidental bronchopneumonia in the anterior segment of the right upper lobe on the chest CT (Fig. 1B). The submucosal septate cystic mass was removed by laparoscopic gastric wedge resection. During the operation, multiple tiny nodules were found in the entire peritoneum, omentum, transverse colon, and the liver surface (Fig. 1C). When the mass was dissected, brownish discharge poured out and an oval-shaped worm was found (Fig. 1D-F). The trematode was 5–6 mm long and 4–5 mm wide and was characterized by an oral sucker, a ventral sucker, a multilobed ovary, testes in the posterior region of the body, teguments covered with spines, and well-developed vitellaria (Fig. 1G). Multiple eggs (size, 50–60 µm) were observed in the lymph node which showed granulomatous inflammation with eosinophil infiltration (Fig. 1H). Additional history taking was taken. He is an office worker living in Seoul, and has eaten freshwater crabs several times. Considering the clinical and pathologic findings, praziquantel (25 mg/kg three times a day for two days) was prescribed after the diagnosis of paragonimiasis. Pulmonary paragonimiasis is sometimes mistaken for pulmonary tumors. However, in the case of extrapulmonary paragonimiasis, to suspect parasite infection is not easy before pathologic confirmation. Prior studies have reported some extrapulmonary paragonimiasis identified in the abdominal cavity.123 Here we report the first case of paragonimiasis mimicking gastric submucosal tumor.
This manuscript was written after receiving the patient's agreement of the publication including private clinical records and images.
 XML Download
XML Download