

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The Sewol Ferry Disaster was a tragic event in Korea. In April 2014, 476 people were on board the Sewol Ferry, including 325 Danwon High School students and 14 teachers; 304 passengers died in the disaster (295 corpses were recovered, and nine passengers were missing), and 172 passengers survived. Only 75 students and three teachers escaped before the ferry sank.12 Immediately after the disaster, over one hundred and fifty psychiatrists volunteered and offered crisis intervention sessions to the Danwon High School students who were indirectly exposed to the disaster.
Disasters undermine the mental health of the affected parties and the community and result in property damage, the loss of life,3 and severe mental problems, such as posttraumatic stress disorder (PTSD) and acute stress disorder (ASD).4 In addition, the damage from a disaster includes the long-term suffering experienced by the survivors and the bereaved family and the physical health deterioration resulting from the disaster. A disaster affects not only the individuals who are the direct victims but also the entire family, and if they are left untreated, long-term problems can arise and lead to social problems.5
After a disaster, the involved parties and the people around them experience psychological problems such as a complicated mourning reaction, PTSD, depression, anxiety, and suicide.6 The prevalence of PTSD, which is characterized by symptoms, such as flashbacks, nightmares, intense alerts, and avoidance of events, after a technical disaster is 15%–75%.7 Disasters also lead to collective and massive stress,8 leading to more significant social disruption.9 Therefore, to minimize the social collapse caused by a disaster, supporting the victim, the bereaved family, and the general public in the community is necessary.10
Previously, there have been many reports of school-related disasters. In October 1966, a coal slag heap collapsed onto a primary school killing 116 children; and 145 children survived.11 On October 21, 1988, 334 of 400 schoolchildren survived the sinking of the cruise ship Jupiter.12 In February 1984, a sniper fired onto a crowded elementary school playground.13 Childhood trauma can lead to PTSD, and PTSD symptoms are significant because they can occur throughout adulthood.14 School is a place in which the exchange of feelings among students, teachers and various related people occurs. Therefore, a disaster occurring at a school, where the emotional distance is close, can be even more stressful. During adolescence, peers play an important role because they create emotional bonds with their friends.15 Previous studies have reported that adolescents with close emotional proximity are more likely to experience symptoms after a disaster.16
Previous studies have shown that early interventions following disasters prevent progression to PTSD.1718 To facilitate access to appropriate care and minimize unmet healthcare needs in populations affected by a disaster, proactive early outreach has been emphasized in several recent consensus documents.19 Several systematic studies have investigated psychiatric outreach following major disasters. For example, Disaster Psychiatry Outreach (DPO) is a nonprofit organization founded in 1998 that provided volunteer psychiatric care to 9/11 survivors in New York City.20 Additionally, volunteer psychiatrists conducted an outreach survey to improve mental health literacy and bridge the communication gaps among 141 Japanese citizens who experienced the Great East Japan Earthquake, and more than one-quarter of the respondents met the expected PTSD criteria.21 In the Jerusalem Trauma Outreach and Prevention Study (J-TOPS), survivors of traumatic events were assessed after visiting a hospital's emergency department (ED) with the Structured Clinical Interview from the DSM-IV (SCID-IV), and 443 (59%) patients were diagnosed with PTSD.22
In addition to direct exposure, indirect victims of traumatic events experience symptoms, such as invasion, avoidance, and excessive awakening, even if they did not encounter the traumatic experience directly.23 Indirect experience with trauma can lead to symptoms, including depression, anger, and PTSD, that are similar to those exhibited by people with direct traumatic experiences.24 Crisis response focuses on disaster survivors and can easily overlook victims who were not at the scene of the attack. People who have indirect experience with a traumatic incident also complain about psychiatric stress and mental symptoms.25
To the best of our knowledge, no studies have investigated the activities of psychiatrists providing psychological support in crisis situations at the scene of a large-scale accident in one school. This study reports on the 1) frequent symptoms, 2) possible diagnoses at the interview, 3) individual recommendations for students who had indirect experience with the disaster (from volunteer psychiatrists) and 4) implications for future policy plans for student-related disasters.
METHODS
The study questionnaires were distributed to psychiatric volunteers who conducted outreach at Danwon High School. Our previous report described the study process.26 A total of 72 out of the 157 (45.9%) volunteer psychiatrists answered the questionnaires. Participants performed a clinical interview to assess psychiatric symptoms in a total of 212 students.26 The surveys included information regarding the psychiatrist volunteers' age, gender, residence, work place, highest level of education, hospital level, and subspecialty. Information regarding the total number of students interviewed, average intervention time per session (minutes), total intervention time per day (hours), intervention period, total number of intervention sessions, chief complaints, psychiatric symptoms, possible diagnosis, and individual recommendations based on the interviews was also obtained.
RESULTS
From the second day to the 138th day after the disaster, 167 psychiatric volunteers conducted emergency counseling outreach services to approximately 550 cases at Danwon High School.27 Seventy-two (43.1%) of the 167 volunteers and 212 (38.6%) of the 550 cases could be reached. The intervention was conducted for 7 months, beginning on the day immediately after the disaster, and was maintained for 229 days.
The demographic characteristics of the psychiatrist volunteers are shown in Table 1. Approximately 51 (70.83%) psychiatrist volunteers were women, and 21 (29.17%) psychiatrist volunteers were men. In total, 58 (80.5%) psychiatrists subspecialized in children and adolescents.
Table 1
Demographic characteristics of the psychiatrist volunteers (n = 72)

The chief complaints, psychiatric symptoms, clinical diagnoses and interview results of the students are shown in Tables 2, 3, 4.
Table 2
Chief complaints of the students exposed to the Sewol Ferry Disaster (n = 212)
Table 3
Psychiatric symptoms of the students exposed to the Sewol Ferry Disaster (n = 212)

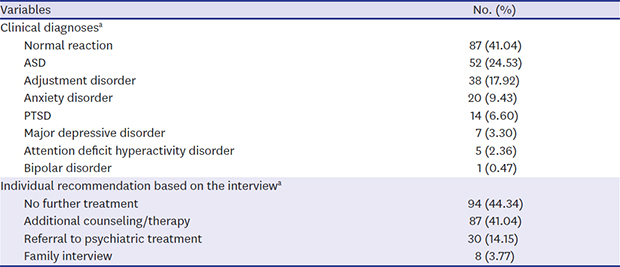
Table 4
Clinical diagnoses and interview results of the students exposed to the Sewol Ferry Disaster (n = 212)

The most frequent chief complaint was mental health problems (60.38%, n = 128). The other chief complaints included problems with colleagues, problems with family members, academic problems and problems with romantic relationships (37.74%, n = 80; 26.89%, n = 57; 15.57%, n = 33; 6.13%, n = 13, respectively).
Anxiety was the most common psychiatric symptom exhibited by the students (76.89%, n = 163). Around 51% of students presented depressed mood and poor concentration (51.42%, n = 109; 50.94%, n = 108, respectively). Symptoms such as sleep problems, anger outbursts or aggressive behaviors reported between 20%–30% range (29.72%, n = 63; 27.36%, n = 58; 21.70%, n = 46; 19.81%, n = 42, respectively). And other symptoms like palpitation, social isolation/withdrawal, recurrent distressing dreams/nightmares, headache, nervous behavior, always being on guard for danger, flashback/loss of appetite, shortened meaning of the future, delusions/hallucinations and hyperventilation were reported less than 20% (18.40%, n = 39; 16.04%, n = 34; 15.57%, n = 33; 15.09%, n = 32; 8.96%, n = 19; 8.02%, n = 17; 4.25%, n = 9; 3.77%, n = 8, respectively).
Regarding the clinical diagnoses at the outreach site, 41.04% (n = 87) of the students did not have any clinical diagnosis. However, the remaining students were diagnosed with ASD, adjustment disorder, anxiety disorder, PTSD, major depressive disorder, and attention deficit hyperactivity disorder (ADHD) (24.53%, n = 52; 17.92%, n = 38; 9.43%, n = 20; 6.60%, n = 14; 3.30%, n = 7; 2.36%, n = 5).
More than half of the students were considered to require “additional counseling/therapy (41.04%)” or “referral to psychiatric treatment (14.15%),” whereas 44.34% (n = 94) of the students had “no further recommendation for treatment.” A few students were recommended to have a “family interview” (3.77%, n = 8).
DISCUSSION
This study is the first to report on how psychiatric service professionals reacted to a national-level disaster at a school in Korea. Our study investigated the outreach intervention provided by psychiatrists at one school. When reviewing various studies related to disaster, it was found that the incidence of PTSD showed different results depending on the age of the victim, the timing of the intervention, prior experiences before the traumatic events, and the clinician who performed the evaluation.2829303132 Therefore, we focused on related studies using the measurements used in the clinicians' evaluations and structured or semi-structured interviews with the children and adolescents.33
After the September 11, 2001 terrorist attack in New York City, many studies were conducted to query the survivors, families, and community about the psychological and psychiatric effects they experienced throughout the trauma. Pandya et al.20 analyzed the DPO records of hundreds of psychiatric pro bono care cases from September 12, 2001 to November 20, 2001. DPO is an organized cadre of volunteer psychiatrist that offers psychiatric assistance to individuals at the New York City Family Assistance Center. The subjects self-refer, but referrals are also provided by other governmental and nonprofit agencies; approximately half of the patients need psychotropic medication. According to their written clinical encounters with a psychiatrist, PTSD was diagnosed in 14% (n = 99) of people exposed to the disaster, and the patients' ages ranged from 3 to 78 years. Hoven et al.34 screened 8,236 public school students in grades 4 through 12 (stratified by exposure levels across New York City) 6 months after the 9/11 terror attack using the Diagnostic Interview Schedule for Children Predictive Scales (DISC-PS) and reported that the rate of PTSD was 10.6%. The percentage of PTSD reported in these two studies is higher than that observed in our study (6.60%) because these studies included subjects who were directly exposed. In our study, the subjects were not directly exposed but were closely related to the victims of the disaster. In addition, the school provided pro bono psychiatric services daily, enabling the availability of the psychiatrists to have protective effects. The school environment provides social support, playing a protective role in children and adolescents following disaster exposure.35 Meanwhile, other reoprts36 have studied 166 vulnerable children (mean age, 11 years; range, 7–15 years) in Boston who were exposed to the 9/11 disaster only through the media. These authors found that the prevalence of PTSD was 5.4% according to the Kiddie Schedule for Affective Disorders and Schizophrenia, Epidemiologic Version (K-SADS-E). This PTSD rate was similar to our result, even though our sample was not driven by a vulnerable population.
Recent studies investigating natural disasters, such as typhoons or earthquake, according to clinician ratings3738 have shown that the rate of PTSD among adolescents ranged from 25.8% to 2.5%. Three months after the Typhoon Morakot in Taiwan, 271 adolescents (mean age, 13.4 years; range 12–15 years) who had been evacuated from their homes were interviewed using the Mini-International Neuropsychiatric Interview,37 and the rate of PTSD among these adolescents was 25.8%. In their study, three-quarters of the subjects were aboriginal adolescents from an aboriginal tribe considered vulnerable to severe mental health problems. The different types of disasters and the vulnerability of the participants could account for this difference. Notably, the manner in which traumatic stress symptoms appear varies according to previous experiences prior to the disaster and depends on the degree of exposure to the traumatic events.39 However, one study in China reported a low rate of PTSD. More than six months after the Wenchuan earthquake in 2008, 3,208 adolescents (mean age, 13.8 years; range, 12–18 years) exposed to the earthquake were assessed using the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children Lifetime version (Kiddie-SADS-L).38 The researchers found that the overall prevalence of PTSD was 2.5%. The latter study showed a low rate of PTSD likely because of the characteristics of the participants, differences in the study methods, and social support provided by the Chinese government, nongovernmental organizations, and international organizations; timely and effective assistance might have played an essential role in reducing the prevalence of PTSD.
Regarding psychiatric symptoms and suggested clinical diagnosis from the point of view of the psychiatrists, the fact that the response related to traumatic symptoms was 58.96% can be interpreted two ways. First, over 58% of students may need psychiatric follow-up. It has been demonstrated in a previous study40 that of the indirect victims after the tsunami in Sweden in 2004, 41% reported posttraumatic stress reactions and 62% reported impaired general mental health. In this study, it is the result of interviewing students during the acute phase when PTSD is difficult to diagnose (73.2% interviewed within a month after the disaster). These findings are consistent with research findings of middle school students (n = 197) who experienced the Lushan earthquake in Sichuan, China, that 28.4% of them suffered from ASD. Furthermore, it is similar to a previous study41 that post-traumatic stress could affect adolescent functioning, for instance, separation anxiety, aggressiveness, delinquency, hyperactivity, and dependence. After the September 11 terrorist attacks, the prevalence of PTSD symptoms was higher not only in persons who were more directly affected by the attacks, but also in a substantial number of persons who were not directly affected by the 9/11 terror attacks.42 This demonstrates that indirect experience can meet the PTSD criteria and affect the general population, even though the type and timing of the disaster are different.
Second, nevertheless, many students need only psychoeducation. On the basis of our study results, it does not suggest that all the symptoms that appear in students correspond to major psychiatric diagnoses. It has been demonstrated in this study that they were also associated with high level of psychiatric symptoms such as anxiety, depression, and difficulty concentrating; in order of frequency. It is similar to prior studies of outcomes that the majority of children exposed to the disasters do not develop diagnosable psychopathology.30 In general, it is common to think only of PTSD as the principal response to traumatic events, but normal response and distress reactions are frequent in the acute-phase.43 It is necessary to distinguish students' psychiatric symptoms well at the acute phase after the disaster. As a result of the psychiatric interview, 44.34% of them reported that they completed the psychological education and did not suggest follow-up intervention for students. The results suggest that even adolescents with normal mood response need to consider continuous observation and professional intervention.
This study has several limitations. First, the results were based on the memory recall of the psychiatrist volunteers. Second, the subjects in this study consisted only of students attending Danwon High School. Third, no structural, formal diagnostic process using diagnostic tools was implemented. Despite these limitations, our findings emphasize that psychosocial management should be provided to students immediately after a disaster because effective early intervention is a factor that can reduce the incidence of PTSD in adolescents. Moreover, it is essential for mental health specialists to provide consultations to adolescents during the acute phase after a disaster, during which the frequency of the psychiatric symptoms and reactions can be observed. In various countries, follow-up studies involving children and adolescents exposed to disasters have been conducted.
In case of the Wenchuan earthquake, “timely and effective assistance” might have played an essential role in reducing the prevalence of PTSD as mentioned above. After the disaster, the substantial disparity between the apparent need for, and receipt of, mental health services by children could lead to long-standing psychological health problems.44 Therefore, even children who are not in a therapeutic relationship must be identified, referred, and treated.44 Thus, well-organized professional volunteering activities, such as the DPO of the United States to survivors in New York City20 or volunteer psychiatrists conducting outreach after the disaster of the Great East Japan Earthquake,21 during the aftermath of a disaster are necessary.
The results of this study could provide empirical evidence that crisis intervention is essential not only for students directly experiencing disasters but also for indirectly exposed students. Therefore, in the event of a disaster, psychiatrists should be prepared to intervene in systematically providing mental health services to the student. When required, intensive intervention should be systematically organized and linked to community service organizations and should consider effective policies. Consequently, a better understanding of youth exposed to disasters could inform future treatment protocols.
 XML Download
XML Download