

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The medical insurance system could influence the prognosis of cancer patients. Early diagnosis and effective treatment are main factors for better prognosis of cancer patients. They are closely associated with medical insurance status. Previous studies have reported that patients with Medicaid or no health insurance are more likely to be diagnosed with late stage cancers at diverse sites (including the breast) compared to patients with health insurance [1,2,3]. It has been reported that older minority women without health insurance or insured by Medicare and Medicaid face challenges in receiving optimal care for breast cancer [4]. The relationship between medical insurance system and prognosis of cancer patients has been reported in various cancers, including breast cancer [5], head and neck cancer [6], Hodgkin lymphoma [7], germ cell tumors [8], colorectal cancer [9], childhood cancer [10], and cancers in young adults [11]. Recently, Ellis et al. [12] have analyzed data of 1,149,891 cancer patients from California Cancer Registry and reported that survival improvements are exclusively limited to patients with private or Medicare insurance while survival for patients with other public insurance or no insurance is largely unchanged or declined.
Medical insurance systems are different across counties. Their impacts on the prognosis of breast cancer patients are also different. ‘Medical Insurance Act’ was legislated in 1963 in the Republic of Korea. The first public medical insurance system was then launched in 1977. Medical insurance coverage was expanded to smaller companies in 1988. Universal coverage for rural and urban areas by medical insurance societies was implemented in 1989 [13]. National Health Insurance system of Korea provides 100% coverage for all Koreans. Although some studies have reported the association between medical insurance status and the prognosis of breast cancer, the association between the Korean public medical insurance system and the prognosis of breast cancer has not been reported. Therefore, the objective of this study was to investigate the prognostic influence of Korean public medical insurance system on breast cancer patients using breast cancer registry data from our institute.
METHODS
Patients
Patients diagnosed as primary breast cancer who received treatment at Seoul Metropolitan Government - Seoul National University Boramae Medical Center were included as subjects of this study. These patients had been registered in the Boramae Hospital Breast Cancer Registry. The number of total patients registered in this database was 1,449 at the time of this study. We excluded 50 patients who were diagnosed after December 31, 2016. We also excluded 119 patients who were diagnosed before January 1, 2000. We further excluded 156 patients diagnosed as stage 0 and 46 patients without information of their medical insurance status. In this study, we excluded 10 patients with other types of insurance (not National Health Insurance or Medical Aid). Finally, data of 1,068 patients with primary invasive breast cancer were analyzed.
The Institutional Review Boards approved this study (Seoul Metropolitan Government - Seoul National University Boramae Medical Center, 16-2017-69) and performed in accordance with the principles of the Declaration of Helsinki. The informed consent of this study was waived.
Clinicopathologic parameters
Patient age was defined as the age at the time of diagnosis of primary breast cancer. TNM staging was described according to the 7th edition of the American Joint Committee on Cancer. Hormonal receptor (HRc) status was defined as positive when immunohistochemistry test for either estrogen receptor or progesterone receptor was positive. HRc was defined as negative when both estrogen receptor and progesterone receptor were negative. Human epidermal growth factor receptor 2 (HER2) was defined as negative when immunohistochemistry results were negative or 1+. HER2 was defined as positive when immunohistochemistry results were 3+. When immunohistochemistry results were 2+, positivity of HER2 was defined according to results of in situ hybridization. Histologic grade and nuclear grade were defined according to modified Scarff-Bloom-Richardson grading system. Body mass index (BMI) was defined as the ratio of body weight in kilograms to height in square meters. Education level was classified into 2 groups according to the length of education period: high education level group (≥12 years) and low education level group (<12 years). Recurrence was defined as any first event of local, regional, distant recurrence, or contralateral breast cancer during the follow-up period.
Medical insurance status
The Korean National Health Insurance system has two main medical insurance programs: National Health Insurance program and Medical Aid program [13,14]. The National Health Insurance program covers the whole population as a social insurance benefit scheme. It is a compulsory short-term insurance. The Medical Aid program is managed by the Korean government as a public assistance scheme to secure the minimum livelihood of low-income households and assist with self-help by providing medical services. In this study, Korean public medical insurance status was classified into 2 groups: National Health Insurance group and Medical Aid group. We excluded patients with other minor types of insurance, such as insurance for disabled, foreigners, or industrial accidence, long-term care insurance, and so on. We also excluded patients with no insurance or no information of insurance. Private insurance programs were not analyzed in this study.
Statistical analyses
Two-sample t-test was used to determine differences in expression levels of biological parameters while Pearson chi-square test was used to determine differences in clinicopathologic characteristics between groups. Overall survival (defined as the time duration from operation to death from any cause) and recurrence-free survival (time duration from operation to recurrence of any type) were analyzed. Kaplan-Meier estimator was used to analyze survival rates. Log-rank test was used to determine the significance of differences between 2 or more survival curves. Cox proportional hazards model was used for univariate and multivariate analyses. Hazard ratio (HR) and 95% confidence interval (CI) were calculated. For multivariate analysis, various models were designed. Details of each model are described in table legends. All statistical analyses were carried out using IBM SPSS Statistics ver. 20.0 (IBM Corp., Armonk, NY, USA). All tests were 2-sided. Statistical significance was considered when P-value was less than 0.05.
RESULTS
Clinicopathologic characteristics
The total number of subjects was 1,068 and their mean age was 54.7 ± 12.5 years (median, 53.0 years; range, 16–93 years). Operation dates were between January 2000 and December 2016. Their mean follow-up period was 67.6 ± 49.2 months (median, 54.0 months; range, 1–209 months). Total numbers of deaths and recurrences during this period were 157 (14.7%) and 147 (13.8%), respectively. Clinicopathologic characteristics of all subjects according to medical insurance status are summarized in Table 1. Proportions of National Health Insurance and Medical Aid were 90.0% and 10.0%, respectively. Mean age of patients with Medical Aid was significantly older than that of patients with National Health Insurance (60.1 ± 11.9 years vs. 54.1 ± 12.4 years, P < 0.001). The Medical Aid group showed higher proportion of patients with tumor size > 2 cm, more advanced stages, age > 50 years, and low education level compared to the National Health Insurance group. The Medical Aid group also showed higher proportion of patients who received mastectomy and those who received no radiation therapy.
Survival analysis
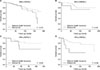
The Medical Aid group showed worse prognoses compared to the National Health Insurance group both in overall survival (P = 0.001) and recurrence-free survival (P = 0.006) (Fig. 1). The 5-year overall survival rate and 10-year overall survival rate were 88.9% and 77.1% in the National Health Insurance group and 76.1% and 62.8% in the Medical Aid group, respectively. The 5-year recurrence-free survival rate and 10-year recurrencefree survival rate were 85.1% and 75.0% in the National Health Insurance group and 71.2% and 64.4% in the Medical Aid group, respectively. Detailed survival rates according to medical insurance status are described in Supplementary Table 1. Although there were no significant differences in local recurrence, regional recurrence, or contralateral breast cancer between the 2 groups, the Medical Aid group showed worse prognosis regarding distant recurrence (P = 0.014) (Fig. 2). The 5-year local recurrence-free survival rate and 10-year local recurrence-free survival rate were 96.6% and 93.5% in the National Health Insurance group and 94.7% and 92.5% in the Medical Aid group, respectively. The 5-year regional recurrence-free survival rate and 10-year regional recurrencefree survival rate were 96.5% and 93.0% in the National Health Insurance group and 93.6% and 93.6% in the Medical Aid group, respectively. The 5-year distant recurrence-free survival rate and 10-year distant recurrence-free survival rate were 92.3% and 86.4% in the National Health Insurance group and 88.1% and 76.5% in the Medical Aid group, respectively. The 5-year contralateral breast cancer-free survival rate and 10-year contralateral breast cancer-free survival rate were 98.4% and 96.9% in the National Health Insurance group and 99.1% and 95.1% in the Medical Aid group, respectively. The Medical Aid group showed worse prognosis for subgroup of HRc(−)/HER2(−) (P = 0.006). However, there were no significant survival differences in overall survival for other subgroups (HRc(+)/HER2(+), HRc(+)/HER2(−), and HRc(−)/HER2(+)) between the 2 groups (Fig. 3). In the HR(+)/HER2(−) subgroup, the 5-year overall survival rate and 10-year overall survival rate were 90.5% and 76.0% in the National Health Insurance group and 89.2% and 69.7% in the Medical Aid group, respectively. In the HR(+)/HER2(+) subgroup, the 5-year overall survival rate and 10-year overall survival rate were 96.0% and 81.5% in the National Health Insurance group and 74.1% and 74.1% in the Medical Aid group, respectively. In the HR(−)/HER2(+) subgroup, the 5-year overall survival rate and 10 year overall survival rate were 84.2% and 79.7% in the National Health Insurance group and 58.3% and 58.3% in the Medical Aid group, respectively. In the HR(−)/HER2(−) subgroup, the 5-year overall survival rate and 10-year overall survival rate were 83.0% and 75.5% in the National Health Insurance group and 45.0% and 45.0% in the Medical Aid group, respectively. Further comparisons of clinicopathologic features between the National Health Insurance group and The Medical Aid group according to each breast cancer subtype are described in Supplementary Table 2.
Subgroup analysis
Subgroup analyses with a forest plot revealed that prognoses of the Medical Aid group were worse than those of the National Health Insurance group regardless of estrogen receptor, progesterone receptor, chemotherapy, or endocrine therapy (Table 2). Although the Medical Aid group showed inferior prognosis for subgroups with tumor size > 2 cm, negative lymph node, stage II/III, negative HER2, histologic grade 1/2, age > 50 years, BMI ≤ 25 kg/m2, no radiation therapy, no Herceptin therapy, and mastectomy, there were no significant difference in prognosis for subgroups with tumor size ≤ 2 cm, positive lymph node, stage I, positive HER2, histologic grade 3, age ≤50 years, BMI >25 kg/m2, lumpectomy, radiation therapy, or Herceptin therapy. In all subjects, the Medical Aid group showed inferior prognosis compared to the National Health Insurance group (HR, 1.973; 95% CI, 1.324–2.940; P = 0.001).
Univariate and multivariate analysis
Univariate analysis revealed that 13 factors were significant, including medical insurance status, tumor size, nodal positivity, metastasis, estrogen receptor, progesterone receptor, histologic grade, lymphovascular invasion, age, education level, operation, chemotherapy, and endocrine therapy (Table 3). Medical insurance status was a significant independent prognostic factor in the following 3 models: model 1 (HR, 1.975; 95% CI, 1.092–3.571; P = 0.024), model 2 (HR, 2.188; 95% CI, 1.093–4.379; P = 0.027), and model 3 (HR, 1.680; 95% CI, 1.115–2.529; P = 0.013). However, it was not a significant factor in model 4. In model 1, medical insurance status was adjusted with 11 factors which were significant by univariate analysis. Medical insurance status was adjusted with 10 clinicopathologic factors in model 2, and it was adjusted with 5 treatment factors in model 3. In model 4, medical insurance status was adjusted with all of 15 factors including 10 clinicopathologic factors and 5 treatment factors.
DISCUSSION
This study aimed to reveal the prognostic influence of Korean public medical insurance system on breast cancer patients. Our results revealed that the Medical Aid group showed worse prognosis compared to the National Health Insurance group in terms of overall survival and recurrence-free survival. Medical insurance status was a strong independent prognostic factor in both univariate and multivariate analyses. To the best of our knowledge, this is the first study that reveals the association between the Korean public medical insurance system and the prognosis of breast cancer patients. Several previous studies have analyzed insurance data in foreign countries and reported similar results. Hsu et al. [15] have analyzed 52,048 female breast cancer patients aged 18 to 64 years using Surveillance, Epidemiology, and End Results 18 registries database and reported that the HR of breast cancer specific survival is increased in association with Medicaid (HR, 1.40; 95% CI, 1.30–1.51) and those without insurance (HR, 1.61; 95% CI, 1.41–1.84) compared to those with private insurance [15]. Niu et al. [16] have analyzed the relationship between medical insurance status and survival using data of 17,939 patients diagnosed as breast cancer during 1999–2004 in New Jersey. They reported that 5-year cause-specific survival rates were 89.1% for private insurance, 76.4% for Medicaid, and 74.7% for no insurance, respectively. They also reported that HRs were 1.56 (95% CI, 1.29–1.88) for Medicaid and 1.44 (95% CI, 1.22–1.69) for those who had no insurance with reference to those who had private insurance [16]. Ayanian et al. [17] have analyzed data of 4,675 women aged 35 to 64 years who were diagnosed with invasive breast cancer from 1985 through 1987 by linking New Jersey State Cancer Registry records to hospital-discharge data. They reported that the adjusted risk of death from all causes was 49% higher (95% CI, 0.20–0.84) for uninsured patients and 40% higher (95% CI, 0.40–0.89) for Medicaid patients than that for privately insured patients at 54 to 89 months after diagnosis. Most of these previous studies regarding this issue are from the United States of America. Although the medical insurance system of the United States of America is different from that of the Republic of Korea, final results are similar between the two countries. Patients whose medical insurance is covered by Korean Medical Aid or American Medicaid/Medicare are associated with worse prognosis compared to patients with Korean National Health Insurance or American private insurance, respectively. In this study, medical insurance status was a significant prognostic factor by univariate analysis. Moreover, medical insurance status was a significant independent prognostic factor after being adjusted with factors which were significant by univariate analysis. It was also a significant independent prognostic factor when adjusted by clinicopathologic factors or treatment factors. These findings imply that medical insurance status has an independent prognostic role which is irrespective of prognostic roles of clinicopathologic factors or treatment factors.
The Medical Aid group showed worse survival rates compared to the National Health Insurance group. Unfavorable clinicopathologic features of the Medical Aid group could explain this result. The Medical Aid group showed more advanced T categories compared to the National Health Insurance group, consequently having more advanced stages. Larger tumor size of the Medical Aid group could be the main reason why the proportion of patients who received mastectomy was higher in the Medical Aid group than that in the National Health Insurance group. As a result, the proportion of patients who did not receive radiation therapy was lower in the Medical Aid group. There were no significant differences between the 2 groups in terms of systemic therapy such as chemotherapy, anti-HER2 therapy, or endocrine therapy. These findings imply that patients with Medical Aid have a tendency to be diagnosed at advanced stages. Delayed diagnosis of the Medical Aid group could be one major reason for poor survival outcome. Some papers have reported the association between medical insurance status and the initial stages of breast cancer patients at initial diagnosis. For example, Hsu et al. [15] have reported that the odd ratios of breast cancer patients with more advanced stages are increased in women with Medicaid (odds ratio, 2.36; 95% CI, 2.19–2.55) and those with no insurance (odds ratio, 2.64; 95% CI, 2.29–3.04) compared to those with private insurance [15]. Coburn et al. [18] have reported that mean tumor sizes are 18.5 mm for those with private insurance, 20.9 mm for those with Medicare, 24.2 mm for those with Medicaid, and 29.5 mm for those uninsured (P < 0.001 for all). They also reported that 71.5% of those with private insurance underwent breast-conserving surgery compared with 64.2% of those with Medicare (P < 0.001), 65% of those with Medicaid (P = 0.097), and 65.4% of those uninsured (P = 0.234) among women with nonmetastatic T1/T2 tumors. Other studies have also reported similar results, showing that patients with Medicaid, Medicare, or no insurance are diagnosed with more advanced T, N, M, and summary stages at initial diagnosis compared to those with private insurance [17,19,20,21,22].
The mean age of the Medical Aid group was older than that of the National Health Insurance group and the proportion of patients with age > 50 years was higher in the Medical Aid group. Age could be a main factor causing the worse prognosis of the Medical Aid group. Chen et al. [23] have analyzed 133,057 female breast cancer patients from 2004 to 2008 using the Surveillance, Epidemiology, and End Results database. They reported that age > 60 years at diagnosis was an independent predictor of poor prognosis with respect to overall survival (HR, 2.77; 95% CI, 2.62–2.94). They also found that the effect of age was less prominent with respect to breast cancer-specific survival (HR, 1.46; 95% CI, 1.37–1.56) compared to age < 40 years [23]. Zhu et al. [24] have analyzed 9,908 female triple negative breast cancer patients using the Surveillance, Epidemiology, and End Results database. They reported that elderly (≥70 years) patients with relatively advanced diseases exhibited distinctly worse cancer-specific (log-rank, P < 0.001) and overall survival (log-rank, P < 0.001) than their young counterparts (<70 years) [24].
The proportion of patients with low education level was higher in the Medical Aid group. Education level is one of main components of socioeconomic status. The association of education level and breast cancer prognosis has been reported in many previous studies [25,26]. Our previous study has also shown that education level is a strong independent prognostic factor for breast cancer in subgroup aged >50 years regardless of molecular subtypes of breast cancer [27]. Favorable clinicopathologic features and active treatments can explain the superior prognosis in the high education level group [27]. A previous study has reported that area-level educational attainment is significantly associated with less favorable features [28]. When the proportion of high school educated persons in an area is decreased, the odd ratio of having less favorable breast cancer is increased [28].
The present study showed that distant recurrence rate was higher in the Medical Aid group compared to that in the National Health Insurance group. However, there were no significant differences in local recurrence, regional recurrence, or contralateral breast cancer rate between the two groups. More advanced stages at initial diagnosis in the Medical Aid group than that in the National Health Insurance group could explain the higher rate of distant recurrence, consequently leading to higher mortalities. We could not find any study reporting recurrence patterns of breast cancer patients according to medical insurance status. In this study, the prognostic impact of medical insurance status in breast cancer according to subgroups stratified by various clinicopathologic factors was analyzed. Although the Medical Aid group showed worse prognosis compared to the National Health Insurance group in many subgroups, there were no differences in other subgroups. The Medical Aid group showed worse prognosis in the subgroup with age >50 years. However, there was no significant difference in prognosis for subgroup with age ≤50 years between the two groups. The Medical Aid group showed inferior survival rate compared to the National Health Insurance group only for the HRc(−)/HER2(−) subtype. In general, the HRc(−)/HER2(−) subtype has the worst prognosis compared to the other breast cancer subtypes, and has an easy tendency to show a prognostic difference according to a proposed prognostic factor. Although further analyses of the clinicopathologic features between the National Health Insurance group and the Medical Aid group according to breast cancer subtype was performed, we could not find significant differences between them in the HRc(−)/HER2(−) subtype. Further studies with large scales are needed to validate the prognostic role of health insurance status in each breast cancer subtype.
This study has several limitations. First, the medical insurance system is not the same across countries. Although findings of this study had limitations for generalization, they could be still valuable to investigate the prognostic impact of each medical insurance system on breast cancer across countries. Second, the number of subjects used in this study is relatively small. Therefore, the statistical power might not be robust, especially in subgroup analysis. For example, subgroup analysis of this study showed a better overall survival rate of the Medical Aid group with metastasis compared to the National Health Insurance group with metastasis. As the subject number of the Medical Aid group with metastasis was too small (n = 5), one subject with exceptionally long follow-up interval (169 months) could affect the significance of survival analysis. For another example, although we showed the worse prognosis of the Medical Aid group only in the HRc(−)/HER2(−) subtype in this study, we could not find further evidences supporting causalities for these results because of relatively small subject number. Further studies with a large number of subjects are needed to validate results of this study. Third, we could not evaluate breast cancer-specific survival due to unavailability of data. We could not obtain detailed information for socioeconomic status of patients either. Last, as this study investigated breast cancer patients of a single institute, selection bias issue needs to be considered. Multi-institutional studies are needed in the future to overcome this issue.
In conclusion, the Medical Aid group showed worse prognosis compared to the National Health Insurance group. Medical insurance status was found to be a strong independent prognostic factor in breast cancer. Unfavorable clinicopathologic features could explain the worse prognosis of the Medical Aid group. Therefore, careful consideration should be given to medical insurance status as one important prognostic factor for breast cancer patients in clinical setting. More active public screening system to detect breast cancer at earlier stage could help to improve survival outcome of the Medical Aid group with breast cancer.





 XML Download
XML Download