

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Bronchial asthma is a disease that causes reversible airway obstruction and nonspecific airway hyper-reactivity due to chronic airway inflammation. Therefore, monitoring airway inflammation, which is one of the main features of the disease, is important for diagnosing and controlling bronchial asthma. The use of fractional exhaled nitric oxide (FeNO), which is a convenient and sensitive marker of eosinophilic airway inflammation, is beginning to spread in routine practice as a noninvasive monitoring method [1]. Long-term management of bronchial asthma based on FeNO has been reported to decrease acute exacerbations and reduce the frequency of corticosteroid treatments [2]. However, there are also other reports that there was no difference in the rates of acute exacerbation or treatments in hospitalization in long-term management of bronchial asthma using FeNO levels [2], suggesting that FeNO is not conclusive yet in the long-term management of bronchial asthma. Therefore, we combined FeNO and spirometry which are both used often in routine to manage bronchial asthma.
MATERIALS AND METHODS
Patients
Subjects were school-aged children 7 years and older with bronchial asthma who underwent FeNO testing in January 2015 to May 2016 and regularly visiting the Haga Red Cross Hospital. Diagnosis of bronchial asthma followed the Treatment and Management Guidelines of Pediatric Bronchial Asthma 2012 issued by the Japanese Society of Pediatric Allergy and Clinical Immunology with parameters of clinical symptoms and blood test results [3]. Long-term management also followed the above guidelines, with parameters of clinical symptoms and respiratory function [3]. We analyzed the FeNO levels and spirometry test results taken every 10 months, presence or absence of inhaled corticosteroid (ICS) use, and the number of acute exacerbations every 10 months, taken up to September 2017. Children whose FeNO tests could not be taken twice consecutively were excluded from the study.
Data collection
We obtained data on course, treatment details and test results retrospectively from electronic charts. Acute exacerbation of bronchial asthma was defined as attacks severer than moderate attacks that required systemic corticosteroid therapy. Diagnosis of complicating allergic rhinitis was defined by the regular prescription of antihistamine or steroid nose drops. Serum IgE levels of class 2 or greater against house dust mite (HDM) by radioallergosorbent test was defined as sensitizing to HDM.
Nitric oxide measurement and spirometry
FeNO was measured using NIOX MINO device (Aerocrine, Solna, Sweden), according to standardized guidelines [4] and expressed in parts per billion (ppb). FENO levels ≥ 21 bbp were defined as high, following the American Thoracic Society guidelines [5]. FENO testing was performed before spirometry. Spirometry was measured using DISCOM-21 FXIII (Chest, Tokyo, Japan). Spirometric parameters including forced expiratory volume in 1 second (FEV1) and maximum flow at 50% of forced vital capacity (V50) were expressed as a percentage of normal predicted values.
Statistical analysis
Statistical analysis was carried out with JMP 9.0.0 software (SAS Institute Inc., Cary, NC, USA). Student t test was used to compare values between the 2 groups, and Fisher exact test was used to compare proportions between the 2 groups. A difference was considered significant with p < 0.05.
This study was approved by the Ethics committee of Haga Red Cross Hospital and was performed with consideration of all appropriate ethical issues.
RESULTS
Clinical characteristics
Of the 140 children aged 7 years and older who underwent FeNO during the testing period, those who could not undergo the FeNO taken every 10 months twice consecutively were excluded, leaving 116 remaining children as subjects of analysis. Children with initial FeNO levels ≥ 21 ppb were assigned to the high FeNO group and those with <20 ppb were assigned to the normal FeNO group, each including 48 (33 boys) and 68 (46 boys) children, respectively. The high FeNO group had higher age at the initial FeNO test, but there were no differences in age (in months) at bronchial asthma diagnosis, number of acute exacerbations of bronchial asthma in the year preceding the initial FeNO test, or details of medications used in long-term control of bronchial asthma at the initial FeNO test (Table 1). The high FeNO group had more children complicated with allergic rhinitis, higher peripheral eosinophil ratios, and HDM sensitization. Respiratory function tests were performed on 83 children (72%) at the time of the initial FeNO test, which revealed that there was no difference between the high and normal FeNO groups in terms of %FEV1 and %V50, and the means of all measured values for both groups were within normal ranges. The mean observation period for the high and normal FeNO groups was 25.8 ± 0.7 and 24.7 ± 0.6 months, respectively.
Table 1
Clinical characteristics

Values are presented as mean ± standard deviation or number (%).
FeNO, fractional exhaled nitric oxide; ICS, inhaled corticosteroid; LTRA, leukotriene receptor antagonists; LABA, long-acting beta-agonist; WBC, white blood cell; HDM, house dust mite; FEV1, forced expiratory volume in 1 second; V50, maximum flow at 50% of forced vital capacity.
*p < 0.05.
FeNO levels and spirometry parameters during 30-month periods
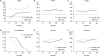
Forty-two children in the high FeNO group and 41 children in the normal FeNO group had performed consecutive respiratory function tests. The high FeNO group continued to have high subsequent (mean) FeNO levels of ≥40 ppb (Fig. 1A). The normal FeNO group also exceeded 21 ppb at 10 months and later, but the FeNO level at 30 months was lower than the high FeNO group (normal FeNO group, 30.6 ± 4.5 ppb; high FeNO group, 52.8 ± 5.2 ppb; p = 0.0018). Both the high and normal FeNO group also had %FEV1 and %V50 within the normal ranges during the observation, without a difference (Fig. 1B, C). There was no difference in the number of acute exacerbations between the high and normal FeNO groups, either, and decreased with time (Fig. 1D). There was no difference in the rate of use or dosage of ICS between the high and normal FeNO groups, either (Fig. 1E, F).
Fig. 1
Fractional exhaled nitric oxide (FeNO) levels ≥ 21 bbp were defined as high. A gray line shows the mean value of each parameters at every 10 months in normal FeNO group. A black line shows the mean value of each parameters at every 10 months in high FeNO group. (A) The high FeNO group continued to have high subsequent FeNO levels of ≥40 ppb. The normal FeNO group also exceeded 21 ppb at 10 months and later, but the FeNO level at 30 months was lower than the high FeNO group. (B, C) Both the high and normal FeNO groups also had %FEV1 and %V50 within the normal ranges during the observation, without a difference. (D) There was no difference in the number of acute exacerbations between the high and normal FeNO groups, and decreased with time. (E, F) There was no difference in the rate of use or dosage of inhaled corticosteroid (ICS) between the high and normal FeNO groups. FEV1, forced expiratory volume in 1 second; V50, maximum flow at 50% of forced vital capacity. *p < 0.05.
Spirometry parameters in high FeNO group during 30-month periods
Among the 42 children who had performed respiratory function test in the high FeNO group, 14 children were with %V50 below normal values at the initial FeNO test. Those with low %V50 at the initial FeNO test also had %FEV1 below normal levels, and their %FEV1 and %V50 levels at 30 months were also below normal (Fig. 2A). However, in the normal FeNO group, even if the %V50 at the initial FeNO test was below normal in 13 children, the %FEV1 was within the normal range, and the %FEV1 and %V50 increased after 20 months to maintain the normal range (Fig. 2B). In the high FeNO group, there were no significant differences in sex, age, complications of allergic rhinitis, or peripheral eosinophilic ratio between the groups with below normal and normal %V50 (sex, p = 0.5527; age at testing, p = 0.5874; complication of allergic rhinitis, p = 0.9499; eosinophilic ratio, p = 0.4263), but all cases were HDM-sensitized. In terms of the medication used for long-term control in the high FeNO group, the rate of long-acting beta-agonist (LABA) use in children with below normal %V50 at 20 months (normal %V50 4 of 28 children, low %V50 6 of 13 children) and the ICS dosage at 30 months (normal %V50, 70 ± 30 μg/day; below normal %V50, 210 ± 40 μg/day) were high (Fig. 2A). There was no difference in the frequency of acute exacerbations between children with normal and below normal %V50 (p = 0.3902), but at 30 months, the change in FeNO during the observation period was greater in children with below normal %V50 (10 months normal %V50, 40 ± 6 ppb; low %V50, 44 ± 8 ppb; p = 0.6637; 20 months, 39 ± 4 ppb, 39 ± 6 ppb, p = 0.9581; 30 months, 43 ± 7 ppb, 69 ± 10 ppb, p = 0.0471).
Fig. 2
A gray line shows the mean value of each parameters at every 10 months in normal %V50 group. A black line shows the mean value of each parameters at every 10 months in low %V50 group. (A) Among the children in the high FeNO group, those with %V50 below normal values at the initial FeNO test also had %FEV1 below normal levels, and their %FEV1 and %V50 levels at 30 months were also below normal. In the high FENO group, the rate of LABA use in children with below normal %V50 at 20 months and the ICS dosage at 30 months were high. There was no difference in the frequency of acute exacerbations between children with normal and below normal %V50. (B) In the normal FeNO group, even if the %V50 at the initial FeNO test was below normal, the %FEV1 was within the normal range, and the %FEV1 and %V50 increased after 20 months to maintain the normal range. FeNO, fractional exhaled nitric oxide; FEV1, forced expiratory volume in 1 second; V50, maximum flow at 50% of forced vital capacity; ICS, inhaled corticosteroid; LABA, long-acting beta-agonist. *p < 0.05.

Spirometry parameters according to age at bronchial asthma diagnosis
Although there was no relationship between FeNO levels and spirometry parameters, spirometry parameters differed by age at diagnosis: the children diagnosed with bronchial asthma before 4 years(50 of 111 children, 45%) had lower %FEV1 and %V50 in the observation period compared to children who were diagnosed after age 4 years (Fig. 3). However, for both subgroups, the mean %FEV1 and %V50 during the observation period was within the normal range.
Fig. 3
The children diagnosed with bronchial asthma before 4 years (onset age < 4) had lower %FEV1 and %V50 in the observation period compared to children who were diagnosed after age 4 years (onset age ≥ 4). FEV1, forced expiratory volume in 1 second; V50, maximum flow at 50% of forced vital capacity. *p < 0.05.

DISCUSSION
Although FeNO levels alone was not a viable indicator of acute exacerbations or respiratory function in school-aged children with bronchial asthma, combining it with spirometry successfully predicted the respiratory functions over the subsequent 30-month period.
This study revealed acute exacerbations in 35% of children with bronchial asthma; however, there was no difference in the frequency of acute exacerbations between the high and normal FeNO groups, thus FeNO levels did not function as a marker of acute exacerbations. Although FeNO levels are reported to be an indicator of acute exacerbation of bronchial asthma or lung dysfunction from the way it reflects eosinophilic inflammation of the airway [6, 7], in some studies such as this one, FeNO values and acute exacerbations did not demonstrate a correlation [8, 9]. This is because FeNO levels are not specifically affected by eosinophilic airway inflammation, but also independently affected by the degree of HDM sensitization [10], exposure to inhaled allergens [11], and complications of rhinitis [12] as well. In particular, sensitization to inhaled allergens are often established during the early childhood to school-aged years [13], and children have poorer knowledge of allergen avoidance behaviors and are thus more likely to be exposed to allergens. Therefore, FeNO values in children are more likely to vary since it does not reflect eosinophilic inflammation of the airway alone. The frequency of acute exacerbations obtained in this study is comparable to the frequency of acute exacerbations in children with bronchial asthma from Western countries of 25%–35% [14, 15]. As such, it is unlikely that the absence of significant differences is attributed to acute exacerbation frequency of the studied population.
The children with high FeNO included in this study had high peripheral eosinophilic ratios, high rates of HDM sensitization, and exhibited characteristics of atopic bronchial asthma [16], suggesting that FeNO testing is an effective indicator of atopic bronchial asthma with eosinophilic airway inflammation as the main feature. However, aside from the abovementioned factors that influence FeNO levels (i.e., HDM sensitization, exposure to allergens and complications of allergnic rhinitis), age and height can also affect FeNO [17]. Thus, the fact that the high FeNO group included older children at the time of testing may have been impacted by the factor of age. However, reports on the relationship between FeNO levels and age compared subjects aged 35–44 years to those aged 64 years and older [18], or between subjects aged less than 60 years to those aged 60 years and older [19]: that is, each group covered a wide age range. Reports on children include a study finding no difference in FeNO level by age in children aged 5–16 years [20], and a study that demonstrated no correlation between FeNO level and age in a group of children aged 8–15 years [21], suggesting that it was highly unlikely that the 1-year difference in age was responsible for the difference in FeNO levels.
Lung dysfunction was found in approximately 30% of children with bronchial asthma, but there was no difference between the rates of lung dysfunction in the high and normal FeNO groups, thus FeNO level did not demonstrate efficacy as a marker of lung dysfunction. The proportion of appearance of lung dysfunction in this study matched with the proportion of lung dysfunction in children with long-term stable control and mild to moderate bronchial asthma [22, 23], thus the study population is considered as an average population of bronchial asthma. Lung dysfunction in bronchial asthma is reported to be affected by phenotypes. Phenotypes of bronchial asthma symptoms that prolong since infancy were most highly associated with lung dysfunction [24, 25], thus poor respiratory function of asthmatic children who started to have lung dysfunction in infancy are believed to persist. In this study, children diagnosed with bronchial asthma by age 4 years had worse respiratory functions. Aside from phenotypes, some of the factors of lung dysfunction are the lack of long-term medical control and poor adherence. But in fact, in children with lung dysfunction, long-term control with medication was practiced with higher rates of LABA treatment and higher ICS dosage, step-ups of treatments were attempted, thus suggesting that it was unlikely that lung dysfunction was due to the lack of long-term control with medication. As for adherence, the high FeNO group responded better to ICS. Wide variation in FeNO levels is an indicator of lack of adherence to ICS [26], but in this study, the variation of FeNO levels in children with lung dysfunction were no different from children with normal respiratory function, suggesting the low likelihood that prolonged lung dysfunction was due to poor ICS adherence.
FeNO levels itself is not a marker of respiratory function, but lung dysfunction of children with bronchial asthma with high FeNO levels was prolonged, thus, asthma control combining FeNO testing and pulmonary function testing is believed to be more effective than control with one method. Indeed, higher sputum eosinophil levels were associated with worse respiratory function and the degree of remodeling is severer [27], thus, some types of respiratory function are impacted by eosinophilic airway inflammation. Gelb et al. [28] reported that individuals with FeNO levels ≥ 28 ppb and FEV1 ≤ 76% in a study of adults with bronchial asthma combining FeNO and pulmonary function testing had more acute exacerbations. It has become clear that there are multiple phenotypes underlying bronchial asthma, so it is essential to combine multiple testing methods for the long-term management of bronchial asthma, according to individual conditions.
As a final note, limitations of this study include the fact that FeNO could be conducted on all children in the study, but spirometry could not be conducted correctly in a portion of the children, thus, analysis of pulmonary function testing does not cover all the children in the study. Furthermore, in some cases, the 30-month observation period could not be completed in some children, so the results of analysis on pulmonary function testing at 30 months may reflect a smaller population than before the 30-month mark.
In conclusion, school-aged children with bronchial asthma with high FeNO levels and lung dysfunction are at high risk of prolonged lung dysfunction.
 XML Download
XML Download