

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Allergic rhinitis (AR) affects more than 20% of adults and 40% of children in Thai population, and the prevalence in both subpopulations tends to increase every year [12]. The common symptoms of AR, which include nasal obstruction, rhinorrhea, postnasal drip, itching, sneezing, and cough, can significantly impair patient quality of life (QoL) [3]. Based on Allergic Rhinitis and Its Impact on Asthma (ARIA) classification, most AR patients (71%) were in the persistent group, and 84.7% of those had moderate to severe symptoms that adversely impacted their lives in ways similar to those experienced by asthma patients [4].
Patient reported outcome measurement is now frequently used in both research and routine clinical practice [56]. The QoL evaluation instrument that is now commonly used to evaluate AR and allergic rhinoconjunctivitis in Thai population is the Rhinoconjunctivitis Quality of Life (Rcq-36) questionnaire [7]. There are 36 questions that cover 6 domains, and 2 independent items. In clinical practice, the magnitude of change in the patient QoL score and the degree of change in the symptoms score are of equal importance in the management of AR.
Minimal clinically important difference (MCID) is defined as the smallest difference in a domain of interest score that reflects a patient's perception that their symptoms and the results of treatment have improved from a treatment regimen that is both cost-effective and free from side effects [8910]. A 7-point Global Clinical Rating Scale (GCRS) was used to estimate the MCID of QoL in allergic patients [11]. The aim of this study was to determine the MCID in AR in Thai population. Determination of the MCID in AR will be useful for patient evaluation and as a guide for patient management.
MATERIALS AND METHODS
This prospective study was conducted at the Division of Rhinology and Allergy, Department of Otorhinolaryngology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand during the September 2011 to February 2012 study period. Siriraj Hospital is Thailand's tertiary referral center. AR patients aged ≥18 years who attended our outpatient allergy clinic were consecutively recruited. All subjects had symptoms, signs, and physical examination results that corresponded with AR. AR diagnosis was confirmed by positive skin prick test (SPT) result. Patients unable to tolerate SPT, or who were diagnosed with sinusitis, nasal polyp, or severe deviated nasal septum were excluded. The protocol for this study was approved by the Siriraj Institutional Review Board (SIRB) (COA No. Si 683/2011). This study complied with the principles set forth in the Declaration of Helsinki (1964) and all of its subsequent amendments, and written informed consent was obtained from all participants.
Subjects were evaluated during 2 visits that were scheduled 4 weeks apart. Patients were requested to discontinue all AR-related medications for 1 week prior to the first visit. During the baseline visit, patients were asked to complete the Rhinoconjunctivitis Quality of Life (Rcq-36) questionnaire [7] for evaluation of patient QoL. Treatment for AR was then prescribed according to ARIA guidelines. During the second visit, the Rcq-36 questionnaire was completed again, and the GCRS was completed to assess change in symptoms and QoL.
The Rcq-36 questionnaire [7] contains 36 questions that cover 6 domains, and 2 independent items. The 6 domains and the number of questions per domain are listed, as follows: rhinitis symptoms (4 questions), eye symptoms (4 questions), learning or work problems (3 questions), sleep problems (3 questions), social problems (3 questions), and emotional function (5 questions). The 2 independent items inquire about overall health and number of days absent from normal daily activities (e.g., work) due to AR symptoms.
The Global Rating of Change Scale (GRCS) questionnaire [1112] consists of four global questions, and it is used to evaluate whether a patient has improved or deteriorated. The 4 questions are: “Since your last visit, has there been any change in 1. activity limitation, 2. symptoms, 3. emotions, and 4. overall QoL relative to your AR? If they indicated that there had been no change, they were given a zero score. Change scores were, as follows: -7 = a very great deal worse; -6 = a great deal worse; -5 = a good deal worse; -4 = moderately worse; -3 = somewhat worse; -2 = a little worse; -1 = almost the same/hardly any worse at all; 0 = no change; 1 = almost the same/hardly any better at all; 2 = a little better; 3 = somewhat better; 4 = moderately better; 5 = a good deal better; 6 = a great deal better; and, 7 = a very great deal better
The MCID was determined using an anchor-based method [11] that was based on the GRCS change, either improve or deteriorate, for 2 and 3 scale. The MCID from each domain was calculated. The overall QoL was also calculated from the sum of all 6 domains. The MCID from the distribution-based method was calculated using standard deviations that ranged from 0.5 to 2.0 [11].
Patient demographic, clinical, and QoL characteristics were summarized using descriptive statistics. Categorical data are presented as number or number and percentage, and continuous data are presented as mean ± standard deviation. All statistical analyses were performed using PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Eighty-four AR patients were consecutively enrolled in this study. Of those, 79 patients completed the study and were included in the final analysis. A flow diagram describing the study recruitment protocol is shown in Fig. 1. The mean age of the 79 analyzed patients was 36.0 ± 15.2 years. Most patients (71 of 79, 89.9%) were sensitized to both indoor and outdoor allergens. The baseline overall QoL score, as measured by Rcq-36, was 2.13 ± 0.69. The mean QoL score for each Rcq36 domain is shown in Table 1.
Fig. 1
Flow chart describing the study recruitment process. Rcq-36, Rhinoconjunctivitis Quality of Life; INCS, intranasal corticosteroid.

Table 1
Patient demographic, clinical, and quality of life characteristics (n = 79)

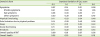
After standard treatment for 4 weeks according to the ARIA guideline, the mean change in overall QoL was 0.21 ± 0.57 from the anchor-based method [11]. The MCID for each domain from the anchor-based method was estimated, and the results are shown in Table 2.
Table 2
Changes in quality of life scores from global rating of change (anchor-based method)

For MCID calculation by the distribution-based method [11], standard deviations (SD) of QoL ranging from 0.5 to 2.0 SD were calculated for overall QoL and for each domain. The MCID for the standard deviation of 1.5 and 2.0 was 0.27 and 0.36, respectively (Table 3).
Table 3
Changes in quality of life scores (distribution-based method)
DISCUSSION
The results of this study revealed an MCID for overall QoL of 0.21 ± 0.57 from the anchor-based method, and of 0.27 from the distribution-based method. MCID estimate recommendations should be based on multiple approaches [13]. In this study, we selected a distribution-based approach based on standard deviation criteria as the comparable method. Using a standard deviation of 1.5, which was calculated from pooled data, the values of both methods were found to be sufficiently similar [11].
A recent study from Devillier et al. [12] recommended the “2-point change of GCRS” for determining the MCID. The global rating change of 2–3 levels serves as an‘anchor’ for changes in QoL. We propose the use of 0.21 units as the MCID for overall QoL from the anchor-based method, because it complies with the definition of ‘minimal clinically important difference’. When we compared the 0.21 MCID value from the anchor-based method to the 0.27 MCID value from the distribution-based method using an SD of 1.5, we found them to be comparable.
The MCID of 0.21 units for overall QoL in AR identified in the present study is different from the MCID of 0.5 units (range, 0.42–0.58 units) for QoL in asthma that was reported by Juniper et al. [10]. From the study by Barnes et al. [11] in AR population, the MCID on the Mini Rhinoconjunctivitis Quality of Life Questionnaire was 0.4 units. Our study revealed an MCID for the rhinitis symptoms domain of 0.42 ± 0.72, which was comparable with the MCIDs reported by Barnes et al. [11] and Juniper et al. [10].
Among the MCIDs calculated for the 6 domains of the Rcq-36, the MCIDs for physical functioning (0.09) and role limitation (0.11) are lower than the MCIDs for rhinitis symptoms and emotional function (both 0.42). This finding can be explained by the nature of AR, which is associated with less physical activity limitation than other diseases, such as asthma. But the symptoms of AR can adversely affect patient emotions, which are supported by the fact that the rhinitis symptoms and emotion domains both had an MCID of 0.42.
A limitation of this study is the wide range of standard deviations of MCID, which suggests an insufficiently large study population. Another limitation is the source from which the study population was recruited. Our center is a large urban tertiary care hospital, which means that the QoL of AR patients at our center may differ from the QoL of AR patients in primary healthcare settings. But the MCID is the determination of ‘change’ that the results can be applied to the clinical response in the general practice as well. An established MCID for QoL can be applied to patients in all age groups [5]. Studies designed to investigate or compare AR treatments can use the MCID from this study to calculate the sample size in future clinical trials.
In conclusion, the MCID for overall QoL was estimated to be 0.21 ± 0.57, and the MCID for rhinitis symptoms was estimated to be 0.42 ± 0.72 in Thai patients with AR. These values can be used for clinically meaningful measurement, and to compare the efficacy of AR treatment modalities. These values can also be used to evaluate and compare the cost-effectiveness of AR treatments.
 XML Download
XML Download