

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of allergic diseases has been increasing over time in many countries [1]. In Tokyo, the prevalence of wheeze and asthma among children aged 5 years was reported to be 16.5% and 9.6%, respectively [2]. The ‘hygiene hypothesis’ is thought to be one of the reasons for an increasing trend in allergic diseases [3], reflecting a modern western lifestyle and a lack of exposure to microorganisms that could explain the allergy epidemic observed after the Second World War [4]. Recently, this hygiene hypothesis has been considered from the aspect of exposure to antimicrobial agents and preservatives such as paraben (Pb) and triclosan (TCS) [5]. Pb and TCS are included in many daily consumer products [6], with Pb present in around 40% of rinse-off personal care and 60% of leave-on products [7]. Common Pbs include methylparaben, ethylparaben, propylparaben, and butylparaben. Often more than one Pb is included in a single product. Although TCS had been widely used in personal care products such as toothpaste, cosmetics, soap, and toys, in September 2016 the Japanese government proposed that alternatives to TCS should be used in soaps following a ban on consumer antiseptic wash products containing TCS by the U.S. Food and Drug Administration.
A cross-sectional study in the United States (US) demonstrated that Pb and TCS exposure was associated with allergic sensitization in children [8]. Another study on children in Norway found that higher concentrations of TCS in urine were associated with allergic sensitization and allergic rhinitis [9]. However, no reports have investigated the relationship between Pb and TCS exposure and allergies in Japan. Therefore, the aim of this study was to examine exposure to Pb and TCS among Japanese individuals with allergic diseases.
MATERIALS AND METHODS
Study design
We conducted a cross-sectional study in the National Center for Child Health and Development (NCCHD) in Japan between October 2016 and April 2017. We recruited 160 children (80 allergic and 80 nonallergic) and 80 adults (40 allergic and 40 nonallergic) from patients visiting the NCCHD, hospital staff, and their families. Because this was an exploratory pilot study, we did not carry out sample size determination. This study was approved by the Clinical Research Ethics Committee of NCCHD (approval number: 1263). Written informed consent was obtained from adults and parents of children. We also obtained informed assent if participants were under 20 years of age.
Outcome assessment
The history of current atopic dermatitis (AD), allergic rhinitis, and wheezing was assessed based on the International Study of Asthma and Allergies in Childhood questionnaire [10] translated into Japanese. Bronchial asthma (BA) was determined by a positive answer of a following question: “Has your child had asthma in the chest in the past 12 months?”. Allergy was defined as having at least one allergic disease.
Exposure assessment
Participants and their caregivers examined all daily commodities used, such as shampoo, toothpaste, body wash, and ointment, determine the frequency at which the commodities were used, and identified whether Pb and TCS were contained in the daily commodities used during the past 3 days. This information was added to the questionnaire. Study staff checked whether each item included Pb and/or TCS using company information about the product. Spot early morning urine samples were collected, and the urinary creatinine concentration (mg/dL) was determined by SRL Inc. (Tokyo, Japan). Urine concentrations of Pb and TCS were measured by liquid chromatography–tandem mass spectrometry at Shin Nippon Biomedical Laboratories, Ltd. (Wakayama, Japan). The limits of detection (LOD) were 1 ng/mL for BP and TCS, and the range of detection was 1–100 ng/mL.
Statistical analysis
Data were analyzed without missing values. The association between current allergic diseases and the use of Pb/TCS-containing daily commodities or the urinary total Pb/TCS concentration was analyzed by the chi-square test or univariable logistic regression. Multivariable logistic regression was performed by including current allergic diseases and age category (0–1, 2–12, 13–18, and ≥19 years old) as the fixed effect. Bayesian multivariable logistic regression was performed using Markov Chain Monte Carlo simulation to estimate the posterior probability of the adjusted odds ratio (OR) and to calculate the probability higher than each preset OR threshold: 1.0, 1.5, and 2.0. Vague priors were set for the intercept and fixed effects using a normal distribution with a mean of 0 and a variance of 10,000, and posterior distribution samples were generated by simulation with 20,000 iterations, 2,000 burn-ins, and 5 thinnings.
We also focused on the subgroup aged under 15 years (representing the age of compulsory education in Japan). Univariable and multivariable logistic regression of the subgroup analysis set were performed as for in the overall analysis set. The comparison of the urinary Pb/TCS concentration distribution which was transformed to ln (1+ [urinary Pb/TCS concentration]) was analyzed by the Wilcoxon rank sum test. p values under 0.05 were defined as statistically significant. All statistical analyses were performed with SAS ver. 9.4 software (SAS Institute Inc., Tokyo, Japan) and EZR ver.3.4.1 (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
We asked 240 candidates for participating in the present study. A total of 229 participants agreed with participating in the study. Of these, 6 were not included in the analysis; 5 were missing values for urine Pb and TCS concentrations and 1 had a missing value for a question about AD. Therefore, 223 participants were analyzed. Characteristics of the study population are shown in Table 1. A total of 117 children (84.8%) aged ≤ 15 years used Pb-containing daily commodities. Methylparaben and ethylparaben were detected in the samples, but other Pbs were under the LODs. The sum of methylparaben and ethyl concentrations was calculated as the creatinine corrected total Pb (pmol/Cr). The mean urinary Pb concentration in children ≤15 years was 8.3 pmol/Cr (range, 0–41,150.9 pmol/Cr). The number of children ≤15 years who used TCS-containing daily commodities was 14 (11.1%). However, urinary TCS concentrations were under the LOD. Regarding individuals without allergy, those aged ≤15 years showed higher Pb concentrations than those aged ≥16 years (Fig. 1).
Table 1
Clinical characteristics of the study population
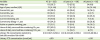
Fig. 1
Comparision of urinary paraben (Pb) concentrations among participants without allergy (≤15 years vs. ≥16 years).
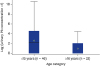
Table 2 shows the results of logistic regression analysis of current allergic diseases according to Pb and TCS use among children aged ≤15 years. Pb use was significantly positively associated with current AD (adjusted OR, 4.61; 95% confidence interval [CI], 1.23–17.3). We could not examine the relationship between Pb use and BA because no participants with BA had been exposed to Pb. Regarding the association of current allergy with Pb use, the posterior probability of OR > 1.0 was 0.968, >1.5 was 0.790, and >2.0 was 0.538 (Table 3).
Table 2
Logistic regression analysis of allergic diseases and Pb and TCS user ≤15 years

Table 3
Results of posterior distribution of Bayesian logistic regression for current allergy using daily commodities with Paraben

In the case of participants without allergies, participants aged ≤15 years using Pb-containing daily commodities tended to have significantly higher urine concentrations of Pb (p < 0.001) (Fig. 2). Although not significant, participants with current allergies tended to show higher urine concentrations of Pb compared with those without current allergies (Fig. 3). In participants ≤15 years old, urinary Pb concentrations were significantly increased in those with current AD (median, 4.58 vs. 0, respectively; p < 0.0001), and showed an increased tendency in those with current wheeze (median, 3.45 vs. 1.82, respectively; p = 0.0535) compared with participants without current AD or current wheeze (Fig. 4). Urinary TCS concentrations in patients with and without allergic disease could not be compared because they were below the LOD.



DISCUSSION
To the best of our knowledge, this is the first study of actual Pb and TCS exposure in the Japanese population, and the first suggestion that Pb exposure is associated with current AD. This study also revealed the high exposure of Japanese children to Pb, while urinary TCS concentrations of all children were below the LOD. A major strength of this study was that we could obtain detailed information about daily commodities and that we could evaluate urine Pb and TCS concentrations.
In the case of Pb exposure, our study showed that children were more exposed to Pb compared with adults. This contrasts with the findings of a US study which observed higher concentrations of Pb in the urine of adults compared with children [11]. This difference could be explained by the fact that the NCCHD previously reported the findings of a randomized controlled study [12] suggesting that using moisturizing skincare on babies prevented AD development. Therefore, the general public in the vicinity of the NCCHD may have used skin moisturizers even though they did not have allergic diseases.
Recently, an earlier study showed an association of Pb exposure with nonatopic wheeze and allergy sensitization [813]. Pb exposure was shown to be linked with emergency department visits among US asthmatic boys [14]. Overgaard et al. [15] reported that children with AD and using emollient increased urinary concentration of Pb. Dodge et al. [16] also indicated that high level of urinary Pb was contributed by Pb-containing medications. The present study also found that Pb exposure was associated with AD in children. Our study results support these findings. The children with AD in our study might be exposed by emollient and topical steroids as well. On the other hand, a post hoc analysis of a prospective birth cohort study did not show the relationship between prenatal Pb exposure and later allergic features in children [17]. Future study is needed to clarify the relationship between Pb exposure and allergy. Nishihama et al. [18] reported that female Japanese university students had negative relationship between Pb exposure and menstrual cycle length, suggesting that Pb exposure might cause negative impact on the reproductive system. We should pay more attention that Pb exposure might be related not only to allergy, but to reproductive system.
As for TCS exposure, urinary TCS was detected in none of the children in our study and only 11% children used daily personal products containing TCS. Urinary TCS was detectable in 74.6% US children [19] and 47% Norway children [9]. This means that Japanese children are less exposure to TCS compared to those in another area. The government regulation for TCS might contribute to reduce TCS exposure in Japan. Past cross-sectional studies demonstrated that TCS exposure was associated with allergic features such as allergic sensitization [8913]. On the other hand, a post hoc analysis of a prospective birth cohort study did not show the relationship between prenatal TCS exposure and later allergic features in children [17]. Our study did not find the evidence for the association of TCS exposure with allergic outcomes as well because of lack of statistical power due to small sample size. The results of the evidence for allergy development by TCS exposure are still controversial. We would like to expect future prospective cohort study to verify these relationships. Our study recently reported that TCS-exposed mite-sensitized mice showed asthma aggravation and the imbalance of gut microbiota, although mite-sensitized mice did not show asthma aggravation [20]. The mechanism of allergy development by TCS exposure might be led by alternation of microbiota.
Our study has some limitations. First, we could not confirm causal relationship, but examined the association since this study is a cross-sectional study. Nevertheless, we are conducting a prospective cohort study for pregnant women and their consequent children in NCCHD to examine the relationship between Pb and TCS exposure and children's allergy. We will validate our study results from the prospective cohort study in the near future. Second, we did not evaluate real dose of exposure by Pb and TCS although urinary concentrations of Pb and TCS were examined. Past studies already reported that urinary Pb and TCS became biomarkers of Pb and TCS exposures in human [1921]. We believe that urinary concentration of Pb and TCs are reliable biomarkers for evaluating these exposures. It is well-known that another chemicals such as phthalate [22], metabolites of diethylhexyl [23] and bisphenol A [24] increased the risk of allergy. We should pay more attention to another chemicals.
In conclusion, children was highly exposed to Pb in daily life and urinary levels of Pb was associated with current AD in children. On the other hand, TCS exposure was not so common among Japanese children. We should pay more attention to Pb and TCS.
 XML Download
XML Download