

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Aging, vascular damage, and arteriolosclerosis make arteries stiffen.1)2) Increases in arterial stiffness contribute to left ventricular hypertrophy, reduced coronary perfusion, and heart failure.2) Notably, information on arterial stiffness is clinically important, because it is an independent predictor of adverse cardiovascular outcomes.1)3) Arterial stiffness can be measured by pulse wave velocity (PWV) that is the most widely used method in research and clinical fields. Brachial-ankle PWV (baPWV) is a simple and convenient method to measure arterial stiffness.4) The value of baPWV has been validated in many clinical studies4)5)6) and meta-analysis.3)
Aging-related structural changes in the arterial wall are associated with a decrease in elastin and an increase in collagen, leading to increased stiffness and decreased distensibility of arteries.7) Increased aortic root size is another feature of aging-related changes in the aorta.2)8) It has been postulated that increased pulsatile stress as well as structural changes in the arterial wall impacts on dilatation of the aortic root by aging.7) A recent study has been attempted to determine the gender difference in aortic geometry. The study showed that aortic distensibility is higher in women than in men in the young age group. Although aging is accompanied by increased aortic stiffness in both genders, the gender difference exists in the rate of stiffness change, with women showing a rapid decline after menopause.9)
The gender-related impact of arterial stiffness on the geometry of the aortic root has not been well studied. This study was performed to investigate the association between baPWV and aortic root size according to gender.
METHODS
Study subjects
This single-center study was performed at Boramae Medical Center (Seoul, Korea). Between May 2013 and June 2014, a total of 296 consecutive subjects without overt cardiovascular disease and in stable medical conditions who underwent both baPWV measurement and transthoracic echocardiography (TTE) on the same day were retrospectively reviewed. Subjects with the following conditions were excluded: (1) left ventricular ejection fraction < 50%, (2) regional wall motion abnormality, (3) significant valvular stenosis or regurgitation more than mild to moderate degree, (4) bicuspid aortic valve, (5) ankle-brachial index < 0.9, (6) non-sinus rhythm, and (7) pericardial effusion. A total of 263 subjects were finally included in the study. The protocol of this study was approved by the Institutional Review Board of Boramae Medical Center (Seoul, Korea). Informed consent was waived due to retrospective study design and routine nature of data collected.
Data collection
Body weight and height were measured in all subjects. Body mass index (BMI) was calculated by the weight divided by the square of the height (kg/m2). Body surface area (BSA) was calculated using the following the Mosteller formula: BSA (m2) = ([height (cm) × weight (kg)]/3600)½. Information on the histories of hypertension, diabetes mellitus, dyslipidemia, and cigarette smoking, and concomitant medications was obtained using a standardized questionnaire. Hypertension, diabetes mellitus and dyslipidemia were defined based on previous diagnosis and medications controlling them. A smoker was defined as someone who smoked within 12 months. The blood levels of hemoglobin, glycated hemoglobin (HbA1c), total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglyceride were measured. Blood samples were collected after at least eight hours of fasting. Estimated glomerular filtration rate (eGFR) was calculated using the following formula: eGFR = 175 × [serum creatinine (mg/dL)]-1.154 × [age (years)]-0.203 ( × 0.742, if woman).
baPWV measurement
The volume-plethysmographic apparatus (VP-1000; Colin Co., Ltd., Komaki, Japan) was used for non-invasive measurement of arterial stiffness. Each baPWV was measured in accordance with the manufacturer's instructions.10) Caffeine, cigarette smoking, and alcohol were not allowed before baPWV measurement on the study day. Each subject rested supine position ≥ 5 minutes in a quiet room. Electrocardiographic electrodes were applied to both wrists, phonocardiographic electrodes were placed on the edge of the sternum to detect heart sounds, and pneumatic cuffs were wrapped on both arms and ankles. PWV was calculated from distance divided by transit time. The distance between sampling points of baPWV was calculated by subject's height. Transit time was calculated from the start of the brachial pulse wave to the start of the ankle pulse wave. The mean of left and right baPWV values was used for the study.
TTE
TTE was performed using commercially available devices (Vivid E9, GE, Vingmed Ultrasound AS, Horten, Norway; or iE 33 xMATRIX Ultrasound, Philips Health care, Andover, MA, USA), with subjects in left lateral decubitus positions. Two-dimensional measurements of the aortic root were made at mid-systole in the parasternal long-axis view at 4 different levels: the diameters of the aortic annulus (AN), sinus of Valsalva (SV), sinotubular junction (STJ), and ascending aorta (AA) were measured perpendicular to the long axis of the aorta (Figure 1). All 4 diameters were indexed to BSA. The degree of aortic regurgitation (AR) was measured by using a color flow Doppler. Valvular regurgitation was diagnosed using Doppler echocardiography. Color flow imaging represented the regurgitant jet proximal to the valve plane during closing. AR was presented as red signals originating from the aortic valve and spread to the left ventricle during diastolic phase. Each imaging was measured at 3 consecutive beats for accuracy. Valvular regurgitation was categorized as absent, minimal, mild, or mild to moderate based on the current guideline's recommendations.11) All examinations were carried out by 2 experienced cardiac sonographer who did not know the value of baPWV. The coefficients of variances (CVs) were calculated to determine the interobserver reliabilities for each aortic measurement. Each CV was 7.6%, 8.4%, 8.3%, and 9.4%, respectively, for AN, SV, STJ and AA in our laboratory.

Statistical analysis
All numeric data are expressed as mean ± standard deviation for continuous variables and percentage for discrete variables. The differences in clinical characteristics, echocardiographic diameters, and baPWV values between men and women were compared using Student's t test for continuous variable and the chi-square test for discrete variables. Univariate associations between baPWV and aortic root diameter were evaluated using Pearson's bivariate correlation analysis. Scatter plots were used to show the association between two continuous parameters. Multiple linear regression analysis was used to assess the independent correlation between each aortic root diameter and baPWV. Age, systolic blood pressure, HbA1c, total cholesterol, eGFR, and the use of vasoactive drugs were controlled in this model as potential confounders. To assess the cutoff value of aortic diameters and baPWV as a predictor of AR, receiver operating characteristic (ROC) curve analysis was used. Multivariable logistic regression analysis was used to assess the independent associations of the presence of AR with aortic root size and baPWV. Age, BMI, hypertension, diabetes mellitus, and eGFR were controlled in this model. Age-matched 61 men and 61 women were selected based on the propensity score, and gender-matched pair analyses were performed. A p value of < 0.05 is used to indicate statistical significance. All statistical tests were performed with SPSS for Windows version 22 (IBM Co., Armonk, NY, USA).
RESULTS
Clinical characteristics of study subjects
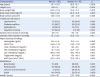
The clinical characteristics of the study subjects are shown in Table 1. There were 187 men and 76 women, ranging in age from 30 to 88 years. Women were older than men (68.5 ± 8.7 years versus 61.1 ± 10.7 years, p < 0.001). The prevalence of hypertension was higher in women, and that of smoking was higher in men. Concomitant medications did not differ between genders. The baPWV values were higher in women than in men (1,717 ± 309 cm/s versus 1,533 ± 311 cm/s, p < 0.001). Table 2 demonstrates the echocardiographic findings of aortic root diameters. The BSA-adjusted diameters of AN, SV, STJ, and AA were higher in women than in men (p < 0.05 for each).
Table 1
Clinical characteristics of study subjects
Data shown are number (%) not otherwise specified.
baPWV: brachial-ankle pulse wave velocity, eGFR: estimated glomerular filtration rate, HDL: high-density lipoprotein, LDL: low-density lipoprotein, RAAS: renin angiotensin aldosterone system.
![]()
Table 2
Aortic root diameters of study subjects

![]()
Association between baPWV and aortic root size
Univariable analyses showed that baPWV was significantly correlated with SV/BSA and STJ/BSA in men, and with SV/BSA, STJ/BSA, and AA/BSA in women (p < 0.05 for each). In men, however, these associations disappeared in multiple linear regression analyses after controlling for potential confounders (p > 0.05 for each). In women, the associations of baPWV with diameters of STJ/BSA (β = 0.407, p < 0.001) and AA/BSA (β = 0.391, p = 0.005) remained significant in the same multivariate models (Table 3). Linear correlations between BSA-adjusted AA diameter and baPWV for men and women are shown in scatter plots (Figure 2). Age, renal function and baPWV were independent factors associated with STJ/BSA in total population (Supplementary Table 1).
Table 3
Associations between brachial-ankle pulse wave velocity and aortic root diameters

Dependent variable was baPWV in each model.
*Age, systolic blood pressure, HbA1c, total cholesterol, estimated glomerular filtration rate, and the use of vasoactive medications were adjusted.
BSA: body surface area.
![]()

Association of AR with baPWV and aortic root size
There were 63 cases of AR; 45 cases (71.4%) of AR with mild degree and 18 cases (28.6%) of AR with mild to moderate degree. AR was observed in 41 men (22.4%) and 22 women (28.9%). SV/BSA, STJ/BSA, and AA/BSA were higher in men with AR than in those without (p < 0.05 for each). The baPWV values were not different according to the presence of AR in men (p = 0.331). All 4 BSA-corrected aortic root diameters and baPWV values were higher in women with AR than those without (p < 0.05 for each). The baPWV values were higher in women with AR than those without (1,831 ± 245 cm/s versus 1,670 ± 323 cm/s, p = 0.040) (Supplementary Table 2). In the ROC curve analysis, the cut-off values of aortic diameters and baPWV for the prediction of AR are shown in Supplementary Table 3. SV/BSA, STJ/BSA, and AA/BSA in men, and all 4 diameters and baPWV in women had cut-off values predicting AR. When these cut-off values were used, AA/BSA was the only factor independently associated with the presence of AR in men in multivariable logistic regression analyses after controlling for potential confounders (odds ratio [OR], 2.81; 95% confidence interval [CI], 1.30-6.04; p = 0.008). In women, all 4 diameters (AN/BSA: OR, 3.11; 95% CI, 1.08-8.93; p = 0.035; SV/BSA: OR, 5.57; 95% CI, 1.90-16.35; p = 0.002; STJ/BSA: OR, 6.12; 95% CI, 2.07-18.10; p = 0.001; AA/BSA: OR, 5.52; 95% CI, 1.89-16.08; p = 0.002) as well as baPWV (OR, 3.20; 95% CI, 1.11-9.20; p = 0.031) were independent predictors of AR in the same multivariable models (Table 4).
Table 4
Independent association of aortic diameters and brachial-ankle pulse wave velocity with aortic regurgitation

Adjusted for age, body mass index, hypertension, diabetes mellitus and estimated glomerular filtration rate.
BSA: body surface area, CI: confidence interval, OR: odds ratio.
![]()
Analyses after gender matching
In age-matched analyses, there were no significant differences in clinical characteristics between genders except lower BSA, lower proportion of smoker and lower hemoglobin levels in women (Supplementary Table 4). Among 4 parameters of aortic root size, STJ/BSA and AA/BSA were independently correlated with baPWV even after controlling of potential confounders in women. There were no correlations between all 4 parameters of aortic root size and baPWV in men in the same multivariable analyses (Supplementary Table 5).
DISCUSSION
This study was designed to investigate the association between arterial stiffness and aortic root size according to gender. The main finding of our study is that increased baPWV was related to increased aortic root size, and the association was more pronounced in women than in men. In addition, increased aortic root diameters and baPWV values were independently correlated with the presence of AR, especially in women.
There have been studies showing a positive correlation between arterial stiffness and aortic luminal size. Kröner et al.12) investigated 40 patients with thoracic aortic aneurysm and showed that normal regional PWV, as assessed by magnetic resonance imaging, is related to the absence of increased diameter, especially in the descending thoracic aorta to the abdominal aorta, suggesting the coupling between increased aortic stiffness and regional aortic dilatation. They also stated similar findings that regional PWV has moderate to high specificity for predicting the absence of regional aortic luminal growth in 21 Marfan patients.13) Koullias et al.14) measured the mechanical characteristics of the aorta using intraoperative echocardiography in 33 patients with ascending aortic aneurysm and compared data from 20 control patients. In that study, they showed that aortic distensibility falls to low levels as aortic root dimension rises.14) Consistent findings showing a correlation between increased aortic stiffness and aortic root dilatation have also been reported in patients with a bicuspid aortic valve,15) tetralogy of Fallot,16) single ventricular circulation,17) and coronary ectasia,18) implicating the important role of arterial stiffness in the development of aortopathy in these specified patients. However, few data are available regarding subjects without documented cardiac and aortic pathology. Vriz et al.19) measured aortic diameter and stiffness in 422 subjects using two-dimensional echocardiography, and demonstrated that the increment in aortic diameter with age is smaller when adjusted for aortic stiffness. This result suggests that there is a significant influence of arterial stiffness on aortic diameter. Milan et al.20) investigated 345 hypertensive subjects and showed that central pulse pressure, PWV, and augmentation index are significantly greater in patients with a dilated proximal AA. In keeping with these findings, our results using baPWV also showed a positive correlation between arterial stiffness and aortic root size in the total study population free of overt cardiovascular disease. Consistent evidence has shown that arterial stiffening is one of the earliest manifestations of vascular aging and usually precedes structural wall changes.21) From a histopathologic viewpoint, aortic media degeneration with breakdown of elastic fibers is related to arterial stiffening and increased blood pressure, finally leading to aortic dilatation.1) Therefore, we can postulate with reasonable confidence that increased arterial stiffness may impact on increases in aortic root size, although a causal relationship could not be assessed in our cross-sectional study. On the other hand, we could not rule out the possibility that the greatest age-related dilatation without a proportional increase in vessel wall thickness occurs in the AA,22) which offsets an increase in PWV, because PWV is directly proportional to the square root of wall thickness and indirectly proportional to the square root of the radius.2) In addition, it should be kept in mind that there is an opposite result demonstrating that reduced aortic diameter is associated with increased aortic pulse pressure or PWV by a mechanism of pressure-flow mismatch.23) Further studies of longitudinal design are needed to elucidate reliable mechanisms on the close relationship between arterial stiffness and aortic geometry.
Our study showed that women had a higher baPWV than men. This finding is in line with those of previous studies showing that age-related increases in arterial stiffness are more pronounced in women than in men.24) Mechanisms underlying gender difference in age-related arterial stiffening is unclear. The mechanisms explaining gender difference may be multi-factorial. However, hormonal status has been considered one of the important contributing factors in arterial stiffness. Tanaka et al.25) showed that postmenopausal women have a higher aortic PWV and a carotid augmentation index than premenopausal women. It has been suggested that estrogen increases prostacyclin production and reduces collagen synthesis by smooth muscle cells of the aorta.26) In addition, estrogen inhibits macrophage infiltration and matrix metalloproteinase production in the aortic wall, which is associated with a low incidence rate of aneurysmal dilatation.27) Notably, hormone replacement therapy in postmenopausal women reduced aortic stiffness as well as aortic size.27) Given that most Korean women go through menopause around the age of 50 years, our enrolled women were mostly postmenopausal. Thus, women had a higher baPWV and a larger aorta than men in our study.
Another important finding in our study is that aortic dilatation and arterial stiffness were associated with AR, especially in women. AR may result from dilatation of the aortic root and annulus as well as malfunction of the valve leaflets.28) It has been reported that aortic root and annular dilatation is the main determinant of increased stress on the aortic leaflet, and may lead to AR despite normal leaflets, shown in experimental study and computer-assisted analysis.29) In regard to the association between arterial stiffness and AR, Grotenhuis et al.30) demonstrated that reduced aortic wall distensibility was related to AR severity in 20 subjects with a bicuspid aortic valve, suggesting the impact of aortic stiffness on the development of AR in this group of subject. However, to the best of our knowledge, there was no data on the association between arterial stiffness and AR, especially in subjects without structural abnormalities of the cardiovascular system. In this context, our result of an independent association between arterial stiffness and AR in women without overt cardiovascular disease is particularly noteworthy. Gender-dependent associations of AR with arterial stiffness and aortic dilatation shown in our study remain to be elucidated.
Our study showed a positive correlation between arterial stiffness and aortic root size, providing pathophysiological evidence on the interplay between functional alterations in aortic skeleton and aortic root geometry. Moreover, the correlation was stronger in women than in men, showing the gender difference in our study. This suggests that the gender effect should be considered and adjusted during interpretation of the results on the association between arterial stiffness and aortic geometry. Furthermore, considering that aortic diameters could be relevant markers of subclinical arterial wall stiffness, aortic diameter measurement through TTE could be a useful tool for diagnosis, risk stratification and evaluation of treatment outcomes.
Limitations
Besides retrospective design, there are several limitations of this study. First, cross-sectional study design did not allow us to prove a causal relationship between arterial stiffness and aortic size. Secondly, not all confounders were adjusted because of a relatively small number of subjects enrolled. Thirdly, our study subjects were middle aged and elderly Koreans without documented cardiovascular disease. This limits generalization of our results to other population groups.
Conclusions
In subjects without documented cardiovascular disorders, increased baPWV is associated with increased aortic root size, supporting evidence for the interplay between functional alterations in aortic skeleton and aortic root geometry. In addition, the association between baPWV and aortic root size is more evident in women than in men. These findings emphasize the role of sex hormone in the interaction between arterial stiffness and aortic morphology, and the gender effect should be considered when we interpret this type of research results. Future longitudinal studies with a larger sample size are required to ascertain our findings.
 XML Download
XML Download