

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Spontaneous echo contrast (SEC) and thrombus in left atrium (LA) as well as left atrial appendage (LAA) detected in transesophageal echocardiography (TEE) were well known risk factors for cardioembolic stroke. Previous report revealed that decreased LAA emptying velocity (<55 cm/s) is an important contributor of thrombus and SEC.1)
There has been increased use of 4-dimensional cardiac computed tomography (4DCT) for the evaluation of valve disease particularly before valve surgery or transcatheter aortic valve replacement (TAVR). In clinical field, 4DCT is utilized to evaluate native and prosthetic valve morphology and function, to measure ascending aorta, aortic root and aortic annulus related with TAVR procedure, and to evaluate subvalvular structures such as papillary muscles and chordae tendinae. In addition, volumetric data of cardiac chambers including LAA can be measured.2)3)
Patients with valve disease are at higher risk of thrombus formation before and after surgery.4)5) Thus, predicting thromboembolic risk and adopting tailored anticoagulation might be important to avoid catastrophic complications in patients undergoing valve surgery. The aim of this study was to investigate the role of 4DCT performed for the evaluation of valve disease before surgery to predict the risk of thrombus formation.
MATERIALS AND METHODS
Patient population and data acquisition
Between March 2010 to March 2015, patients who underwent 4DCT and TEE for cardiac valve evaluation before surgery in Yonsei Cardiovascular Hospital were screened. Inclusion criteria was patients who underwent 4DCT and TEE with LAA velocity measurement within 3 months with maintained normal sinus rhythm during both exams. Exclusion criteria were patients with atrial fibrillation (AF) or flutter rhythm during any of the exam, more than moderate mitral regurgitation, prosthetic valve or intracardiac devices which generate artifact. Among 150 patients who were initially screened, 37 patients with prosthetic heart valve and 51 patients with AF or atrial flutter rhythm were excluded. Finally, 62 patients were included for the analysis in the current study.
Transesophageal echocardiography image acquisition and analysis
Standard TEE views were acquired as per recommendations of the American Society of Echocardiography guidelines using 5 MHz multi-plane probe with commercially available scanners (GE Vivid E9; Vingmed Ultrasound, Horten, Norway, Philips IE33 system; Phillips Medical Systems, Andover, MA, USA).6) LAA was observed at best image between 45 to 90° including 2-dimensional, color Doppler images and pulsed-wave Doppler. Fractional area change (FACTEE) was calculated by dividing maximum area of LAA from the difference between maximum and minimum area of LAA (Figure 1). Peak end-diastolic emptying velocity at LAA in TEE view (VeTEE) was the mean of 3 consecutive values by pulsed-wave Doppler at LAA ostium. SEC was defined as smoke-like swirling pattern observed in LA or LAA after adjustment of optimal gain setting.7)
 | Figure 1Representative image showing measurement of EFCT (A) and FACTEE (B).BP = blood pressure; EF = ejection fraction; EFCT = ejection fraction of left atrial appendage in computed tomography; FAC = fractional area change; FACTEE = fractional area change in transesophageal echocardiography view; LAA, = left atrial appendage; TEE = transesophageal echocardiography; 4DCT = 4-dimensional cardiac computed tomography.
|
Computed tomography image acquisition and analysis
Cardiac computed tomography (CT) scans were performed with a dual-source CT scanner (SOMATOM Definition Flash; Siemens Healthcare, Erlangen, Germany) or a 64-slice multidetector computed tomography (MDCT) (SOMATOM Sensation 64; Siemens Medical Solution, Erlangen, Germany). They were performed with retrospective electrocardiographically gated data acquisition (0–90% phase). The indication of the retrospective gating was to evaluate valvular function as well as coronary patency and adjacent thoracic structures according to the clinician's discretion. Vitrea 6.4 version workstation (Vital Images Inc., Minnetonka, MN, USA) was used for reconstruction and analyzing volume. After selecting LAA orifice at the level of left circumflex artery, LAA was separated from LA, and volume was measured during 10 cycles. Ejection fraction of left atrial appendage in computed tomography (EFCT) was calculated by dividing maximum volume from the difference between maximum and minimum volume (Figure 1).
Statistical analysis
All analyses were conducted using SPSS version 23.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were expressed as mean±standard deviation and were compared using the independent t-test and Pearson correlation coefficient. Variables which were not normally distributed were compared using the Mann-Whitney U test. Categorical variables were compared using the χ2 test or Fisher's exact test, as appropriate. A p value of <0.05 was considered statistically significant. The best cut-off value of EFCT to predict the presence of SEC or thrombus were measured using receiver operator characteristic curve. Correlation between the parameters were also estimated.
RESULTS
Baseline characteristics and transthoracic echocardiography results
Baseline characteristics are compared in SEC/thrombus (+) group and SEC/thrombus (−) group (Table 1). Baseline characteristics were not significantly different between the 2 groups. Transthoracic echocardiography results are shown in Table 2. Left atrial volume index was significantly higher in the SEC/thrombus (+) group when compared to SEC/thrombus (−) group.
Table 1
Baseline characteristics
BP = blood pressure; CAD = coronary artery disease; CKD = chronic kidney disease; CVA = cerebrovascular accident; DM = diabetes mellitus; Hb = hemoglobin; HF = heart failure; HTN = hypertension; NT-ProBNP = N-terminal-prohormone of brain natriuretic peptide; PAD = peripheral artery disease; SEC = spontaneous echo contrast.
![]()
Table 2
Transthoracic echocardiography results

DT = deceleration time; EF = ejection fraction; LAVI = left atrial volume index; LVEDD = left ventricular end-diastolic dimension; LVESD = left ventricular end-systolic dimension; SEC = spontaneous echo contrast.
![]()
Left atrial appendage parameter measurement by 4-dimensional cardiac computed tomography and transesophageal echocardiography
Volumetric assessment of EFCT and functional assessment of VeTEE were significantly lower in SEC/thrombus (+) group. However, 2-dimensional area assessment by FACTEE was not significantly different between 2 groups (Table 3).
Table 3
LAA parameters measured by 4DCT and TEE
CT = computed tomography; EFCT = ejection fraction of left atrial appendage in computed tomography; FACTEE = fractional area change in transesophageal echocardiography view; LAA, = left atrial appendage; SEC = spontaneous echo contrast; TEE = transesophageal echocardiography; VeTEE = emptying velocity at left atrial appendage in transesophageal echocardiography view; 4DCT = 4-dimensional cardiac computed tomography.
![]()
Correlation between parameters
Correlation between EFCT and FACTEE, EFCT and VeTEE were compared. There was no significant correlation between FACTEE and EFCT (r=−0.072, p=0.577). Nevertheless, there was significant correlation between VeTEE and EFCT (r=0.431, p<0.001) (Figure 2). Additional Bland-Altman plot also showed relationship between measurements of EFCT and FACTEE, and measurement of EFCT and VeTEE (Supplementary Figure 1).
 | Figure 2Correlation graph of EFCT and FACTEE (A) and EFCT and VeTEE (B).EFCT = ejection fraction of left atrial appendage in computed tomography; FACTEE = fractional area change in transesophageal echocardiography view; LAA = left atrial appendage; VeTEE = emptying velocity at left atrial appendage in transesophageal echocardiography view.
|
Best cut-off value of ejection fraction of left atrial appendage in computed tomography predicting thromboembolic risk
Best cut-off value of EFCT predicting presence of SEC/thrombus was 37.5% (area under the curve [AUC], 0.654; sensitivity, 0.824; specificity, 0.536; p=0.038), and predicting VeTEE <55 cm/s was also 37.5% (AUC, 0.704; sensitivity, 0.917; specificity, 0.500; p=0.007) by receiver operating curve (Figure 3).
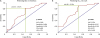 | Figure 3Receiver operator characteristics curve presenting best cut-off value of EFCT predicting SEC or thrombus (A) and VeTEE <55 cm/s (B).AUC = area under the curve; EF= ejection fraction; EFCT = ejection fraction of left atrial appendage in computed tomography; LAA = left atrial appendage; NPV = negative predicative value; PPV = positive predicative value; SEC = spontaneous echo contrast; VeTEE = emptying velocity at left atrial appendage in transesophageal echocardiography view.
|
DISCUSSION
The main findings of this study are as follows: 1) EFCT and VeTEE were significantly lower in SEC/thrombus (+) group. However, FACTEE showed no correlation in regards of the presence of SEC or thrombus. 2) VeTEE was also correlated with EFCT, but FACTEE showed no correlation with EFCT. 3) Best cut-off value of LAA EF by 4DCT predicting thromboembolic risk and LAA peak emptying velocity of <55 cm/s was 37.5%.
Cardiac CT is a useful alternative to TEE for the diagnosis of LAA thrombus. Comparing CT and TEE for the diagnosis of LAA thrombus, the overall sensitivity and specificity were 96% and 92% respectively. Negative predictive value was up to 99%.8)9) Previous studies have shown that MDCT can find potential cardiac sources of cardioembolic stroke including LAA/LA thrombus, aortic atheroma, circulatory stasis and PFO.10)11) However, previous studies with CT acquired delayed image to evaluate LAA thrombus which is not routinely performed in most laboratories.11) The benefit of the current method is that we can apply EFCT in all CT scan with retrospective protocol. Further benefit of EFCT in patients with AF or without valvular heart disease need to be investigated.
TEE has been a gold standard for the detection of cardioembolic source in stroke patients. However, there are several drawbacks to use TEE as a routine practice. First, it is a semi-invasive procedure which produces patient discomfort.10) Patients with neurological dysfunction are more difficult to tolerate the discomfort during procedure. Second, TEE cannot detect extracardiac source of thrombus which is also an important source of embolic stroke.12) Lastly, the ability of TEE for the detection of cardioembolic source is highly dependent by the physician and post-processing is impossible.
TEE has a superiority for temporal resolution than CT, however it can only visualize cross-sectional image of LAA with complex structure.13) Moreover, there is a possibility to measure different cross-section during systole and diastole due to the beating effect. Functional measurements are less affected by beating effect since flow measurement is similar among whole LAA chamber regardless of the measurement site. We consider the most accurate measurement of anatomical EFCT and it is closely related with functional parameters as well as thromboembolic risk.
In our study, LAA EF by 4DCT had benefit for the prediction of SEC or intracardiac thrombus. SEC and intracardiac thrombus are well known risk factors for cardioembolic stroke. It was also correlated with functional parameter of LAA by TEE (LAA emptying velocity <55 cm/s). Best cut-off value predicting SEC or thrombus and emptying velocity <55 cm/s was LAA EF <37.5%.
4DCT can provide useful information for the evaluation of a patient with embolic stroke. Its utility for detecting intracardiac thrombus, patent foramen ovale, aortic atheroma, and coronary artery disease was previously reported.10)12)14) By 4DCT, we can also acquire functional information which was previously provided only by TEE. Those parameters are frequently used for thromboembolic risk assessment.
The indication of TAVR has been expanded recently, and increasing number of patients are undergoing CT before surgery or procedures. In virtue of advancement in CT protocols, patients get less radiation and contrast. Although, TEE still stands for gold standard of evaluating thromboembolic risk, 4DCT might have an alternative role which provides excellent spatial resolution and additional functional information.
This study is retrospective cross-sectional single center study with small number of patients which might inherit limitations.
Patients with normal sinus rhythm were only enrolled to fairly compare the ability of LAA EF by 4DCT and LAA FAC by TEE with correlation to thromboembolic risk in this retrospective design study. AF is an important source of thromboembolism, but thromboembolic risk still exists in the patients with normal sinus rhythm undergoing valve surgery or procedures. Future study including AF patients might be an interesting topic.
In the present study, we evaluated composite of SEC and thrombus as study endpoint and outcome data (e.g., embolic stroke or death) was not available. However, both dense SEC and thrombus are strong risk factors for future thromboembolism.15)16)17)18) They are also related with poor clinical outcome and further studies are needed to investigate whether EFCT is related with hard outcomes such as stroke or death. It is worth to mention that how many actual patients would suffer from true thromboembolic events and we are expecting further prospective design study with larger population to evaluate the role of 4DCT predicting actual thromboembolic event.
In conclusion, the patients who undergo 4DCT before surgical correction of valvular heart disease, LAA EF by volume analysis using 4DCT has additional benefit to evaluate future thromboembolic risk.
 XML Download
XML Download