

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Case summary
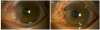
After excision of the pterygium, we measured the size of the defect with reference to the side opposite the defective area and prepared an AM with margins 1.5–2.0 mm greater than the defect size. The AM was first sutured vertically, with reference to the opposite side of the defect. Then we sutured the upper and lower horizontal axes, and positioned the eye, from the front, slightly away from the direction of the opposite side of the defect. The AM was cut by reference to its boundary at the limbus, and three fixation sutures were placed.
Figures and Tables
 | Figure 1Surgical procedures in amniotic membrane (AM) design technique. (A, B) We measured the horizontal and vertical lengths with a caliper. (C) AM was cut to an appropriate size. (D) The AM was positioned on the defect side. (E) Keeping an eye on the opposite side of the defect, the AM was sutured the vertical axis first with 10-0 nylon (arrows). (F) When suturing the upper and lower horizontal axes (arrows), the eye was slightly against the direction of the defect site. (G) The AM was cut according to the boundary at the limbus. (H) Three fixation sutures were added to the transplanted AM (arrowheads). (I) Treatment soft contact lens was applied.
|

References
1. Li M, Zhu M, Yu Y, et al. Comparison of conjunctival autograft transplantation and amniotic membrane transplantation for pterygium: a meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2012; 250:375–381.

2. Zheng K, Cai J, Jhanji V, Chen H. Comparison of pterygium recurrence rates after limbal conjunctival autograft transplantation and other techniques: meta-analysis. Cornea. 2012; 31:1422–1427.

3. Meller D, Pires R, Tseng S. Ex vivo preservation and expansion of human limbal epithelial stem cells on amniotic membrane cultures. Br J Ophthalmol. 2002; 86:463–471.

4. Meller D, Tseng S. Conjunctival epithelial cell differentiation on amniotic membrane. Invest Ophthalmol Vis Sci. 1999; 40:878–886.
5. Ti SE, Tseng SC. Management of primary and recurrent pterygium using amniotic membrane transplantation. Curr Opin Ophthalmol. 2002; 13:204–212.
6. Azuara-Blanco A, Pillai C, Dua HS. Amniotic membrane transplantation for ocular surface reconstruction. Br J Ophthalmol. 1999; 83:399–402.
7. Hwang HS, Kim EC, Kim MS. A new conjunctival free flap design technique for pterygium surgery: stamp technique. Eye Contact Lens. 2016; 42:171–176.
8. Meller D, Tseng SC. Conjunctival epithelial cell differentiation on amniotic membrane. Invest Ophthalmol Vis Sci. 1999; 40:878–886.
9. Kucukerdonmez C, Karalezli A, Akova YA, Borazan M. Amniotic membrane transplantation using fibrin glue in pterygium surgery: a comparative randomised clinical trial. Eye (Lond). 2010; 24:558–566.
 XML Download
XML Download