

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pulmonary embolism (PE) is a rare but dangerous complication of pregnancy and the post-partum period (123). PE is a manifestation of venous thromboembolic (VTE) disease and typically originates from deep venous thrombosis. Since normal pregnancy is accompanied by a state of hypercoagulability and hypofibrinolysis, the overall risk of developing VTE is five-fold greater than that in non-pregnant women, with the highest risk occurring in the post-partum period (45). Unfortunately, the non-specific clinical symptoms of PE such as chest pain and dyspnea mimic certain symptoms of pregnancy, often leaving clinicians unsure of whether to pursue diagnostics.
The American Thoracic Society (ATS) recommends performing bilateral venous compression ultrasound of the lower extremities, followed by further testing if negative. The placement of computed tomography of the pulmonary arteries (CTPA) in the diagnostic algorithm for pregnant patients is currently firmly established; the ATS recommends ventilation/perfusion (V/Q) scanning in case of a normal chest radiography and CTPA in case of an abnormal chest radiography (6). The Australasian Society of Thrombosis and Heamostasis, together with the Councils of the Society of Obstetric Medicine of Australia and New Zealand recommend CTPA when V/Q scanning is not available or non-diagnostic (2). However, all current recommendations are based on limited scientific evidence and lack clear recommendations with regard to the scan protocol (267). This indicates a need for further research regarding PE imaging diagnostics in pregnant women, which is underlined by the variety of CTPA scan protocols and corresponding radiation doses found in the literature for this patient group (68910).
The current trend of individualized diagnostics has led to increasingly patient-tailored CTPA scan protocols, thereby lowering both contrast material (CM) doses and radiation doses to an all-time low (11121314151617). Pregnant patients might benefit most from radiation dose reduction due to the rapid proliferation of tissues in both the fetus and expectant mother (1819).
This study aimed to quantify the differences in radiation dose when applying various CTPA scan protocols on three currently, clinically used CT scanners. Two methods for adapting the scan length were then investigated; a 10% reduction in the caudal scan range and an individually optimized scan range along the z-axis and radiation dose were evaluated. Finally, the technician's decision was evaluated before and after observing the results of this study.
MATERIALS AND METHODS
Study Population and Simulation
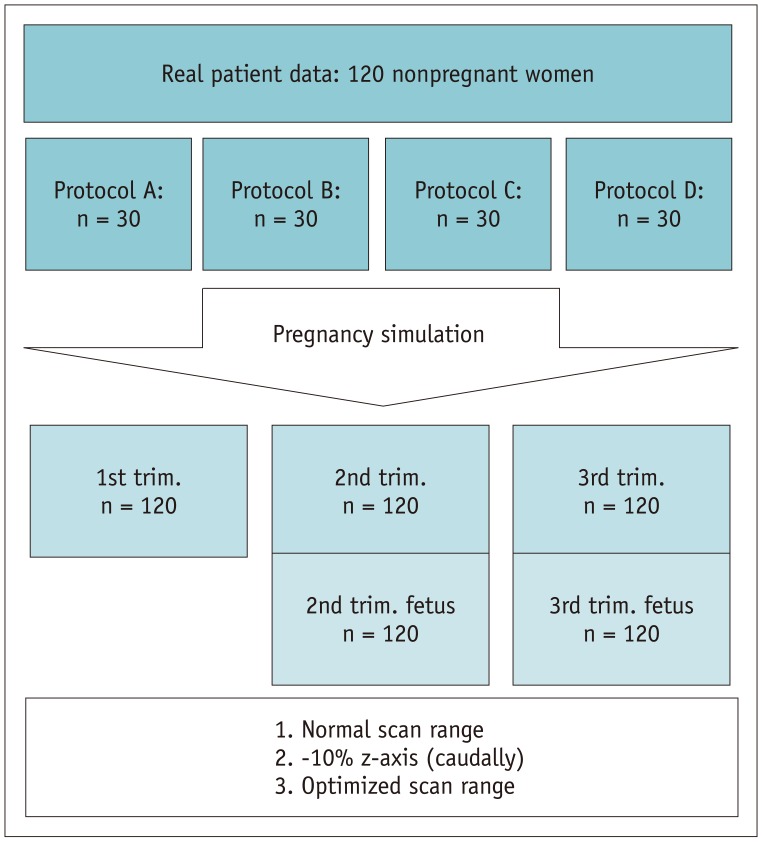
Thirty consecutive female patients undergoing CTPA were included for each of the four scan protocols, resulting in a total of 120 patients being included in this study. The mean patient ages for the four consecutive protocols were 49 ± 20, 63 ± 15, 57 ± 16, and 55 ± 18 years. All patients had a clinical suspicion of PE based on their history and clinical symptoms. A waiver of written informed consent was obtained from the local ethical committee (approval of the local Medical Ethical Review Board [METC] was obtained; waiver reference numer 14-4-158.4). The real patient data were used as the basis for computer-guided phantom simulations, thus assuring that the phantoms would carry the natural variance in body habitus of a real CTPA patient group.
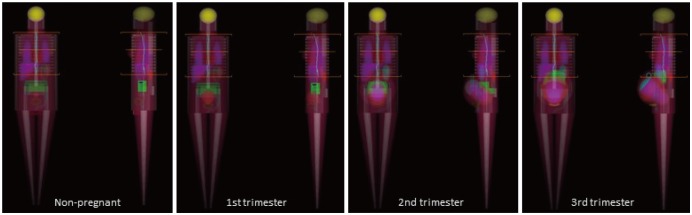
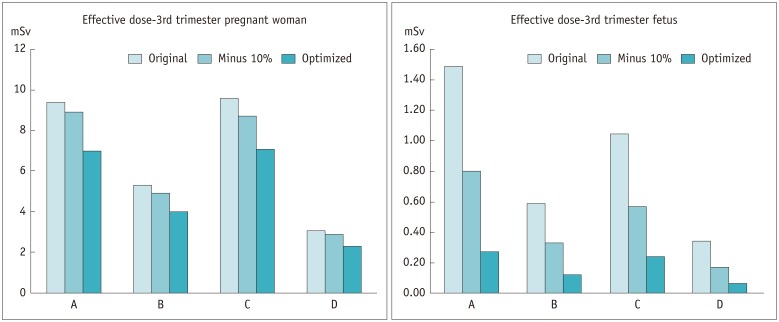
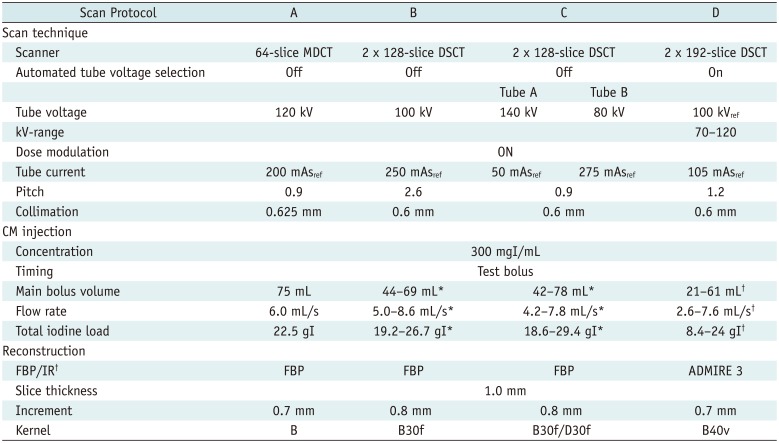
All 120 patients were non-pregnant women; after initial organ dose estimations were performed, the three stages of pregnancy were simulated. This process (described in the next paragraph) resulted in an additional 360 phantom simulations, i.e., n = 120 per pregnancy trimester. For the 2nd and 3rd trimester of pregnancy, fetuses were also simulated in the software; this resulted in 240 phantom fetuses (n = 120 per trimester) in total, for whom the dose estimations are provided, see Figures 1 and 2.
Using a dose monitoring software (Radimetrics™ Enterprise Platform, Bayer Healthcare, Berlin, Germany), the original 120 patients were mapped to mathematical anthropomorphic (Cristy) phantoms based on age, sex, and size, which was determined from the CT scan and scout images (20). This software allows for modification of the patient characteristics and scan parameters such as scan range, sex, and pregnancy status to simulate their effect on organ (equivalent) dose, effective dose, and fetal dose (Fig. 2). The Monte Carlo code employed by the software simulates the X-ray source and radiation transport inside the human body, including scattered radiation (21). The dose monitoring software takes dose modulation along the z-axis into account; however, it does not register angular dose modulation, thereby assuming equal distribution of dose over the slice. None of the scan protocols investigated used angular dose modulation.
Scan and Injection Protocol
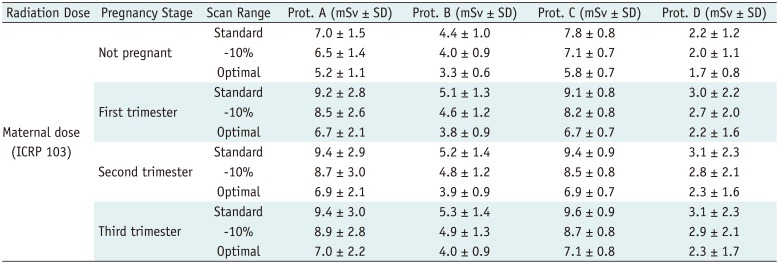
The three CT scanners investigated in this study were a 64-slice multidetector-row CT (MDCT; Brilliance 64, Philips Healthcare, Best, The Netherlands), a 2nd generation dual-source CT (DSCT; SOMATOM, Definition Flash, Siemens Healthineers, Forchheim, Germany), and a 3rd generation DSCT (SOMATOM Force, Siemens Healthineers).
The following four scan protocols were investigated: standard helical acquisition on the 64-slice MDCT (referred to in this text as ‘A’), both a high pitch ‘flash’ helical scan and a dual-energy acquisition (respectively referred to in this text as ‘B’ and ‘C’) on the 2nd generation DSCT, and a high pitch helical scan using patient- and indication-tailored automated tube voltage selection (ATVS; CARE kV, Siemens Healthineers) on the 3rd generation DSCT (referred to in this text as ‘D’).
An overview of all scan parameters of the four protocols is listed in Table 1. All patients were scanned using the breath-hold technique and arm abduction. Careful instructions were given to avoid the Valsalva effect (22). The cranio-caudal scan range was set by the technicians, covering the entire thorax and extending to include the costodiaphragmatic recess, which was identical to a standard thoracic CT scan range.
In all cases, pre-warmed (37℃/99°F) CM was used; iopromide 300 mgI/mL (Bayer Healthcare). In order to determine scan delay, the test bolus technique was applied with a 30 mL saline flush at the same flow rate as the CM. The CM was injected into the left or right antecubital vein using 18–20 G needles and flushed with 40 mL of saline after the main CM bolus (Table 1).
Adaptation of Scan Range
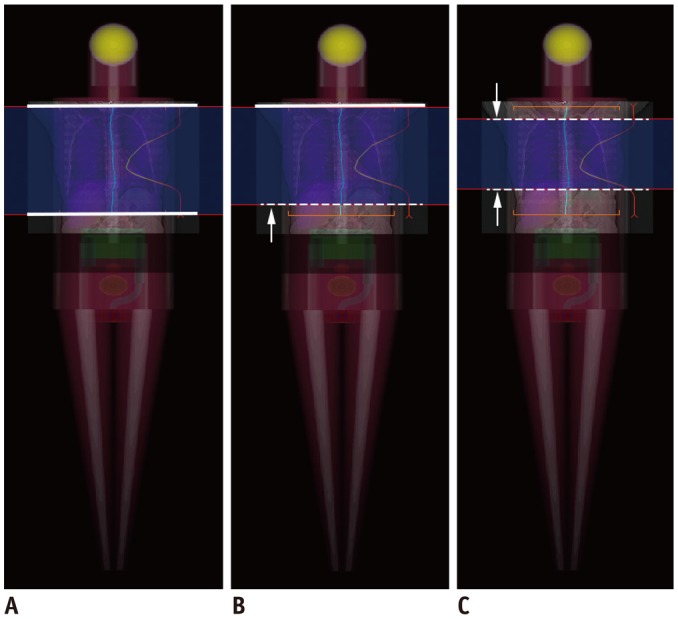
Two methods of reducing z-axis coverage were simulated and investigated. First, the original scan range was reduced by a fixed 10% at the caudal end of the scan. The second method involved optimizing the scan range on a per-patient basis. This was achieved by setting the new scan range from the lung apex to the top of the most caudal diaphragm on the scout image (Fig. 3).
Effective Dose Assessment
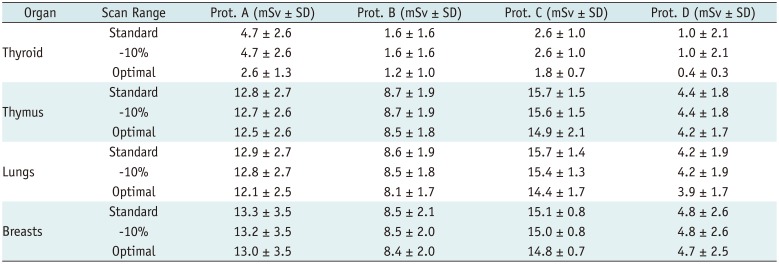
Dose monitoring software was used to determine the effective doses in mSv per scan, calculated according to the International Commission on Radiological Protection, Publication 103 (ICRP 103) (23). Organ-specific (equivalent) doses were assessed for the thymus, thyroid, lungs, and breast tissue in all 120 non-pregnant female simulations. The effective dose and breast tissue equivalent dose were assessed for all stages of pregnancy, and the fetal dose was calculated for the second and third trimester of pregnancy. All assessments were then repeated for both scan range optimization techniques.
Diagnostic Assessment and Image Quality
All 120 original scans were evaluated on a dedicated workstation. An experienced researcher delineated regions of interest in the pulmonary trunk and both pulmonary arteries in order to evaluate the intravascular enhancement. Mean enhancement levels were calculated and values of > 180 HU were considered diagnostic (24). The presence, location, and extent of PE was reported by thoracic radiologists with 4–25 years' experience of reporting CTPA scans. Any incidental findings or alternative diagnoses were reported both before and after adaptation along the z-axis; the latter was performed by noting the top and bottom slice number after adaptation and only reading the slices in between.
Assessment of Clinical Practice
As a second step, eight qualified CT technicians (1–3 years' experience) were asked to set the scan range on 12 scout views of previously scanned pregnant patients as though they were about to perform a CTPA. The technicians were informed of the clinical question — suspected PE — and of the pregnancy status, including the trimester. The scan ranges were noted as the most cranial and most caudal slice. After completion of the dose simulation study, the same technicians were informed of the results of our simulation and asked to repeat the exercise.
Statistical Analysis
Data analysis was conducted using the statistical package for the social sciences (SPSS) version 23.0 (IBM Corp., Armonk, NY, USA). For continuous variables, group means were compared using a one-way analysis of variance (ANOVA) and a post hoc Tukey's test was applied to analyze differences between groups in case of a significant result in the one-way ANOVA. All p values were two-sided and a p value of < 0.05 was considered statistically significant. Continuous values are reported as mean ± standard deviation.
RESULTS
Original Study Population
The patient groups consisted of 30 consecutive non-pregnant women in each protocol. The mean patient age was significantly lower in patients in group A than in those in group B (p = 0.010).
For six patients, there were no data available on body weight (n = 4 in group A and n = 2 in group C). The mean body weight per group was as follows: 81.4 ± 23.9 kg for protocol A, 71.2 ± 13.0 kg for protocol B, 68.8 ± 19.9 kg for protocol C, and 73.7 ± 20.4 kg for protocol D. The mean body weight did not differ significantly between protocol groups (p = 0.104).
Protocol D employed ATVS, which primarily resulted in a kV selection between 70 kV and 90 kV (n = 2 for 120 kV, n = 6 for 90 kV, n = 19 for 80 kV, and n = 3 for 70 kV).
Simulated Dose Assessment and Adaptation of Scan Range
The mean effective doses per protocol for the non-pregnant women using the standard scan range were as follows: 7.0 ± 1.5 mSv for A, 4.4 ± 1.0 mSv for B, 7.8 ± 0.8 mSv for C, and 2.2 ± 1.2 mSv for D (p < 0.01) (Table 2). The thymus, lungs, and breasts all received similar organ doses before and after scan range adaptation, since these remained within the scan range. The doses were highest for protocol C and lowest for protocol D (Table 3).
Effective patient dose increased slightly throughout the pregnancy trimesters for each protocol; the dose increased from the 1st to the 3rd trimester from 2.2% to 5.5%. This effect was also observed for the fetus, but the increase was more significant; the dose increase from the 2nd to the 3rd trimester was 37%, 41%, 40%, and 42% for protocols A, B, C, and D, respectively (Table 4).
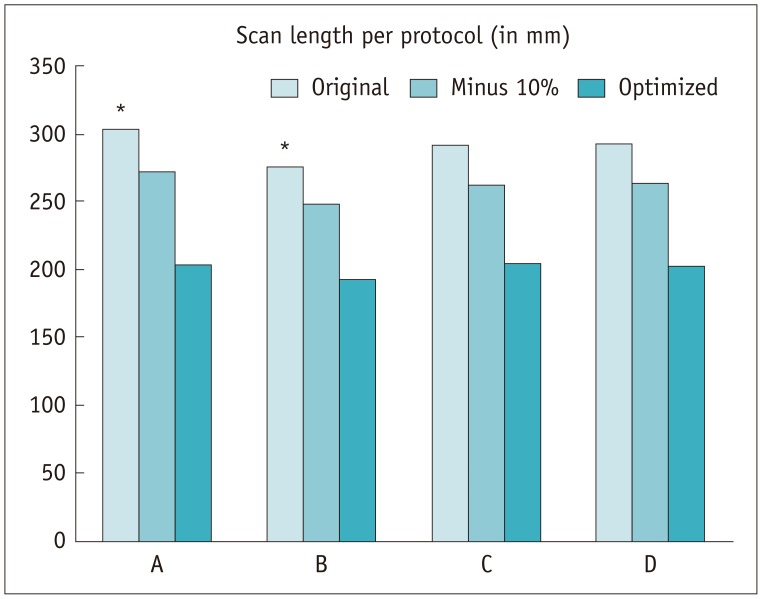
The average scan length before adaptation was comparable for most scan protocols; 303 ± 26 mm for protocol A, 275 ± 36 mm for B, 291 ± 27 mm for C, and 293 ± 32 mm for D, with a significant baseline scan length difference between protocols A and B (p = 0.004). The individually optimized z-axis resulted in a 33%, 30%, 30%, and 31% reduction in the scan ranges for protocols A, B, C, and D, respectively. There was no significant difference in the range reduction between the four protocols (p > 0.438) (Fig. 4).
The individually-optimized scan range was successful in terms of radiation dose reduction (Table 2, Fig. 5). For non-pregnant female phantoms, the effective dose reduction was 26%, 25%, 26%, and 23% for protocols A, B, C, and D, respectively. The overall maternal dose for each of the pregnancy trimesters was reduced by 26–27% for protocols A, C, and D, and by 25–26% for protocol B.
For most of the female adult organs, the individualized scan range resulted in modest mean dose savings: the greatest reduction was 5% for the thymus (protocol C), 8% for the lungs (protocol C), and 2% for breast tissue (protocol A). However, the thyroid gland exhibited more significant dose reductions after z-axis optimization: 45% for protocol A, 25% for protocol B, 31% for protocol C, and 60% for protocol D (Table 3).
The larger caudal reduction of the scan range was paramount in reducing the fetal radiation dose (percentages were similar for the 2nd and 3rd trimesters); 82–83% in protocol A, 80–81% in protocol B, 76–77% in protocol C, and 79–82% in protocol D (Table 4).
Original Datasets Diagnosis and Image Quality
On the original 120 CTPA scans, 19 cases of PE were found (16%); 7 central emboli, 3 lobar emboli, 4 segmental emboli, and 5 cases of exclusively subsegmental PE. None of the PE diagnoses were missed on the CTPA with an optimized scan range; even the exclusively subsegmentally located PE remained visible in these cases. Optimization of the z-axis resulted in four missed incidental findings in the thorax; two cases of missed benign thoracic findings (pulmonary infarction and a small amount of pleural effusion), and two cases of nonspecific pulmonary nodules.
The mean pulmonary enhancement was 335 ± 92 HU for protocol A, 380 ± 107 HU for protocol B, 435 ± 126 HU for protocol C, and 347 ± 73 HU for protocol D. There was a statistically significant difference in attenuation between protocols A and C (p = 0.001) and between protocols C and D (p = 0.006). Two scans were considered non-diagnostic, with mean pulmonary arterial enhancement of < 180 HU, which was likely due to low cardiac output and markedly high body weight; one for protocol A and one for protocol B.
Assessment of Clinical Practice
Initially, the average scan range selected by the technicians was 236 ± 35 mm. After observing the results of the study, the technicians set narrower scan ranges in terms of the z-axis, with an average decrease of 65 ± 40 mm. Interestingly, the z-axis decrease ranged from -17.0–114 mm, indicating that one technician opted to increase the z-axis after the study.
DISCUSSION
This study clearly demonstrates large variations in the CTPA radiation dose between several CT scanners and scan protocols. In this study, a clear advantage of low kV scanning in terms of patient dose was observed; the addition of iterative reconstruction in protocol D ensured diagnostic image quality throughout all scans. The optimized scan range allowed for a mean scan range reduction of 30–33%, translating into a 23–27% effective dose reduction for pregnant women. The dose savings were comparable for each of the tested protocols, indicating that this is a highly effective technique for reducing the CTPA radiation dose with any scanner or protocol. The large dose reduction estimated for the fetuses (up to 83%) is explained by the increased distance between fetus and the scanner beam, which effectively reduces the overall radiation absorption (2526).
One issue, inherent to helical MDCT scanning, is overranging (27). This occurs when the scan length is automatically extended beyond the planned image boundaries, in order to reconstruct the first and last slices of a helical CT scan (28). The Radimetrics™ software uses the dose-length-product and CT-dose-index (CTDI) or CTDIvol as reported by the scanner, thereby calculating the actual irradiated length and including any dose from overranging in the effective dose estimations. The two DSCTs used in this study were equipped with fast moving collimators that minimize overranging and the associated radiation dose; however, it is known that for MDCTs without sliding collimators, overranging can constitute a significant portion of the total radiation dose. For the 64-slice MDCT system used in this study, overranging was responsible for adding approximately 1 mSv to the total effective dose.
Currently, hospitals function according to the ‘as low as reasonably achievable’ or ALARA principle, aiming to make the best choices in scan protocol, CM application, image quality, and more. This principle becomes of even greater importance when performing CT on younger patients, due to the greater hypothetical lifetime attributable risk (2930).
In this study, no PE diagnoses would have been missed with an optimized scan length. Even if one would miss a solitary subsegmental clot, the clinical relevance of such PE has yet to be demonstrated and the positive predictive value of CTPA during pregnancy beyond the segmental level remains unclear (31323334). As a general rule, but even more important when imaging pregnant or young patients, radiation dose risks and the need for diagnostic imaging should be weighed in an individual risk assessment (35).
Several studies have been published on decreased scan length in CTPA, proposing rigorous scan length reductions (14–16 cm) (363738). These studies demonstrated a statistically and clinically insignificant number of missed PEs (0–0.8%), which could be taken as an indication that this method is safe for the patients. The current study confirmed this safety in a markedly larger population with a higher prevalence of PE (16%). Additionally, this is the first study to estimate the impact of optimizing the scan length for the fetal dose of CTPA, which remains a topic of concern and debate in current guidelines.
Although several methods for adapting scan length for scanning pregnant patients have been advocated by the previously mentioned study groups, they have not yet been firmly established in the diagnostic routine or been standardized in any guidelines. However, the current study underlines the importance of careful planning and optimizing the scan length for pregnant patients. This proposed technique can be used in combination with other previously described radiation dose reduction methods, such as automated tube current modulation, bismuth breast shields, and lower kV settings (3539).
Our study has several limitations. First, although this study used real CTPA datasets, the pregnancy stages and fetuses were simulated using phantom models and Monte Carlo code. The reported effective doses and dose savings need to be verified in a real pregnant patient population. Second, this study included several different CM injection protocols. However, the heterogeneity of injection protocols might not impact on the main outcomes of this study, which focused on the radiation dose rather than the CM dose. Additionally, the simulation software did not account for the increased radiation dose uptake in tissues with high iodine uptake, as described by Perisinakis et al. (40). Lastly, the dual-energy scan protocol had not been optimized in terms of radiation dose.
In conclusion, radiologists and technologists alike should be aware of the variations in radiation dose between different scanners and CTPA scan protocols and their impacts on pregnant women. Optimized scan length settings for each patient can result in significant radiation dose savings for pregnant women and their fetuses.

 XML Download
XML Download