

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In congenital heart disease (CHD), the role of cardiothoracic computed tomography (CT) using state-of the-art imaging techniques is evolving rapidly in clinical practice (123). The expanded role of cardiothoracic CT is attributed to the recent technical developments in CT imaging, which are temporal resolution, scan speed, longitudinal coverage, and electrocardiography (ECG)-synchronized data acquisition (4567). It is quite challenging to obtain quality cardiothoracic CT images in children with CHD. This is chiefly because of a wide spectrum of morphologic abnormalities and the resultant hemodynamic complexities that are difficult to predict. Therefore, cardiothoracic CT protocols should be highly individualized to acquire optimal images in these patients. In this regard, a guideline for pediatric cardiothoracic CT imagers would be very helpful to achieve optimized standards. Currently, pertinent specifications and parameters, such as the number of X-ray tube, temporal resolution, longitudinal coverage, and detector configuration, vary among different CT models, and these factors should be considered during the development of a truly practical CT guideline for users. However, the current technical diversity among different CT models at present is not fully incorporated into the existing guidelines (89). Moreover, CT is generally preferred to magnetic resonance imaging (MRI) for evaluating children with CHD in Asian countries; this is mainly due to high costs of MRI, lack of availability, the limitations in human resources, such as dedicated physicists and pediatric anesthesiologist for pediatric cardiac MRI, and a heavy workload of radiologists (10). However, a pediatric cardiothoracic CT guideline considering such regional differences in clinical practice in Asia is currently lacking. Therefore, we developed not only a comprehensive but also vendor-specific guideline for pediatric cardiothoracic CT on the imaging techniques based on as the consensus opinions of the experts in the Asian Society of Cardiovascular Imaging; the guideline includes recommendations for patient preparation, scan techniques, radiation dose reduction techniques, intravenous iodinated contrast agent injection protocols, and post-processing techniques. Vendor-neutral and vendor-specific check points are summarized in Tables 1 and 2, respectively.
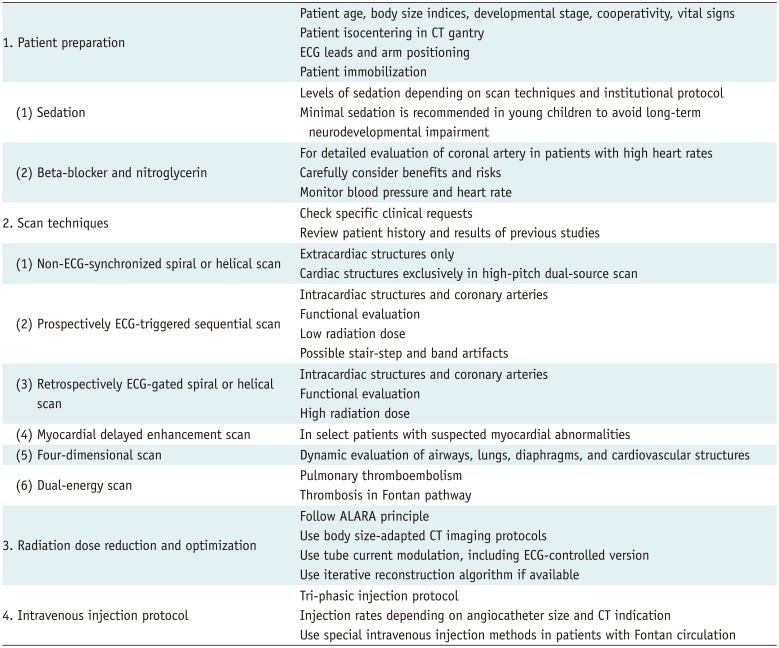
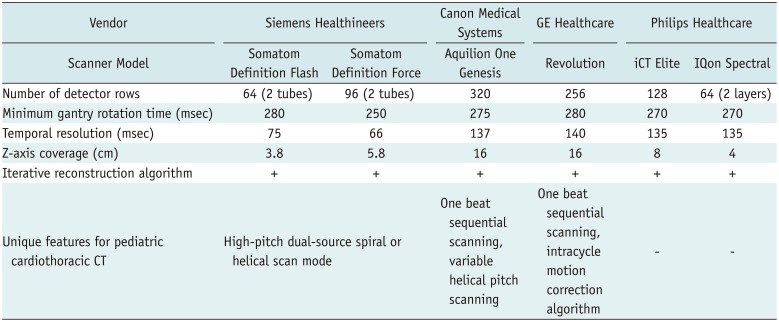
Table 1
Vendor-Neutral Check Points for Optimal Pediatric Cardiothoracic CT
![]()
Table 2
Vendor-Specific Features for Pediatric Cardiothoracic CT
![]()
Go to : 
Patient Preparation
Careful patient preparation is a prerequisite for successful performance of pediatric cardiothoracic CT. Detailed pre-procedural patient assessment including age, body size indices, developmental stage, cooperativity, vital signs, oxygen saturation, renal function, and venous accessibility, should be performed by certified medical personnel. Maintenance of body temperature during the examination is also crucial in newborns to support their immature thermoregulation. Patient positioning at the isocenter of the CT gantry is important to avoid image quality degradation and inappropriate high or low radiation exposure, especially when CT scanning is combined with attenuation-based tube current modulation and use of an additional bowtie filter (411). In this respect, radiology technicians should ensure a patient is isocentered by utilizing the laser beams on the scanner. Because a small child is commonly positioned below the isocenter even at the highest CT table position (12), an additional patient pad or a vacuum device may be necessary to lift the child further up to the isocenter; on this occasion, it is desirable to be radiolucent in order to avoid artifacts (13). Radiopaque ECG leads for ECG-synchronized CT should be placed outside the scan range (e.g., on the arms and upper abdomen) to avoid artifacts (1214). Of note, radiolucent ECG lead sets made of carbon may be used to reduce the artifacts from radiopaque ECG leads (1115). It is better to secure both arms above the head because the position is ideal for the optimization of image quality and radiation dose (1316). Because horizontal position tends to cause severe artifacts (13), the arm position in a sleeping child should be meticulously changed to other positions when possible. Patient immobilization is important not only to reduce motion artifacts but also to reduce the depth of sedation in young children. A vacuum device is helpful for this purpose (11); however, if such a device is not available, a blanket with bands may be used as an alternative.
Sedation
A pediatric radiologist, a cardiologist, or an anesthesiologist may be involved in patient sedation for pediatric cardiothoracic CT based on the policies at each institution. Special caution should be exercised in sedating children with CHD, because they often have the American Society of Anesthesiologists physical status of class III or greater, which is associated with higher occurrence of sedation-related adverse events (17). Levels of sedation are categorized into minimal, moderate, deep sedation, and general anesthesia (17). In contrast to cardiac MRI, which requires a long examination time in the range of 30 minutes to one hour, cardiothoracic CT requires a short examination time less than several minutes; therefore, a lighter level of sedation is generally sufficient for the latter. In addition to the well-known risk of cardiovascular and respiratory complications, long-term neurodevelopmental impairment has recently been recognized to be a potential complication of deeper, repeated, or prolonged sedation in young children (18). It should be emphasized that sufficient levels of sedation necessary for quality pediatric cardiothoracic CT can almost always be achieved without using general anesthesia and endotracheal intubation. Consequently, the minimal level of sedation required for pediatric cardiothoracic CT should be appropriately and individually adjusted, depending on the patient's condition as well as the utilized CT protocol, to avoid these adverse events. In this respect, imagers determining the CT protocol should be actively involved in this important decision-making process to ensure patient safety. Instead of using sedative medications, a feed-and-swaddle technique utilizing oral 25% dextrose solution and a pacifier may be used in neonates and young infants (89); however, this technique is seldom used in Asia. Despite the above general statements, sedation strategies for pediatric cardiothoracic CT often depend on the institutional policies and preferences. After completion of the CT examination, full monitoring should be maintained in a recovery area until the child is awake.
Beta-Blockers and Nitroglycerin
Beta-blockers and nitroglycerin are commonly administered to reduce the heart rate and to dilate coronary arteries, respectively, during coronary CT angiography in adults; both measures contribute in improving image quality (1920). In adolescents whose coronary arteries are the main diagnostic concern, the same medications may be utilized to increase the diagnostic accuracy of CT (2122). On the contrary, coronary CT angiography in young children is usually performed without these medications, and sufficient image quality can still be achieved (4615212324252627). On the other hand, Rigsby et al. (28) reported the initial experience of using beta-blocker and nitroglycerin in 41 children (mean age 6.5 years; range, 2 days–18 years) who had undergone single-source 32-detector-row ECG-gated coronary CT angiography under general anesthesia with intubation and apnea. Despite the use of bi-segment reconstruction to increase the temporal resolution and the heart rate drop of 5–10 beats per minute (bpm) due to apnea and injection of a contrast agent, the target heart rate was achieved in merely 54% of study participants. Although there were no major complications, hypotension occurred in 44% of the patients, bradycardia in 5%, and respiratory distress in 2%. In addition, two intravenous lines were required for administration of medications and a contrast agent (one line for each), and the total examination time, which was approximately 30 minutes, was substantially prolonged in spite of the intravenous administration of an ultra-short-acting beta-locker (esmolol). Patients should be prudently screened for contraindications to each drug. For beta-blockers, the contraindications are severe asthma, allergy, severe aortic stenosis, severe ventricular systolic dysfunction, atrioventricular block, and use of a calcium channel blocker; for nitroglycerin, the contraindications are hypersensitivity, obstructive hypertrophic cardiomyopathy, severe aortic stenosis, systolic hypotension, constrictive pericarditis, and acute right ventricular infarction. During the CT examination while using these mediations, blood pressure and heart rate should be carefully monitored for early detection of adverse events. Considering the procedure-related complexity and the uncertain benefits in improving image quality, the use of beta-blocker and nitroglycerin for pediatric cardiothoracic CT is not highly recommended. It should be kept in mind that these medications should not be used when CT is used to assess the ventricular function and the hemodynamics in cardiovascular structures.
Go to :
Scan Techniques
A variety of scan techniques including non-ECG-synchronized spiral or helical scan, retrospectively ECG-gated spiral or helical scan, prospectively ECG-triggered sequential scan, myocardial delayed enhancement scan, four-dimensional (4D) scan, and dual-energy scan may be used for evaluating children with CHD (Table 1). These scan techniques are generally available in a modern CT scanner. Pediatric cardiothoracic CT should be performed by or under the supervision of an experienced radiologist. Performance of a pediatric cardiac CT examination by a CT technician alone is not recommended because of the complexity of the pathophysiological changes in CHD as well as the diagnostic quality concerns.
Non-ECG-Synchronized Spiral or Helical Scan
Non-ECG-synchronized spiral or helical scan has been commonly utilized for pediatric cardiothoracic CT since the introduction of the slip-ring technology-which enables the use of continuously rotating scan-in 1987. This scan mode chiefly allows the assessment of the extracardiac thoracic vessels, the lungs, and the airways that is still clinically relevant (2930). Hardware advancements in multi-detector row CT scanners with respect to longitudinal coverage and gantry rotation time have increasingly reduced the cardiac and respiratory motion artifacts on pediatric cardiothoracic CT images acquired with this scan mode (5). Moreover, breath-hold scan, which exceedingly improves the image quality, has become possible in a subset of young children. The scan speed is proportional to a pitch value, which is defined as a ratio of table increment per 360° gantry rotation to beam collimation width. It is noteworthy that image quality and radiation dose may or may not be affected by the pitch value depending on the CT scanner used. To obtain a gapless scan dataset for image reconstruction, the upper pitch value is mostly limited to 1.5 for a single-source scan and 3.2 for a dual-source scan (31). In free-breathing young children with CHD, high-pitch dual-source non-ECG-synchronized spiral or helical scan further reduces cardiac and respiratory motion artifacts during cardiothoracic CT (53233). Nonetheless, ECG-synchronized data acquisition is necessary for detailed and accurate assessment of the coronary arteries and the ventricular function.
ECG-Synchronized Scan
ECG-synchronized scan substantially improves the morphologic evaluation of the intracardiac structures, coronary arteries, aortic root, and pulmonary trunk. Appropriate cardiac phase selection is crucial in ensuring acquisition of motionless image quality of pediatric cardiothoracic CT: the mid-diastolic phase at low heart rate and the end-systolic phase at high heart rate. The definition of borderline heart rate, generally in the range of 65–80 bpm, differs among different institutions, and it also depends on temporal resolution of a CT scanner. For the ventricular function assessment, the end-systolic and end-diastolic phases should be obtained. The best cardiac phase is usually determined by visual analysis of the two-dimensional (2D) or three-dimensional (3D) multi-phase datasets or it may be suggested after automatic analysis of a 4D motion map where available (434). In general, the end-systolic, mid-diastolic, and end-diastolic phases are in the ranges of 35–50%, 65–80%, and 90–100%, respectively, of the RR interval. It is noteworthy that the trigger delays may indicate the starting point or the middle point of the acquisition window depending on a vendor. In subjects with arrhythmia, targeting the end-systolic phase with an absolute trigger delay in msec, where possible, is highly recommended to avoid image degradation; alternatively, a wider data acquisition window, in terms of percentage, with ECG editing may be necessary to capture the target cardiac phase at the expense of a higher radiation dose. To certain the proper end-systolic phase, the T wave position may be utilized as a landmark on ECG (456). There are three different ways to acquire ECG-synchronized CT dataset: retrospectively ECG-gated spiral or helical scan, prospectively ECG-triggered sequential scan, and prospectively ECG-triggered high-pitch dual-source spiral or helical scan.
Retrospectively ECG-Gated Spiral or Helical Scan
Before the era of multi-detector row CT, electron-beam CT was used to obtain ECG-synchronized CT images by utilizing prospective ECG triggering (3536). However, electron-beam CT is no longer utilized because retrospectively ECG-gated spiral or helical CT provides excellent image quality, and is widely available (37). The major disadvantage of this scan mode is the high radiation dose resulting from the low pitch values (−0.2). Therefore, imagers involved in pediatric cardiothoracic CT should not only utilize all the available radiation dose reduction techniques including ECG-controlled tube current modulation and minimal scan range. Furthermore, functional evaluation utilizing this scan mode should be judiciously performed in children because it is associated with a high radiation dose. Breath-holding is usually recommended to avoid respiratory motion artifacts in retrospectively ECG-gated spiral or helical scan (4), but this scan mode may be used in free-breathing young children with a slightly high radiation dose and an acceptable image quality (152538).
Prospectively ECG-Triggered Sequential Scan
In this scan mode first proposed in 2006 (39), sequential scans are acquired at a predefined time point in the cardiac cycle with prospective ECG triggering and at consecutive table positions (42638). The low radiation dose achieved by negligibly overlapped data acquisition is regarded to be the major merit of this scan mode (40). In contrast, as the name "step-and-shoot" implies, the prolonged examination time due to the required time intervals for table movement between sequential scans is the major drawback of this scan mode, which often produces "stair-step" misregistration artifacts due to respiration and heart rate variability between adjacent imaging stations. The number of sequential scans is inversely proportional to the longitudinal coverage; for example, a CT scanner with a 16-cm longitudinal coverage can cover the entire scan range in young children in a single sequential scan or one heartbeat (41). Based on many studies in adults (42), it is recommended to use this scan mode in patients with stable and low heart rates (≤ 70 bpm). Because of this recommendation and the concerns about the stair-step artifacts in CT scanners necessitating the use of more than two imaging slabs, this scan mode has been underutilized in free-breathing young children with high heart rates. End-systolic images obtained using this scan mode in children, unlike in adults, have excellent image quality, and the stair-step artifacts are less pronounced due to smaller tidal volumes and smaller time intervals between sequential scans at high heart rates. In addition, a difference in contrast enhancement may occur between adjacent slabs; however, this difference in children is usually trivial and does not substantially affect image interpretation. This scan mode can be used for ventricular function assessment if "padding," which allows for an extended acquisition window in the cardiac cycle, is utilized (434445).
Myocardial Delayed Enhancement Scan
Myocardial lesions with delayed enhancement can be demonstrated during the delayed phase (i.e., between 5 minutes and 15 minutes after intravenous administration of iodinated contrast agent) of ECG-synchronized CT with either retrospective ECG gating or prospective ECG triggering (46). Initial experience with this imaging technique in 29 consecutive children and young adults with suspected coronary artery or myocardial abnormality was recently reported (47). The study showed that sufficiently high contrast-to-noise ratios (10.3–25.4) could be achieved in delayed hyperenhancing myocardial lesions at low tube voltages (70–80 kV) and a shorter delay time (6–8 minutes); in addition, delayed-phase CT findings were equivalent to those of delayed-enhancement MRI in all cases and to those of thallium single-photon emission CT in 70% of the cases. This CT technique can be used as the "one-stop shop" examination in select patients when delayed enhancement cardiac MRI is not possible because of the presence of MRI-incompatible implants or in critically ill patients.
Go to :
Four-Dimensional Scan without ECG Synchronization
4D CT allows acquisitions of multiple consecutive 3D thoracic CT data with the same longitudinal scan range (up to 16 cm) without movement of the CT table. The scan time usually includes at least one respiratory cycle and is in the range of 2.0–4.6 seconds depending on the child's respiratory rate (6484950515253). Although respiratory rates in intubated patients were artificially manipulated in an institution in the United States of America (4852), 4D CT is generally performed during free breathing in most institutions. This scan technique may be used with or without intravenous injection of iodinated contrast agent. Simultaneous evaluation of the cardiovascular structures, the airways, and the lungs is feasible using contrast-enhanced 4D CT. In contrast, non-contrast 4D CT may be added to the cardiac CT protocol in select children.
Go to :
Dual-Energy Scan
Dual-energy scan, which utilizes two X-ray sources with two different energy spectra, was introduced with a first-generation dual-source CT scanner in 2006; other dual-energy scan techniques, including rapid tube voltage switching, use of a dual-layer detector, and use of a twin beam with a split filter, have been introduced since then (54). Initial experience of dual-energy lung perfusion CT in children showed that it is useful for detecting lung perfusion defects caused by pulmonary thromboembolism (55). This scan technique also may be used for evaluating lung ventilation using xenon gas inhalation in children (56). One study (57) demonstrated that 3-minutes delayed dual-energy CT can enhance the detection of silent thrombi in the extracardiac Fontan conduit by utilizing monochromatic 50 keV images. However, it should be noted that dual-energy CT images are acquired with a lower temporal resolution and are susceptible to various artifacts; both of these factors considerably degrade the image quality of the pediatric cardiothoracic CT. Therefore, dual-energy scan should be used as a complementary method in children with CHD.
Go to :
Radiation Dose Reduction and Optimization
In order to comply with the As Low As Reasonably Achievable principle, the radiation dose of pediatric cardiothoracic CT should be strictly optimized and adapted to the body size while maintaining the diagnostic image quality (4558). Body weight is the body size index that is commonly utilized for body size-adapted pediatric cardiothoracic CT protocols. However, the use of cross-sectional dimensions and body attenuation is highly recommended for a better body size adaptation (59). In this regard, a water-equivalent cross-sectional dimension seems to be the single best body size index for this purpose. In contrast, the patient age is not recommended as a body size index because of a broad overlap of body sizes as a function of age in children (60).
Attenuation-based tube current modulation is an essential radiation dose reduction technique, which allows approximately 16% reduction of the tube current without degradation of the image quality (61). Therefore, it should be always used during pediatric cardiothoracic CT examination when available. Imagers should recognize that the basic principles differ among different CT manufacturers (62), and the imagers should also determine the optimal level of image quality unique for each manufacturer (e.g., noise index for General Electric Healthcare, quality reference mAs for Siemens Healthineers, reference image for Philips Healthcare, or standard deviation for Canon Medical Systems) that they wish to achieve. Of interest, a recent study demonstrated that the user-determined level of image quality that was entered before the adjustment of the scan range resulted in an additional 18% reduction in the radiation dose compared with that entered after the adjustment of the scan range (13). As previously mentioned, patient isocentering is of critical importance in ensuring to take full benefits of tube current modulation and to avoid image degradation caused by off-centering. In addition, a suboptimal CT scout image should be repeated after changing the patient position or removing a radiopaque material from the patient to ensure accurate tube current modulation. The radiation dose parameters of a CT scout image also should be minimized to reduce radiation exposure to a patient.
The use of lower tube voltages is beneficial in pediatric cardiothoracic CT, because it produces a higher iodine contrast-to-noise ratio (456). From the radiation dose efficiency point of view, imagers should be careful to avoid tube current saturation at lower tube voltages during cardiothoracic CT using tube current modulation and fast gantry rotation speed (6364). It should be kept in mind that increased image noise at low tube voltage should be adequately compensated for by increasing the tube current.
The scan range of pediatric cardiothoracic CT should be adequately tailored to include anatomical structures of interest only; this is because the radiation dose is proportional to the longitudinal scan range. In the majority of cases, the scan range is similar to or slightly shorter than that of chest CT; the range generally includes the aortic arch superiorly and the bottom of the heart inferiorly. For the assessment of anomalous pulmonary venous connections, major aortopulmonary collateral arteries, or cavopulmonary connections, the lower neck and/or the upper abdomen should be included using a longer scan range as required.
Iterative reconstruction algorithms enabling image noise reduction without substantially affecting the anatomic details are useful in reducing the CT radiation dose, and the image quality is comparable to or better than that of filtered back projection (66566). It is not surprising that CT images reconstructed using these new algorithms are not always favorably ranked by radiologists with different and complex subjective criteria and opinions. In general, newer iterative reconstruction algorithms are better than old ones in terms of image noise reduction as well as preservation of anatomic details, contrast, and sharpness (6768). A lower limit in reducing radiation dose without image degradation or a point of diminishing returns by utilizing an iterative reconstruction algorithm was reported to be present; therefore, the image quality may begin to deteriorate below this limit (6970).
ECG-controlled tube current modulation or ECG pulsing is a useful method to reduce radiation dose for retrospectively ECG-gated spiral or helical scanning (456). Usually, the tube current outside a predefined window in the cardiac cycle can be reduced to 20% of the full tube current. A more aggressive mode of ECG pulsing is available, and ECG pulsing also can be utilized in prospectively ECG-triggered sequential scan in some CT models.
Adaptive collimation technology blocks radiation at both ends of spiral or helical scanning that is not used for image reconstruction. In most modern CT scanners, this function is usually turned on to reduce unnecessary radiation exposure due to z-overranging (671). To reduce radiation exposure to the breasts, an organ-based tube current modulation or a breast shield may be used. A breast shield is limited by the increased image noise in adjacent tissues (72), whereas the breasts may not be included in the reduced dose zone of organ-based tube current modulation (73).
A review of the data on the cumulative pediatric CT radiation dose over 5 years showed that the median value in children with CHD was relatively low (74). Based on the results of a multi-center, multi-vendor study on radiation dose of pediatric cardiothoracic CT, it has been suggested that sex, tube voltage, scan mode, and cardiac function assessment should be considered as essential radiation dose-influencing factors in developing the optimal pediatric cardiac CT protocols (75).
Go to :
Intravenous Injection Protocol
In CHD, all cardiovascular structures, including the left and the right side of the heart and the systemic and pulmonary vessels, need to be sufficiently and evenly visualized on pediatric cardiothoracic CT. Therefore, a tri-phasic injection protocol, in which an undiluted contrast agent is followed by a 30–60% diluted contrast agent and then by a saline chaser, is usually recommended to achieve optimal contrast enhancement and to reduce perivenous streak artifacts (576). If a 5% dilated contrast agent is used instead of saline in the third phase of the tri-phasic protocol, visualization of the thoracic systemic veins may be improved with decreasing perivenous artifacts (5). With regard to the injection site, the leg veins tend to show less perivenous streak artifacts than the arm veins do because the injected contrast agent is mixed gradually with unopacified blood while passing through abdominal visceral veins before arriving in the right atrium. When an arm vein is used, use of the right side can avoid streak artifacts around the left brachiocephalic vein; the streak artifacts are more pronounced and extensive in patients with bilateral superior vena cavae, in which the use of a right arm vein is highly recommended. It is difficult to achieve uniform vascular enhancement in patients with superior or total cavopulmonary connection because of the preferential blood flow and streaming (47778). To obtain optimal vascular enhancement in subjects with superior cavopulmonary connection, leg vein injection with a longer scan delay of approximately 50–60 seconds depending on the patient size is recommended. For imaging of total cavopulmonary connection or Fontan pathway, several injection methods for a single CT scan have been suggested to avoid two repeated (i.e., early and delayed) CT scans: simultaneous injection of an undiluted or a 50% diluted contrast agent through arm and leg veins (4798081); a 3-minutes delayed scanning irrespective of the site of intravenous injection (82); a venous two-phase or split injection method, in which 30–50% of the contrast agent is given and followed by a 30–60 seconds pause and then by the second injection of contrast agent (9); and arm, leg, or dual vein injection with a 60–70-second delayed scanning (7782). The last injection method appears to offer balanced opacification of all thoracic cardiovascular structures and requires a simple injection procedure. However, further comparative studies are needed to determine the best injection method in a patient with Fontan pathway.
With regard to the amount of iodinated contrast agent, 1.5–2.0 mL/kg of body weight is usually sufficient for pediatric cardiothoracic CT. A larger amount of contrast agent may be required in subjects with abundant shunt flow, severe valvular regurgitation, and severely enlarged cardiac chambers (4). In most cases, the use of a power injector is preferred to the use of hand injection. Hand injection may be used for a long and narrow central catheter, especially a peripherally inserted central line, and for an angiocatheter inserted into the hand or foot. Before power injection, unobstructed delivery of the saline flush and unrestricted return of blood should be confirmed to avoid extravasation of the contrast agent. Because patients with CHD often have right-to-left shunt, which has an increased risk of air embolism, particular attention should be paid to clearing air bubbles from the tubes and connections.
The maximum injection rate (1.5–4.0 mL/sec) of iodinated contrast agent depends on the size of the placed angiocatheter (5). In general, such high injection rates are not necessary in children with CHD, and lower injection rates (0.3–3.0 mL/sec) with longer scan delays (20–30 seconds) (except for subjects with superior or total cavopulmonary connection) are acceptable in attempting to achieve optimal and homogeneous cardiovascular enhancement, especially when scanning is performed using a low tube voltage (4569). Real-time pressure monitoring, when available, is quite helpful for early detection of malfunctioning intravenous line or extravasation of contrast agent, particularly in sedated children. Studies in adult (8384) have shown that small fenestrated catheters with side holes have promising results with respect to the injection rates, vascular enhancement, and safety; these catheters may be useful in patients with small and fragile peripheral veins. Further investigations are warranted to confirm whether equivalent effects would be observed in pediatric patients.
To determine the scan delay, an empirical method, a test-bolus injection method, or a bolus tracking method may be utilized. The use of a fixed delay appears to be inappropriate in children with CHD having complex hemodynamics. A test-bolus injection may accurately predict an optimal scan delay that reflects the individual's hemodynamics, but the use of an additional contrast agent and the increased radiation exposure in small children are its shortcomings. Bolus tracking is the most commonly used method in current clinical practice. The location of a region of interest for bolus tracking and the threshold attenuation to start CT scanning may be different according to each imager's strategy and the diagnostic purpose of the CT examination; a mid-cardiac level that shows the cardiac chambers is often used because complex hemodynamics of CHD can be easily appreciated during the monitoring scans (45611). A monitoring delay should be long enough to minimize additional radiation exposure from monitoring scans (4511). In addition, radiation dose parameters, including the tube voltage and the tube current, of the monitoring scan should be minimized (911).
Go to :
Post-processing
To appropriately evaluate the complex cardiovascular anatomy in CHD, multiplanar and 3D reformations in addition to axial images should be used for image interpretation. A combination of maximum intensity projection, minimum intensity projection, and volume rendering (VR) visualization techniques is commonly utilized to highlight the target anatomic structures as required. Detailed descriptions of these techniques are beyond the scope of this article. Color-coded merging of multiple 3D segmented datasets is often useful to depict different anatomic substrates and their spatial relationships in a single 3D image; for example, this technique has been demonstrated in subjects with vascular airway compression and major aortopulmonary collateral arteries (5685). Transparent-lumen VR imaging is quite useful for illustrating intracardiac anatomy in children with CHD (86). Ventricular volumes can be quantified by using CT datasets in children with CHD (456458788). Recent studies have demonstrated that useful assessment of the pulmonary vascularity ratio can be provided using end-systolic cardiothoracic CT in patients with CHD (8990). Multi-phase cine 2D or 3D analysis may be used to evaluate not only the global and regional ventricular function, but also the respiratory dynamics of the airways, the lungs, and the diaphragms in patients with CHD (456484950515253869192). Post-processing, as CT scanning, should be performed by or under the supervision of an experienced radiologist, but it should not routinely be performed by a radiology technician along since this may lead to a misinterpretation due to a pseudo-lesion or a missed lesion. Accurate and detailed segmentation of 3D CT dataset is also crucial for developing 3D printed heart models (93).
Go to :
Vendor-Specific Protocols
Siemens Healthineers
A dual-source CT scanner is indeed a technical innovation in cardiac CT (93). The most distinguished advantage of this scanner type is the high temporal resolution, which is equivalent to a quarter of the gantry rotation time: 83 msec for a first-generation scanner; 75 msec for a second-generation scanner; and 66 msec for a third-generation scanner (1193), which is exceedingly useful in children with CHD and high heart rates. Another eminent imaging technique useful for pediatric cardiothoracic CT that exclusively available from this manufacturer is high-pitch dual-source spiral or helical scan mode that is available in second- and third-generation dual-source scanners (3194). The high-pitch scan mode considerably reduces cardiac and respiratory motion artifacts in children by drastically reducing the scan time, while maintaining the low radiation dose (9596). There are two types of high-pitch dual-source spiral or helical scan modes applicable to pediatric cardiothoracic CT: non-ECG-synchronized mode, pitch up to 3.2 (3132); and prospectively ECG-triggered mode, pitch up to 3.4 (979899). A recent study using a second-generation dual-source CT scanner (14) disclosed that additional ECG triggering did not substantially reduce cardiac motion artifacts on high-pitch dual-source spiral or helical pediatric cardiothoracic CT in young children with CHD.
A couple of radiation dose reduction techniques are available from this CT manufacturer, and some of them are exclusively available from this manufacturer. Combined longitudinal and transverse tube current modulation (CARE Dose 4D; Siemens Healthineers, Forchheim, Germany) is almost universally available in all types of CT scans. Organ-based tube current modulation may be utilized to reduce radiation exposure to the breasts when available. For retrospectively ECG-gated spiral or helical CT scan, two types of ECG-controlled tube current modulation are available; a conventional one offers 20% of full tube current outside pulsing window as in other CT manufacturers, whereas only 4% of the full tube current is produced outside the pulsing window in a more aggressive type (MinDose; Siemens Healthineers). Overall the radiation dose in dual-source retrospectively ECG-gated spiral or helical cardiothoracic CT can be reduced by approximately 15% by using the "chest pain" protocol, in which, unlike conventional protocol, a half of the radiation dose is utilized outside the heart (100). The study (100) also demonstrated that a tube current modulation curve over the whole scanning range provided in real-time was useful to avoid tube current saturation. Heart-rate-adaptive pitch allows a reduction of the radiation dose and the scan time in retrospectively ECG-gated spiral or helical scan. The availability of 70 kV is quite useful in reducing the radiation dose and increasing the iodine contrast-to-noise ratio in young children with CHD (101). ECG pulsing is also applicable in prospectively ECG-triggered sequential CT scans from this manufacturer as it is in retrospectively ECG-gated spiral or helical scans. Adaptive section collimation, which reduces the effect of z-overranging, is almost routinely available from this manufacturer (6).
The best systolic and diastolic phases can be automatically selected after retrospectively ECG-gated spiral or helical scan by using a 4D motion map (Cardio BestPhase; Siemens Healthineers), and this helps to simplify the workflow (33). Automatic tube voltage selection software (Care kV; Siemens Healthineers) helps imagers to optimize the CT radiation dose (102). The isocenter line displayed on the lateral scout view is very helpful in adjusting the vertical centering of a child before CT scanning. The extent of z-overranging is also indicated on CT scout images (6).
Three versions of iterative reconstruction algorithm are available in dual-source CT scanners for reducing image noise without substantially affecting the anatomic details. The latest version (ADMIRE; Siemens Healthineers) has been recently reported to improve the objective and subjective image quality when a low-dose 70 kV chest CT angiography is performed in young children (67).
Canon Medical Systems
A 320-detector-row CT scanner (Aquilion ONE; Canon Medical Systems, Otawara, Japan) with a 16 cm coverage in its z-axis was introduced in 2007. The 16-cm longitudinal coverage has several advantages when performing pediatric cardiac CT. In fact, the longitudinal coverage is usually long enough for the whole heart in older children and for the whole chest in young children. Because the total scan range in pediatric cardiac CT can be acquired in one gantry rotation in most of cases, cardiac and respiratory motion artifacts can be reduced. Moreover, sequential scanning in a single imaging slab can completely eliminate respiratory misregistration artifacts as well as differences in contrast enhancement between adjacent imaging slabs that often occur in several sequential scans during free breathing in other CT scanners with shorter z-axis coverage. For pediatric cardiac CT, four scan modes, which are target scan, prospective scan, and continuous scans with and without ECG modulation, may be utilized according to the heart rate and the required acquisition window in the cardiac cycle. Among them, the single-beat target scan with the minimum acquisition window is usually sufficient for pediatric cardiac CT (68).
The fastest gantry rotation time available from this vendor is 275 msec, and the temporal resolution of half reconstruction, which is approximately 140 msec, may be insufficient in patients with high heart rates. Notably, the vendor provides a unique CT imaging technique, called "variable helical pitch" scanning, which allows a seamless change of pitch during one continuous acquisition and enables the combination of ECG-gated and non-ECG-gated acquisition within one scan (103). The scan mode appears particularly useful in reducing the radiation exposure of pediatric cardiac CT requiring longer scan ranges such as the evaluation of the anomalous pulmonary venous connection and the Fontan pathway. Multiple wide volume scans may be used to acquire such longer scan ranges with low radiation dose, but the artifacts caused by the difference in contrast enhancement between the volumes are inevitable.
In planning the scan parameters of pediatric cardiothoracic CT, a user may be guided by the automatic software (SURE Cardio and SURE kV; Canon Medical Systems). In addition, the workflow can be simplified by utilizing automatic selection of the best cardiac phase instead of performing manual selection (PhaseXact; Canon Medical Systems). To reduce the radiation dose of pediatric cardiac CT, ECG-controlled tube current modulation in retrospectively ECG-gated spiral or helical scan and organ-based tube current modulation are available as in other vendors. The most recent version (FIRST; Canon Medical Systems) of iterative reconstruction algorithm can improve image quality of a low-dose ECG-gated pediatric cardiothoracic CT, compared with those an older version (68).
General Electric Healthcare
The most recent CT scanner (Revolution; GE Healthcare, Waukesha, WI, USA) can also provide a wide longitudinal coverage of up to 16 cm. As previously described, the scanner also has the advantages of one beat or single rotation sequential scanning; these advantages include the reduction of cardiac and respiratory motion artifacts as well as absence of respiratory misregistration and different-enhancement artifacts. The scan coverage of axial or sequential scanning can be adjusted by using variable collimation (4, 8, 10, 12, 14, and 16 cm), and this can reduce unnecessary radiation exposure to small children. The determination of the optimal CT scan parameters may be guided by utilizing software (Auto gating and kV Assist; GE Healthcare) as it is with other vendors. In addition, the best cardiac phase may be automatically selected (Smart Phase; GE Healthcare). Tube current modulation based on noise index and ECG-controlled tube current modulation are available to reduce the radiation dose of pediatric cardiac CT. Several versions of iterative reconstruction algorithm can be used to reduce image noise while maintaining anatomic details.
Of note, motion artifacts of the coronary arteries can be reduced by utilizing an intracycle motion correction algorithm (Snapshot Freeze; GE Healthcare), especially in the evaluation of the right coronary artery (104). To compensate for coronary motion, cardiac phases adjacent to the target phase within a single cardiac cycle are used in the algorithm. This technique is less vulnerable to beat-to-beat variability than multi-segment reconstruction is because the former operates on a single cycle (104). However, it remains to be determined whether the motion correction algorithm is also useful in pediatric cardiac CT.
Philips Healthcare
A single-source dual-layer CT scanner with a unique spectral detector was recently introduced and allows dual-energy CT evaluation (105). Because basic ECG-synchronized scan options are available in Philips CT scanners, cardiovascular structures–including the coronary arteries–can be evaluated using end-systolic ECG-synchronized cardiac CT even in newborns with CHD (3715). Nevertheless, beta-blockers seem to be helpful to compensate for the limited temporal resolution (the gantry rotation of 0.27 second) of cardiac CT and to reduce the cardiac motion artifacts on pediatric cardiac CT images acquired at high heart rates. On the other hand, an adaptive multi-segment or multi-cycle reconstruction algorithm is not really effective in increasing the temporal resolution and is susceptible to variable heart rates or arrhythmias. The longitudinal coverage of the modern CT scanners produced by the vendor is in the range of 4.0–8.0 cm; therefore, the whole scan range of pediatric cardiac CT examination cannot be covered in one heartbeat or single gantry rotation with these scanners. A recently developed knowledge-based iterative reconstruction algorithm (IMR; Philips Healthcare, Cleveland, OH, USA) can improve the image quality of cardiac CT in infants with CHD; however, small structures, such as a small patent ductus arteriosus and coronary arteries, are blurred or missed (106).
Go to :
SUMMARY
We have provided in this article serves a comprehensive vendor-specific guideline with respect to the imaging techniques for cardiothoracic CT in children with CHD based on the consensus opinions of the experts the Asian Society of Cardiovascular Imaging. The first part of the guideline includes recommendations on patient preparation, scan techniques, radiation dose reduction techniques, intravenous iodinated contrast agent injection protocols, and post-processing techniques. Therefore, the guideline may be used to shape each user's own protocol, especially with reference to the same vendor-specific descriptions. Selecting a CT scanner for cardiac imaging is the heart of the matter (107) because it is really technically demanding to obtain excellent image quality of pediatric cardiothoracic CT. In this respect, the detailed comparative information of the most recent CT scanners described in this article may help a user to select a new CT scanner for pediatric cardiothoracic CT based on the specific institutional requirements.
Go to :
 XML Download
XML Download