

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sepsis is a critical illness with high morbidity and mortality [123]. A population-based study estimated the prevalence of episodes of bloodstream infections (BSI) to be 575,000–677,000 in North America and 1,200,000 in Europe per year, and deaths due to BSI were estimated to be 79,000–94,000 in North America and 157,000 in Europe per year [3].
Blood culture is essential for the diagnosis of sepsis, and early reporting is crucial for a better outcome in sepsis patients [4]. The currently available blood culture systems such as BacT/Alert 3D (BioMérieux, Durham, NC, USA), BD BACTEC FX (BD Diagnostics, Franklin Lakes, NJ, USA), and VersaTREK (Thermo Fisher Scientific, Waltham, MA, USA), have the benefits of early detection and high sensitivity [5]. As antibiotics are administered to many inpatients before blood collection, resin-based media may enhance the growth of microorganisms by adsorbing antibiotics or serum inhibitors [16]. Consequently, the aerobic (FA Plus) and anaerobic (FN Plus) bottles of the BacT/Alert system (BioMérieux) have polymeric adsorbent beads, and the BD BACTEC Plus (BD Diagnostics) system contains resins inside the bottles to help the growth of microorganisms.
BacT/Alert Virtuo (Virtuo; BioMérieux) is the only system that has automatic registration, loading, and unloading of the blood culture bottles. Virtuo is a closed system, which may enhance the growth of microorganisms due to the stable incubator temperature (35–37℃) compared with an open system such as the BacT/Alert 3D system. In addition, Virtuo has an advanced algorithm to detect microorganisms faster and has a function to measure the blood volume. We prospectively compared the positive rate and time to detection (TTD) between these two blood culture systems, using resin bottles for the clinical samples.
METHODS
Blood collection
Patients with suspected sepsis (N=952) visiting the emergency department (N=686) or admitted (N=266) to Gyeongsang National University Changwon Hospital (GNUCH) and with requested blood cultures were enrolled. Median (interquartile range, IQR) age of the patients was 62 years (45–76 years), and males (54.1%) were more than females.
Two sets of blood samples were collected from each patient. Once the antecubital area was disinfected with 2% chlorohexidine-alcohol, 20 mL of blood was collected using a syringe in the emergency department. The sample was divided equally into two FA Plus and FN Plus bottles. A butterfly needle, connected with a blood collection adapter cap (BioMérieux), was used to draw blood from the admitted patients, and 5 mL of blood was dispensed. These bottles were randomly inserted into the Virtuo and 3D systems at the same time as soon as they arrived at the laboratory. The bottles were incubated for five days at 35.5℃ or until there was a positive signal in the blood culture systems.
The positive rate was defined as the percentage of growth of microorganisms among the experimental blood cultures. TTD was defined as the time lapse between entry of the bottles into the system and the observation of a positive signal in the machine. The software version was 02.01.06.928 for Virtuo, 4.0.0.29 for Myla middleware B.40, and Rel.4 for 3D. The positive rate and TTD were compared between Virtuo and 3D. This study was approved by the Institutional Review Board (No. 2016-09-004) of GNUCH.
Culture and identification
Once the positive signal was detected in the blood culture systems, 1 mL was drawn out for Gram staining and culture. Culture was routinely performed using a blood agar plate (BAP), MacConkey agar, and chocolate agar for aerobic culture; Sabouraud dextrose agar, if fungus was observed; and Brucella agar for anaerobic culture. Colonies of bacteria or yeasts were identified with either Vitek matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF) mass spectrometry (BioMérieux) or the Vitek 2 system (BioMérieux). The clinical relevance of the isolates was categorized into three groups: clinically significant, contaminant, and indeterminate, according to a previous report [2]. An infectious disease specialist reviewed the medical records for interpretation of the positive results. All positive bottles were weighed. Approximately half of the negative bottles were measured for weight and were subcultured on BAP and chocolate agar. The blood volume was calculated as the blood weight divided by 1.055 [7].
Statistical analysis
We used the Mann-Whitney test to compare median age between positive- and negative cases. The positive rate was expressed as a proportion of the total number of blood cultures. The difference in positive rates between the Virtuo and 3D systems for FA Plus and FN Plus bottles were compared using the McNemar's test. TTDs and collected blood volumes were expressed as the median with interquartile range (IQR) and as the mean with standard deviation (SD), respectively. Normality and equal variance assumptions were confirmed by the Shapiro-Wilks test and Levene's F-test, respectively, for TTD and blood volume data. TTD was compared according to the bottle types (FA Plus vs FN Plus) and for each bacterial pathogen separately. If the assumptions were not satisfied, the differences in TTD or blood volume between the two systems were compared by the non-parametric Wilcoxon signed-rank test.
Spearman's rank correlation was analyzed to evaluate the correlation of TTD between the Virtuo and 3D systems. SPSS 21.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. Two-sided P<0.05 was considered statistically significant.
RESULTS
Blood collection volume
The means±SD blood volumes of positive bottles (N=251) were 5.2±1.5 mL in Virtuo and 5.3±1.5 mL in 3D, respectively (P=0.064). The mean±SD blood volumes of negative FA Plus bottles were 5.4±1.2 mL in Virtuo (N=1,021) and 5.5±1.2 mL in 3D (N=1,057) (P=0.382). The mean±SD blood volumes of negative FN Plus bottles were 4.7±1.4 mL in Virtuo (N=1,013) and 4.7±1.3 mL in 3D (N=1,068) (P=0.716).
Positive rate
Positive rates of the 1,904 blood culture sets did not differ between the Virtuo and 3D systems for both the FA Plus (8.3% vs 8.4%, P=0.664) and FN Plus bottles (7.8% vs 8.3%, P=0.099). The median age of positive cases was higher than that of negative cases (median, IQR: 71, 57–78 vs 61, 45–75) (P<0.0001).
Among the 355 total isolates obtained, 337 (aerobic 169+anaerobic 168) (94.9%) were clinically significant microorganisms, 12 (3.4%) were contaminants, and six (1.7%) were indeterminate. The proportion of coagulase-negative staphylococci was only 1.1% (3/269) among the positive isolates. Terminal subculture of negative bottles (approximately 55% of all bottles) did not show growth of any microorganism. Polymicrobial growth was observed in eight bottles (2.3% of positive bottles), which were excluded from the data analysis.
TTD of clinically significant pathogens
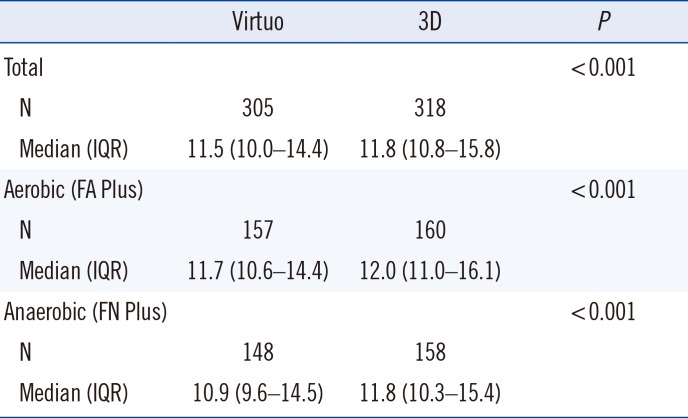
The median TTDs were significantly shorter in all bottles (18 minutes, 11.5 hours vs 11.8 hours), as well as in FA Plus (18 minutes) and FN Plus (54 minutes) in the Virtuo system (all P<0.001) (Table 1).
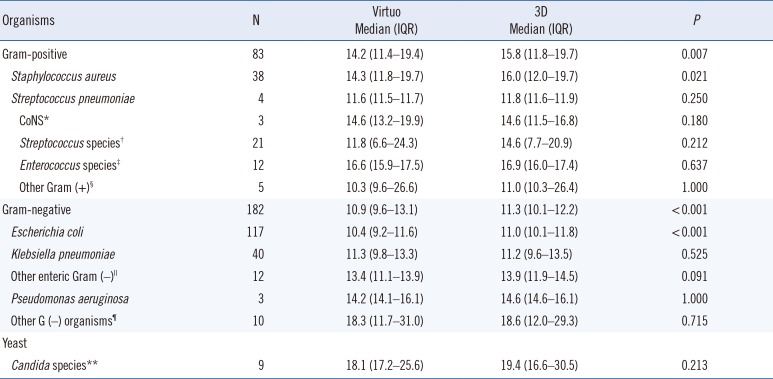
Similarly, the TTD for Staphylococcus aureus and all gram-positive organisms was longer with 3D than with Virtuo (P=0.021 and 0.007, respectively) (Table 2). Although the same trend was observed for Streptococcus species and Enterococcus species, the difference was not significant. In addition, the TTD for Escherichia coli and all gram-negative organisms was also longer for 3D than Virtuo (P<0.001 for both), although TTD did not differ for Klebsiella pneumoniae (P=0.525). TTD for Candida species did not differ between the two systems (P=0.213).
Correlation of TTD in the two systems
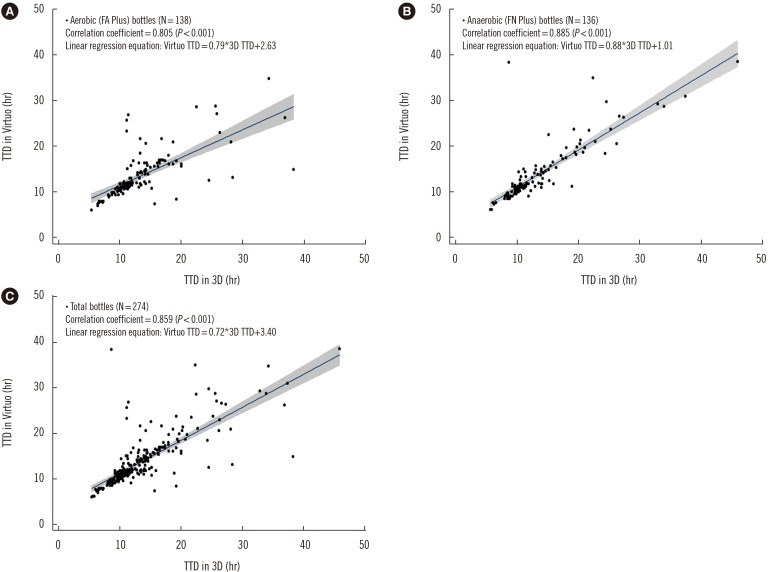
The correlation coefficients (ρ) of TTD between Virtuo and 3D were 0.805, 0.885, and 0.859 for FA Plus bottles, FN Plus bottles, and all bottles, respectively (P<0.001; Fig. 1). The correlation coefficients of (ρ) of TTD between Virtuo and 3D were 0.832 and 0.890 for E. coli and S. aureus, but 0.592 for K. pneumoniae. There were two outlier cases exceeding 20 hours of difference in TTD between Virtuo and 3D.
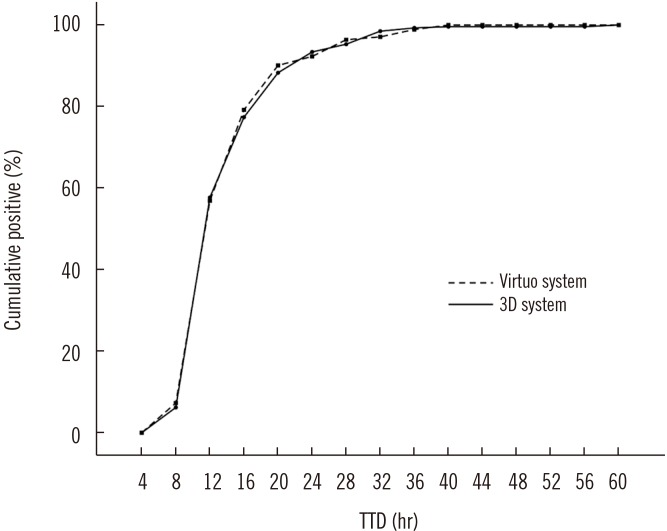
The cumulative proportions of positive results by TTD were very similar between two systems (Fig. 2): approximately 50% of the samples were positive by 12 hours, 80% by 16 hours, and 90% by 24 hours.
DISCUSSION
In this clinical study, we used a four-bottle design, with the bottles inserted into the Virtuo and 3D systems at the same time, which enabled head-to-head comparison of the positive rate and TTD between the two systems. The optimal blood volume collected, and the low skin contamination rate indicated that blood collection was carried out well overall. The proportion of clinically significant pathogens (94.9% of positives) was higher than that of other reports [28].
The positive rates of Virtuo and 3D were similar, indicating that Virtuo has an equivalent capability of detecting pathogens to 3D. Although there were slightly more pathogens growing in 3D only than in Virtuo only, the difference was not statistically significant. The proportion of pathogens growing in both Virtuo and 3D was also greater that that reported previously (84.9% vs 68.7%) [8], which indicates that the chance of missing pathogens might have been reduced in our study. Since the bottles were randomly inserted into the machines, this difference in the positive rate might have occurred by chance. However, further research is warranted to determine why the positive rate was always slightly lower in the Virtuo than in the 3D system.
A previous clinical study showed that the Virtuo detected microbial growth two hours earlier than the 3D on an average (15.9 hours vs 17.7 hours) [8]. Although our study showed an 18-minute earlier detection in Virtuo, the median TTD (11.5 hours in Virtuo; 11.8 hours in 3D) was much shorter than the value reported in the previous study. Delivery lag to the laboratory or delayed entry into the machine [910], blood collection volume [1112], and spectrum of pathogens might have affected the TTD. The previous study noted suboptimal mean blood volumes (4.4 mL for Virtuo and 4.3 mL for 3D), whereas our study had optimal blood volume (5.2 mL for Virtuo and 5.3 mL for 3D). The previous study analyzed TTD in 119 isolates, wherease we investigated TTD in 274 isolates, which may produce more accurate data. The same study also found a significantly shorter TTD for enteric gram-negative bacilli (3.6 hours) and enterococci (2.3 hours) [8], whereas in the present study, TTD was significantly shorter for all gram-positive organisms (96 minutes), S. aureus (102 minutes), all gram-negative organisms (24 minutes), and E. coli (36 minutes) in Virtuo.
Another clinical study using blood culture bottles for body fluids showed that TTD was three hours shorter in Virtuo than in 3D (median 12.5 hours vs 15.5 hours) [13]. However, that study used body fluids, not blood cultures.
Further, a retrospective study comparing the TTD between two different periods showed that the cumulative percentage was shorter for common pathogens using Virtuo than using 3D [14]; however, the method of measuring the TTD was not clearly described. In addition, this was not a head-to-head comparison. Our prospective study did not show a difference in cumulative percentage between Virtuo and 3D.
TTD for clinically significant pathogens was strongly correlated between Virtuo and 3D. A simulated blood culture evaluation study showed a similar correlation of TTD between Virtuo and 3D (r=0.91; P<0.001), and the TTD was also significantly shorter in Virtuo than in 3D (median 12 hours vs 15 hours; P<0.001) [15]. Another simulated blood culture study revealed that the TTD was three hours shorter in Virtuo than in 3D [16], whereas a similar study found no significant difference between Virtuo and the BD BACTEC FX system [17]. The cumulative proportion of positive results showed a similar pattern between Vituo and 3D in our study, indicating an equivalent detection capability. In addition, 80% of the isolates were detected within 16 hours, which is earlier than in the previous report [18].
Our study has several limitations. Not all of the negative bottles were subcultured to rule out false negatives. In addition, the false positive rate was not evaluated. Anaerobic cultures were performed selectively when there was no growth in the aerobic culture and when Gram staining showed positive results. Two-thirds of the blood samples analyzed were derived from patients at the emergency department; hence, the results might differ from that of inpatients. In addition, the specific demographic characteristics of the patient group or disease severity might have affected the distribution of pathogens as well as the TTD data.
Despite these limitations, our results indicate that Virtuo has a significantly shorter TTD than 3D for all the bottle types and for two of the most commonly encountered pathogens (S. aureus and E. coli) of sepsis, while its detection capability was equivalent to that of 3D. Virtuo has the potential to detect pathogens early in all bottle types, which might improve the prognosis of sepsis by allowing for implemention of expeditious management
 XML Download
XML Download