

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Maintaining adequate levels of sedation and analgesia in a mechanically ventilated patient is essential for regulating anxiety and agitation, providing suitable ventilation and oxygenation, ensuring conformity with the ventilator, and allowing for the smooth conduct of other procedures and treatments.1234 It is even more important in children compared with adults, because children in general lack understanding about why they are intubated with an endotracheal tube and placed on mechanical ventilation, which leads to increased agitation.56 Furthermore, because children are unable to appropriately express the degree or location of their pain, discriminating the cause of their irritability and agitation can be more difficult than in adults. Thus, sedation therapy for children requires more careful attention.7
Although sedation during mechanical ventilation is a cornerstone of daily pediatric intensive care unit (PICU) patient management, there is still a lack of evidence to define the best practice. Because there is no established guideline on sedation therapy for mechanically ventilated children, hospitals have implemented their own various sedation protocols.489101112 In addition, since there are few studies in children, it is inevitable to estimate the effect of sedation protocol in children based on the results of adult studies.13
In Korea, the administration of fentanyl in adult patients receiving mechanical ventilation is approved by Ministry of Food and Drug Safety (MFDS) of Korea because of medical evidences such as the randomized controlled trial (RCT) mentioned above. However, since the use of fentanyl in children with mechanical ventilation has not been approved by MFDS because of a lack of medical evidences such as previous studies, it is inevitable to use fentanyl off-label. Pediatric patients need more careful treatment because they feel more anxiety than adults and do not adequately express anxiety and pain. Nonetheless, there is a contradiction in the use of fentanyl as off-label in children who need more detailed sedation therapy than adults.
Therefore, to address these drawbacks, the MFDS had proposed a study. The aim of this study was to evaluate the efficacy and safety of fentanyl in children receiving mechanical ventilation.
METHODS
Study design and participants
This double-blind, parallel, two-group, RCT was conducted from April 24, 2013 to January 23, 2015 at a PICU with 20 beds within a tertiary university children's hospital. Patients between 2 months and 18 years of age who were placed on mechanical ventilators at the PICU were included as candidates. Patients with hypotension at the time of registration were excluded. In this study, hypotension was defined using the following criteria: systolic blood pressure (SBP) < 70 mmHg in patients between the ages of 2–12 months, SBP < 70 + (age in year × 2) mmHg in ages between 1–10 years, and SBP < 90 mmHg in ages greater than 10 years.14 Patients with the following underlying diseases were also excluded: any disorders of the central nervous system that may affect the consciousness level, and renal impairment that may influence both serum concentration and effectiveness of the drug. We regarded patients to have renal impairment when the calculated estimated glomerular filtration rate by the Schwartz equation was less than 50 mL/min/1.73m2.15 Patients administered with neuromuscular blocking agents were also excluded, because evaluation of the level of sedation is impossible in such cases.
Group allocation and randomization
Eligible patients were randomly allocated into two sedation groups. The control group, which did not receive fentanyl, also needed sedation, so midazolam, a commonly used sedative in mechanical ventilation, was administered to all subjects.781016 Thus, the experimental group received fentanyl in combination with midazolam, and the control group received midazolam alone.
Randomization was performed through block randomization method without stratified factor. The randomization code of the patient was issued through a web-based random number generator operated by the medical research collaborating center of Seoul National University Hospital. After randomization, the randomization code was transferred to the assigned research pharmacist to prepare the ‘experimental drug’; normal saline in the control group, versus fentanyl in the combination group. In order to avoid being distinguished by appearance, the experimental drugs were packaged in 50 mL syringes, diluted into volumes of 25 mL. For patients in the control group, only 25 mL of normal saline was packaged as the experimental drug. For patients in the combination group, fentanyl citrate was diluted with normal saline into a final 20 μg/mL concentration to make a 25-mL solution. In order to maintain a double-blind status, the research pharmacist was not involved in any other processes of this study except in the preparation of the experimental drug.
Procedures
In cases where intubation was performed in the PICU, midazolam 0.1 mg/kg, fentanyl 1 μg/kg, and vecuronium 0.1 mg/kg were administered as preparation drugs. For all study participants, the patients' assigned nurse prepared midazolam, which was to be continuously infused during the study. When both the experimental drug and midazolam were ready for administration, the study was initiated with continuous infusions of both drugs. The initial infusion rates of midazolam and the experimental drug were 0.06 mg/kg/hr and 0.05 mL/kg/hr, respectively. The infusion rates were then adjusted according to the sedation level.
The sedation level was assessed using the Comfort Behavior Scale (CBS), which is a scale used worldwide for children undergoing sedation.171819 Prior to initiating the study, considering the medical condition of each patient and their expected duration of mechanical ventilation, the patients' assigned research physician determined their individual target CBS score, and re-evaluated its validity through reassessments every 8 hours during the study period. CBS scores were measured regularly at one-hour intervals from study initiation, and additional CBS scores were measured whenever the patient was suspected of awakening from sedation.
Under-sedation was defined as the measured CBS score ≥ 4 points above the target CBS score. Over-sedation was defined as a measured CBS score ≥ 4 points below the target CBS score. In cases with under-sedation, the midazolam infusion rate was increased by 0.03 mg/kg/hr, and the experimental drug infusion rate by 0.025 mL/kg/hr, if the infusion rate had not been altered within one hour. Likewise, in cases with over-sedation, the infusion rate was decreased by the same amount for each drug. In order to prevent an overdose of medications, the infusion rates of midazolam and experimental drug were limited to a range of 0.03–0.36 mg/kg/hr and 0.025–0.3 mL/kg/hr, respectively. If the CBS difference (defined as the target score subtracted by the measured score) was ≥ 8 points, it was considered as serious under-sedation, and a bolus of midazolam (0.1 mg/kg) was injected intravenously for a rapid regulation of the under-sedation status.
The study lasted up to 48 hours if there were no interruptions throughout the study process, after 48 hours, the sedation therapy was performed according to the patient's condition regardless of sedation group or research sedation protocol. If mechanical ventilation weaning was carried out before 48 hours or if any adverse events occurred, the study was immediately terminated. The study was also discontinued for the following reasons: administration of other sedatives or analgesics making it difficult to evaluate the sedation level, application of continuous renal replacement therapy which affects the serum level of drugs, sedation failure even with maximal infusion rates of medications, and co-administration of medications that mask adverse reactions of fentanyl such as antihypertensive drugs.
Outcomes
The primary outcome of this study was to investigate the time ratio of under-sedation (defined as cumulative hours with a CBS difference of ≥ 4 points divided by hours of drug administration) in the two sedation groups. The secondary outcomes were to analyze the CBS differences, time ratio of serious under-sedation, and total amount of midazolam used during study period in each of the sedation groups.
Sample size calculation
In order to calculate a suitable sample size for this study, we need to know the mean difference and standard deviation (SD) of the CBSs of the two groups to be compared. Since there is no previous research on the pediatric population, the sample size was estimated based on a similar adult study instead.13 Because it was an adult study, the sedation level was assessed using Modified Ramsay Sedation Scale and therefore, the scale and score ranges of the CBS used in this study are different. However, as mentioned earlier, previous studies in the pediatric population do not exist, thus we inevitably used the results of the adult study to estimate the approximate number of samples. In the above study, the mean difference between the two groups was 4.9 and the SD was 4.9. For α error of 5% (two-tailed) and a β error of 20%, 17 samples were required for each group.23 Assuming a 20% drop-out rate, we planned to recruit a total of 44 participants, 22 patients per group.
Statistical analysis
Shapiro-Wilk normality test was performed for continuous data to determine whether the data were normally distributed or not. Continuous data were presented as mean ± SD if it was determined to be normally distributed. If the data was not normally distributed, data were shown as median (interquartile range [IQR]). Two-sample t-test was used in analyzing normally distributed continuous data, and Wilcox rank sum test for nonparametric data. For categorical data, χ2 test or Fisher's exact test was adopted in the analyses. In order to analyze the effects of study time on the sedation level and CBS between the sedation groups, we used mixed effect logistic regression model with study time as random effect and sedation group as fixed effect. P values less than 0.05 were considered statistically significant. All statistical analyses were performed using R version 3.4.1 (R Foundation for statistical computing, Vienna, Austria).
Ethics statement
If the inclusion and exclusion criteria of this study were satisfied, after explanations pertaining to the details of this study, a written informed consent was obtained from a legally authorized representative of the patient. Afterwards, the patient was regarded as an eligible study participant and research was then advanced on the patient. This trial was approved by the Institutional Review Board of Seoul National University Hospital (H-1210-127-437), and the procedures were in accordance with the Helsinki Declaration.
RESULTS
During the study period, 2,065 patients were screened, and 44 patients were enrolled and randomly assigned to a sedation group. Six of the patients who received randomization were excluded from the study because their consent was withdrawn before the initiation of the study (Fig. 1). The median age of the patients included in the analyses was 2.3 (0.6–10.8) years, and 23 (60.5%) patients were men. Baseline characteristics of the sedation groups are listed in Table 1. There were no statistically significant differences between the groups.
 | Fig. 1Flow of participants. Of the 2,065 patients admitted to the PICU during the study period, 44 patients were enrolled and randomly assigned, with 22 patients in either the control group or combination group.PICU = pediatric intensive care unit, CNS = central nervous system.
|
Table 1
Enrolled patients' baseline characteristics before drug administration during the study
Normally distributed continuous data were presented as mean ± standard deviation, and nonparametric continuous data as median (interquartile range). Categorical data were presented as number (%).
SBP = systolic blood pressure, GFR = glomerular filtration rate, PIM = pediatric index of mortality.
![]()
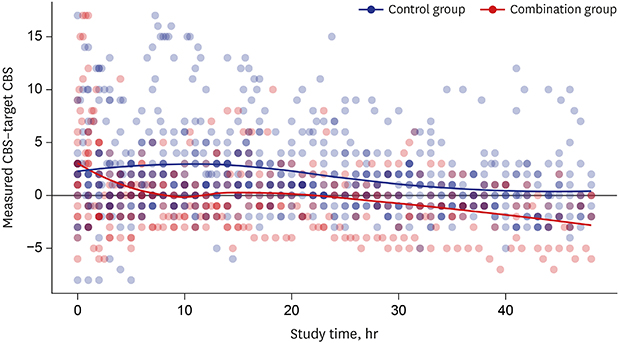
The total duration of the study period (drug administration) was 47 (11.1–48) hours in the control group and 13 (6–37.5) hours in the combination group (P = 0.09). A total of 1,137 CBS scores were measured; we analyzed this by observing different trends in the scores of the patients throughout the study period. The median target CBS score in the control and combination groups were 12 (10–12) and 11 (10–12), respectively. There was no statistically significant difference between the groups (P = 0.257). However, there was a significant difference in the median measured CBS score (P < 0.001). The differences in the target and measured CBS scores (CBS difference) also showed significant differences between the sedation groups (P < 0.001), and it was consistently prominent with time (Table 2 and Fig. 2).
Table 2
Comparison of the sedative effects between the two groups

Continuous data were presented as median (interquartile range).
SE = standard error, CBS = Comfort Behavior Scale, NA = not applicable.
aCBS difference: measured score of CBS – target score of CBS; bTime ratio of under-sedation: cumulative hours with a CBS difference of more than or equal to 4 points divided by the drug administration hours; cTime ratio of serious under-sedation: cumulative hours with a CBS difference of more than or equal to 8 points divided by the drug administration hours.
![]()
 | Fig. 2Differences between measured CBS score and target CBS score. The differences in the target and measured CBS scores (CBS difference) were calculated for the patients throughout the study period for the control group (blue) and combination group (red).CBS = Comfort Behavior Scale.
|
The overall time ratio of under-sedation in the combination group (median, 0.06; IQR, 0–0.2) was lower than the control group (median, 0.15; IQR, 0.04–0.29) (P < 0.001). The time ratio of serious under-sedation was significantly different between the groups (P < 0.001). Another efficacy outcome was the total amount of midazolam administered during the study period. The total amount administered to the patients was significantly lower in the combination group (median, 0.07 mg/kg/hr; IQR, 0.06–0.11 mg/kg/hr) compared with the control group (median, 0.11 mg/kg/hr; IQR, 0.07–0.14 mg/kg/hr) (P < 0.001) (Table 2).
On the other hand, coma, ileus and mortality did not occur during the study, but hypotension occurred in 4 cases. This occurred in two cases for each sedation group, and was not statistically significant (P = 1.000). The vital signs measured during the study were not different between the sedation groups. Estimated glomerular filtration rate, oxygenation index, and ventilation index were also not different between the two groups (Table 3).
Table 3
Adverse events and clinical findings during study in the two groups

Normally distributed continuous data were presented as mean ± standard deviation, and nonparametric continuous data as median (interquartile range). Categorical data were presented as number (%).
SBP = systolic blood pressure, NA = not applicable, GFR = glomerular filtration rate.
aClinical findings: values measured or calculated in the course of drug administration during the study period.
![]()
DISCUSSION
The results of our study show that a combination therapy of midazolam and fentanyl in mechanically ventilated children is more effective than midazolam monotherapy demonstrated by a lower time ratio of under-sedation in the combination group compared to the control group. Moreover, continuous fentanyl infusion combined with midazolam is safe without any increased incidences of adverse reactions.
In this study, although the target CBS scores were similar for both sedation groups, the combination group showed a significantly lower measured CBS score than the control group, suggesting that the combination group had a more adequate level of sedation. Moreover, the overall infusion rate of midazolam was evidently lower in the combination group compared to the control group. As is generally well known for its merits of combination therapy, this reduces the possibility of drug adverse events caused by the usage of high drug doses, which are known to increase in the incidences of adverse events and withdrawal symptoms.12425
In this study, the time ratio of under-sedation in the combination group (0.06 [0–0.2]) was significantly lower than the control group (0.15 [0.05–0.29]). In a previous RCT on adults, the “off-target” hours per day in the midazolam-only group and co-sedation group (midazolam and fentanyl) were 9.1 ± 4.9 and 4.2 ± 2.4, respectively.13 Although it is difficult to make direct comparisons due to differences in the subject and measurement scale, the "off-target" time ratio for midazolam alone was similar in both studies, 2–2.5 times higher than the combination group.
Meanwhile, there were no cases of mortality, coma, and ileus. Among the adverse reactions, hypotension was the only adverse event that occurred in this study, with two occurrences of hypotension in each group, showing no statistically significant association to a certain sedation group.
However, there was a critical limitation to this study, which was that the subjects dropped out in the study were concentrated in one group, which was not small. Because this study was double-blind, it was unexpected that many of the patients in a particular group were eliminated. And most of the reasons for withdrawal are not directly related to sedation or safety, such as withdrawal of consent or invasive procedures. However, the asymmetry of the number of subjects between the two groups could not be ruled out because it was difficult to exclude the possibility of a bias in the analysis process. However, the additional recruitment of a particular group of subjects in a state after the double blindness has been lifted may lead to greater bias, and even if both groups were randomly recruited, it was difficult to recover the discrepancy in numbers.
In this study, it took about 2 years to recruit 44 subjects. The difficulty in recruiting subjects was due to the difficult selection criteria of underlying disease and concomitant medications. In addition, parents who were reluctant to conduct clinical research for their children were also difficult to recruit. In addition, unlike adults, pediatric patients are more difficult to maintain if they are anxious or irritable because it is difficult to obtain patient cooperation. These are one of the reasons why it is difficult to conduct RCT in children, and we think that this is the reason why there are few RCTs in pediatric patients. Although this study showed the imbalance of the dropout subjects, it is still worthwhile considering that it is difficult to conduct RCTs on children and that there are no pediatric RCT on this topic.
This study had some limitations besides those mentioned above. First, because the study period was designed to last only during the administration of midazolam and fentanyl, information of the patients regarding adverse events after drug discontinuation such as withdrawal symptoms or dependency was not included. Second, because the primary aim of this study was to evaluate the effects of fentanyl in combination with midazolam, the reverse was not analyzed. Third, many cases were eliminated from the study prior to 48 hours for various reasons, especially in the combination group. Therefore, the number of study participants in the two groups was uneven, leading to possible bias in analysis. However, considering that it is difficult to carry out pediatric research, it is expected that this study can be used as a basic data of future pediatric studies even though it is not a perfect study itself.
In conclusion, this trial showed that combination therapy of fentanyl and midazolam is more effective than midazolam monotherapy for sedation therapy in mechanically ventilated children, without any increased risk for adverse reactions. Through this study, the authors expect that more well-designed and well-conducted pediatric RCTs will be performed in the future.
 XML Download
XML Download