

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Twin to twin transfusion syndrome (TTTS) is a complication in approximately 5%–15% of monochorionic twin pregnancies, with 90% of perinatal mortality if untreated.12 Because of high mortality, several treatments such as amnioreduction, selective feticide, and fetoscopic laser ablation have been suggested, and among these treatment modalities fetoscopic laser ablation is the only method reversing the pathophysiologic problem in TTTS. Indeed, fetoscopic laser ablation is now considered as the first choice of treatment in TTTS with stage 2–4 before 26 weeks, because fetoscopic laser ablation showed better outcome.3
The reported neonatal survival after fetoscopic laser ablation is 45%–70%, and several studies have issued the prognostic factors associated with neonatal survival.45 However, until now there is a paucity of information on the factors which are associated with fetal survival or death immediate after the fetoscopic laser ablation, although fetal death immediate after the procedure is one of the major complications we should consider on the decision of the procedure.
The aim of this study was to determine prognostic factors that can affect the fetal survival immediate after fetoscopic laser ablation in TTTS.
METHODS
Study population
In this retrospective study, twin pregnant women who underwent fetoscopic laser ablation for TTTS in Seoul National University Hospital from July 2011 to June 2018 were included. Cases in-utero fetal demise before the procedure were excluded. Fetal survival immediate after procedure was defined as survival to 48 hours after procedure. Clinical characteristics and ultrasound findings were compared according to the fetal survival or death immediate after procedure.
Ultrasound findings
In monochorionic twin, TTTS was diagnosed as the presence of polyhydramnios in one twin and oligohydramnios in the other twin, and cases were categorized according to the Quintero staging system.6 Abnormal Doppler finding was defined as 1) absence of end-diastolic flow or the presence of reversed flow in umbilical artery Doppler or 2) the presence of pulsatile flow in umbilical venous Doppler or 3) the absence of end-diastolic flow or the presence of reversed flow in ductus venosus. Hydrops was defined as fluid accumulation in at least two of the body compartments (subcutaneous edema, pleural effusion, pericardial effusion, or ascites).
Fetoscopic laser ablation
After counseling on the benefit and risk of the fetoscopic laser ablation, written informed consent was obtained from all patients. Under ultrasonographic guidance, a 1.3 mm trocar was inserted into the amniotic sac through the small skin incision. The 8 Fr. curved sheath (11540KB Operating Sheath, curved; Karl Storz SE, Tuttlingen, Germany) or 8 Fr. straight sheath (11540KA Operating Sheath, straight; Karl Storz SE) was introduced according to the location of the placenta. The 11540AA Miniature Straight-Forward Telescope, semirigid, (1.3 mm out diameter, 0° angle of view) was used. After systemic fetoscopic evaluation along the placental vascular equator, selective coagulation of anastomosing vessels was performed. At the end of the procedure, amnioreduction in recipient fetus was done until the recipient amniotic fluid volume became adequate before withdrawing the trocar. After the procedure tocolytics was administered at the discretion of the attending physician.
Statistical analysis
The continuous variables are described as means with standard deviations and were compared with Mann-Whitney U test. Categorical variables were analyzed with Fisher's exact test. Logistic regression was conducted for multivariate analysis. Receiver operating characteristic (ROC) curves for the prediction of fetal death immediate after the procedure were generated for gestational age at procedure, and used to determine the best cutoff values for gestational age at procedure. A P value of < 0.05 was considered statistically significant. SPSS version 21.0 software (SPSS Inc, Chicago, IL, USA) was utilized.
Ethics statement
We follow the ethical standards for human experimentation established in the Declaration of Helsinki. This study protocol was reviewed and approved by The Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. 1311-045-533). The informed consent was waived by the board because of its retrospective nature.
RESULTS
A total of 46 twin pregnant women with TTTS were underwent the fetoscopic laser ablation during the study period. Table 1 shows the outcome of fetoscopic laser ablation. The mean gestational age at procedure was 20.46 weeks, and the overall fetal survival immediate after fetoscopic laser ablation (< 48 hours) was 67.4%: dual fetal survival rate was 47.8% and at least one fetus survival rate is 87.0%. The mean gestation age at delivery was 29.63 weeks, and the overall neonatal survival rate to 28 days of life after delivery was 57.5%. The neonatal survival of least one infant was achieved in 72.5% and dual survival was noted as 42.5%.
Table 1
Outcomes of 57 cases of TTTS after fetoscopic laser ablation

Data are presented as mean ± standard deviation or number (%).
TTTS = twin-twin transfusion syndrome, GA = gestational age, FDIU = fetal death in utero.
aAmong 10 cases, 5 cases are excluded due to follow-up loss, 5 cases are excluded due to on-going pregnancy; bData for both fetuses are included in 47 cases, data for only one fetus are included in 2 cases.
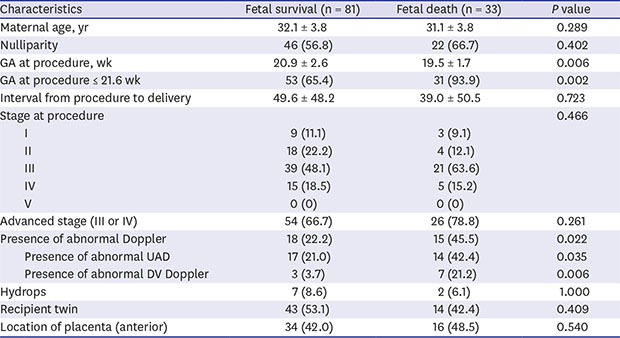
Table 2 compares the clinical characteristics and ultrasound findings according to the fetal survival or death immediate after the procedure. Fetuses who survived immediate after procedure had higher gestational age at procedure and lower frequency of abnormal Doppler studies than those did not survive. Cutoff value of gestational age for prediction of fetal death was derived from the ROC curves (area under the ROC curve 0.663; 95% confidence interval [CI], 0.562–0.765), and the gestational age at procedure ≤ 21.6 weeks was significantly associated with the risk of fetal death. However, the frequency of hydrops was not different between cases with fetal survival and fetal death. Cases with fetal survival had lower frequency of advanced stage (Quintero stage III or IV) than cases with fetal death, but this difference did not reach statistical significance.
Table 2
Clinical characteristics according to the fetal survival immediate after procedure (within 48 hours after operation)
In multivariate analysis, the risk of fetal death immediate after procedure increased with abnormal Doppler findings (odds ratio [OR], 2.838; 95% CI, 1.137–7.085; P = 0.025) and lower gestational age at procedure (≤ 21.6 weeks; OR, 8.185; 95% CI, 1.789–37.451; P = 0.007) (Table 3).
Table 3
Logistic regression for fetal death immediate after procedure

| Characteristics | OR | 95% CI | P value |
|---|---|---|---|
| GA at operation ≤ 21.6 wk | 8.185 | 1.789–37.451 | 0.007 |
| Abnormal Doppler | 2.838 | 1.137–7.085 | 0.025 |
| Hydrops | 0.754 | 0.136–4.193 | 0.747 |
Out of 33 fetuses with abnormal Doppler findings, 4 fetuses were recipient twins and 29 fetuses were donor twins. The survival rate of these fetuses was similar (55.2% in donor twin [16/29]; 50% in recipient twin [2/4]; P = 1.000).
Table 4 compares clinical characteristics and ultrasound findings between cases with at least one fetal survival and cases with double fetal death (per pregnancy). Cases with double fetal death had earlier gestational age at procedure and higher frequency of abnormal Doppler in at least one fetus. However, these differences did not reach statistical significance, probably because of small number of cases.
Table 4
Clinical characteristics per pregnancy according to the fetal survival immediate after procedure (within 48 hours after operation)
Table 5 showed complications associated with fetoscopy laser ablation. Most significant complications were intraoperative bleeding which prevents further treatment and endanger the fetuses and immediate preterm premature rupture of membranes (PPROM) which is an important cause of preterm delivery and affects fetal survival.
Table 5
Complications after the procedure

DISCUSSION
The principal findings of the current study are: 1) after fetoscopic laser ablation, the overall fetal survival immediate after procedure was 67.4% (62/92) and overall neonatal survival rate to 28 days of life after delivery was 57.5%; 2) fetuses who survived immediate after procedure had higher gestational age at procedure and lower frequency of abnormal Doppler studies than those did not survive; 3) the frequency of hydrops was not different between cases with fetal survival and those with fetal death.
In the literature, this study is the first study from Korea regarding TTTS cases treated with fetoscopic laser ablation. The fetal survival rate immediate after the procedure (at least 1 survival rate of 87%) and neonatal survival rate (at least one survival rate of 73%) are comparable to other studies in several other countries (75%–88% of at least one fetal survival and 58%–86% of at least one neonatal survival) (Table 6).578910111213141516171819
Table 6
Comparison of fetal survival outcomes after fetoscopic laser ablation in a single center
| Variables | Total No. | Immediate post-procedure (within 48 hr after procedure) | Survival after birth (within 28 days after birth) | ||||
|---|---|---|---|---|---|---|---|
| Total survival | Dual survival | At least 1 survivor | Total survival | Dual survival | At least 1 survivor | ||
| Cincotta et al.7 | 100 | - | - | - | - | 66 | 85 |
| Morris et al.8 | 164 | - | - | - | - | 38 | 85 |
| Yang et al.9 | 30 | - | - | - | - | 60 | 83 |
| Rustico et al.10 | 150 | - | - | - | - | 41 | 74 |
| Chang et al.5 | 44 | - | - | - | - | 50 | 80 |
| Ek et al.11 | 66 | - | - | - | - | 48a | 76a |
| Halvorsen et al.12 | 142 | 80 | - | - | 47b | - | - |
| Stirnemann et al.13 | 507 | - | - | - | - | 46 | 78 |
| Teoh et al.14 | 49 | - | - | - | - | 51 | 86 |
| Baschat et al.15 | 147 | - | 60 | 88 | - | - | - |
| Peeters et al.16 | 340 | - | - | - | 77 | 59 | 86 |
| Has et al.17 | 85 | - | - | - | - | 26 | 58 |
| Müllers et al.18 | 105 | - | 47 | 75 | - | - | - |
| Diehl et al.19 | 1,019 | - | - | - | - | 63 | 87 |
| This research, 2017 | 57 | 69 | 53 | 87 | 57 | 48 | 70 |
According to previous reports, neonatal survival after fetoscopic laser ablation can be affected by several factors including the presence of abnormal Doppler finding or hydrops, presence of associated abnormalities, the technical skill of operator, and location of placenta,51718202122 and these prognostic factors might be used when counseling the result of fetoscopic laser ablation. However, there are several factors considered in the interpretation of these results. First, the neonatal death may not be attributed to fetoscopic laser ablation alone, because many factors such as fetal growth restriction, preterm labor or PPROM, and even postoperative complications such as recurrent TTTS or twin anemia polycythemia sequence. Second, identification of high risk patients for fetal death immediate after fetoscopic laser ablation is another clinically important issue, because these patients may be candidates for other treatment modalities for TTTS. However, to our knowledge, there is a paucity of information on the prognostic factors which are associated with intra-uterine fetal death immediate after the fetoscopic laser ablation, although this is another essential point in clinical practice. Although the result of this study does not provide new guidelines for determining the procedure, the prognostic factors affecting the survival rate immediately after procedure can be used in patient counseling regarding the prognosis after procedure.
Among clinical factors related to neonatal survival rate (such as gestational age, Quintero stage, Doppler abnormalities, associated fetal anomalies, ultrasonographic abnormalities, experience of the practitioner, and placental location), only gestational age and abnormal Doppler finding were related to fetal survival immediate after procedure. Why are these determining factors for fetal death immediate after the procedure? Early gestational age at operation usually means early onset TTTS, which might be associated with larger volume of inter-twin communication, and the abrupt interruption of that communication may result in adjustment failure after the procedure. The presence of abnormal Doppler studies means cardiovascular burden to fetuses, which can result in the poor prognosis of fetal outcomes. However, the presence of hydrops was not associated with the risk of fetal death after the procedure. Hydrops was usually present in recipient twin, but recipient itself was associated with better survival than donor twin.1723
In conclusion, the fetal survival immediate after procedure in TTTS can be affected by the gestational age at procedure and the presence of abnormal Doppler studies.
 XML Download
XML Download