

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tenosynovial giant cell tumor (TS-GCT), also known as giant cell tumor of the tendon sheath or pigmented villonodular synovitis is a benign lesion of the tendon sheath, bursae, and synovium (1). Extraarticular TS-GCT is commonly located in the tendon sheath, bursa, and periarticular soft tissues; however, on rare occasions, it may be located in other regions with no association with the synovial tissues, making diagnosis a challenging task (2). The occurrence of TS-GCT in the retropharynx is a very rare case. In the literature, the presence of TS-GCT in the retropharynx has been reported in only one case (3).
In this report, we describe a rare case of TS-GCT in the retropharynx, which was initially misdiagnosed as oropharyngeal cancer.
CASE REPORT
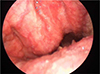
A 70-year-old man visited the otorhinolaryngology department because of an accidentally discovered mass in the right posterior oropharynx. On laryngoscopy, a bulging mass with smooth margins was observed on the posterior oropharyngeal wall (Fig. 1). For further evaluation, computed tomography (CT) and magnetic resonance imaging (MRI) scans were performed. The CT scan depicted a heterogeneously enhancing mass with smooth margins in the right retropharyngeal space at the level of C2. Posteriorly, the mass appeared to have eroded the anterior portion of the C2 vertebral body and odontoid process and was abutting with the inferior margin of the anterior atlantoaxial (AA) joint (Fig. 2). An MR image of the oropharynx depicted a mass with hypointense signal intensity on T1- and T2-weighted imaging and heterogeneous enhancement on enhanced T1-weighted imaging (Fig. 3). As a result, the lesion was diagnosed as oropharyngeal cancer.
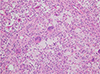
The patient underwent partial excisional biopsy via an intraoral approach. A histopathological examination revealed numerous foamy histiocytes and scattered multinucleated giant cells, suggestive of a diffuse type tenosynovial giant cell tumor (Fig. 4). On immunohistochemical study, the lesion exhibited expression of CD68 and CD45.
The patient did not undergo complete surgical excision and continued treatment with monoclonal antibodies (denosumab) for a year. On follow-up enhanced CT scan, the size of the mass was slightly decreased.
DISCUSSION
TS-GCT, also known as pigmented villonodular synovitis, is a benign soft tissue tumor that arises from the synovium of the joint, bursa, and tendon sheath (12).
TS-GCT can be classified as localized and diffuse types, based on the pattern of growth, and as intraarticular and extraarticular types, based on the location. The intraarticular type is more common than the extraarticular type. In our case, as the mass was abutting with the inferior border of the atlantoaxial joint, the intraarticular TS-GCT with the extraarticular extension was considered. However, as the center of the mass was in the anterior aspect of the joint and virtually did not involve the joint, the probability was towards the extraarticular type than the intraarticular type with extraarticular extension.
The extraarticular type of TS-GCT is of rare occurrence and was first described by Jaffe et al. (4); it is commonly localized and exhibits a benign clinical course. As it arises from the tendon sheath, it is also called as ‘the GCT of the tendon sheath’ (2).
The diffuse type TS-GCT is classified as a ‘fibrohistiocytic tumor’ in the World Health Organization system of classification of bone and soft-tissue tumors, 2013. Unlike the localized type, diffuse type TS-GCT is usually aggressive and often shows multiple recurrences (2).
On imaging, the extraarticular diffuse type TS-GCT is commonly located in the periarticular soft tissues with the involvement of adjacent joints, but on rare occasions, it can be characterized by the presence of an infiltrative soft tissue mass, without the involvement of the adjacent joint (25).
In most of the reports, extraarticular diffuse type TS-GCT is demonstrated as an ill-defined and infiltrative mass; however, it may also present as a well-defined mass, as in the present case. Unlike localized TS-GCT, the diffuse type is more frequently invasive to the adjacent soft tissue and bone (6).
On T1- and T2-weighted MR images, TS-GCT predominantly exhibits low signal intensity, reflective of hemosiderin deposition (27), but it may also show variable signal intensities, depending on the composition of the lesion and the relative proportion of hemosiderin, lipid, fibrous tissue, cyst formation, and cellular elements (1).
Pathologically, the extraarticular variant typically lacks a villous pattern. Grossly, a multifocal alternative pattern of white, yellowish and brownish lesions is common. Microscopically, TS-GCT is composed of proliferative synovial-like mononuclear cells, multinucleated giant cells, compact fibrous stromal cells, foamy and hemosiderin-laden cells etc. (46).
Diffuse type TS-GCT is composed of a striking vascularization pattern with thin-walled, slit-like, and partially hyalinized small blood vessels, including giant hemosiderin granules. Immunohistochemical analysis has revealed the expression of CD 68, CD3, and calretinin in diffuse-type TS-GCT (58).
Until date, only one case of extraarticular diffuse type TS-GCT in the retropharyngeal space has been reported and it involved the retropharyngeal space from the posterior pharyngeal wall to the level of the epiglottis. Total tumor excision and postoperative radiation therapy were performed, and no recurrence was observed (3).
Because of its rarity, extraarticular diffuse type TS-GCT is often not included among the differential diagnoses, and the lesion may often be misdiagnosed. In our case, TS-GCT was not considered during imaging evaluation (6).
The recommended treatment for TS-GCT is complete resection if possible because of the aggressive nature (9). For recurrent or unresectable lesions, moderate-dose adjuvant radiotherapy could provide good local control. However, recently, monoclonal antibodies such as imatinib, having activity against CSF1 receptor, have been used for treating TS-GCT in patients with recurrent or inoperable lesions (710). Most of the tumors appear to be clonal, neoplastic proliferations driven by CSF1 production of the neoplastic cells. They could be treated by a tyrosine kinase receptor inhibitor, such as imatinib thus demonstrating early success in the treatment (6).
In conclusion, tenosynovial giant cell tumor can involve extremely rare locations, like the retropharynx. In such cases, TS-GCT is often not included among the differential diagnoses because of the rarity of its occurrence. However, extraarticular diffuse type TS-GCT should be considered in the differential diagnosis of lesions that show low signal intensity appropriate for a giant cell tumor.


 XML Download
XML Download