

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Eperisone hydrochloride (4′-ethyl-2-methyl-3-piperidinopropiophenone hydrochloride) is a centrally acting oral muscle relaxant used for painful muscle spasm and spasticity associated with musculoskeletal disorders. It directly acts on the motor nerve to hyperpolarize the action potential, resulting in reduction of nerve conduction and sensitivity of the muscle spindle contraction.1 Eperisone yields not only muscle relaxation, but also analgesic effects by inhibiting the release of substance P.2 In addition, it has a vasodilator effect through a calcium antagonist and sympatho-suppressive action that leads to improved muscular blood flow.34
In previous double-blind randomized studies using eperisone, only gastrointestinal symptoms were reported as adverse reactions, and no allergic reactions were reported.356 In a recent systematic literature review paper, neither hypersensitive reaction nor anaphylaxis was reported after use of eperisone.7
For effective pain control, nonsteroidal anti-inflammatory drugs (NSAIDs), paracetamol, and centrally acting muscle relaxants such as eperisone are prescribed concomitantly.6 NSAIDs are well-known to induced adverse drug reactions (ADRs) and are considered a culprit drug ahead of others when hypersensitivity reaction occurs with multiple drugs. Therefore, centrally acting muscle relaxants have been overlooked as a cause of ADR. In this study, we analyzed the incidence, clinical manifestations and immunologic mechanisms of eperisone-induced ADRs, particularly anaphylaxis.
MATERIALS AND METHODS
Subjects
Pharmacovigilance data of eperisone were collected from the Korea Institute of Drug Safety-Korea Adverse Event Reporting System (KIDS-KAERS) database of the Korea Institute of Drug Safety and Risk Management (Ministry of Food and Drug Safety). Data on ADRs nationwide reported by doctors, nurses, pharmacists, pharmaceutical employers and patients are all collected in this system.8 The KIDS-KAERS database provides information on age, sex, reporting personnel, generic name of the drug, administration day/dose/route, clinical manifestations/severity, re-challenge and causality criteria. It uses the Anatomical Therapeutic Chemical Classification System for drug name, World Health Organization (WHO)-Adverse Reaction Terminology for clinical manifestations and World Health Organization-Uppsala Monitoring Center (WHO-UMC) causality criteria for assessment.9 ADR reports from January 2010 to December 2015 were analyzed. From this database, cases in which eperisone was reported only as a suspected drug and not as concomitant medication were used for the analysis. Cases in which causal relationship was assessed as certain or probable/likely were selected.
For a more accurate analysis of hypersensitivity, all reports were reviewed and revalidated if they were indeed anaphylaxis according to the WHO diagnostic criteria.10 Reviews were doctors who certified with a subspecialty in allergy. They had a minimum of 7 years of experience in the pharmacovigilance field. To overcome the limited medical information of anonymously converted computerized database, Severance Hospital (Seoul, Korea) pharmacovigilance data from January 2010 to December 2017 were analyzed for a more detailed investigation. This tertiary teaching hospital in Yonsei University operates a well-established pharmacovigilance system, and drug allergy tests (e.g., skin test, patch test, serum-specific immunoglobulin E (IgE) test, tryptase, provocation test and basophil activation test [BAT]) are available. Past medical history, drug history and underlying conditions for the use of eperisone were thoroughly reviewed. The study design schematic is shown in Fig. 1. This study was approved by the Institutional Review Board of the Yonsei University Health System (No. 2018-0770-001).

Skin prick test (SPT)
Eperisone (Exoperin®; Hanmi Pharmaceutical, Seoul, Korea) dissolved in normal saline to a concentration of 10 mg/mL was used for SPT. Normal saline with 0.3% phenol and 50% glycerol was used as the negative control, and 0.1% histamine (Allergy Therapeutics, Worthing, UK) was used as the positive control. All participants discontinued medications that might influence the test result. Wheal and erythema sizes were measured after 15 minutes, and wheal sizes greater than 3 mm were considered positive reactions. As eperisone is only available in oral tablet form in Korea, intradermal test was not performed in this study considering the patients' safety.
Oral provocation test (OPT) and tryptase
Patients requiring oral challenge were admitted to the hospital for close monitoring of adverse reactions. Open challenge OPT was performed using medications suspected to induce anaphylaxis. Eperisone provocation test was started with 5 mg (1/10 of once dose) or 10 mg (1/5 of once dose) according to previous anaphylactic reactions, increased to 10, 25 and 50 mg per hour. OPT was conducted under the supervision of an allergy specialist, and the test was stopped immediately if an allergic reaction occurred. The tryptase level was checked using fluoroenzymeimmunoassay kits (Thermo Fisher Scientific Inc., Waltham, MA, USA) in cases of anaphylaxis.
BAT
Fresh whole blood from patients allergic to eperisone was collected in EDTA vacutainer tubes (BD Biosciences, San José, CA, USA), and BAT was performed with the FlowCAST® kit (BÜHLMANN, Schönenbuch, Switzerland) according to the manufacturer's protocol. Briefly, 50 μL of the patient's whole blood was treated with various concentrations of eperisone (1, 0.1, 0.01 and 0.001 mg/mL),11 positive controls (FcεRI Ab, fMLP), and background control in 100 μL of stimulation buffer and staining reagent for 15 minutes at 37°C. For the cellular lysis, 2 mL of lysing reagent was incubated for 15 minutes at 37°C. Then, samples were centrifuged, the supernatant was decanted, and the cell pellet was resuspended with 300 μL of wash buffer. Flow cytometric analysis was performed via FACS Verse (BD Biosciences). Data were analyzed using FlowJo software (TreeStar, Ashland, OR, USA). Stimulation index (SI) was calculated as follows:
SI = % of basophil activated by the drug/% of activated basophils in the negative control
If SI was 2 or more and activated basophils were increased by more than 5%, the basophil test was regarded as positive.
RESULTS
Characteristics of eperisone-induced anaphylaxis from the KIDS-KAERS database
There were 2,213 patients who had eperisone-induced ADRs. Among them, 207 whose ADRs were considered to have causal relationships (certain or probable/likely relationship based on the WHO-UMC criteria) were selected for analysis (Supplementary Table S1). The most common ADRs were cutaneous hypersensitive reactions (30.4%) such as urticaria, itchiness and angioedema. Anaphylaxis, a systemic hypersensitive reaction, developed in 16.9% of the patients (n = 35, Supplementary Table S2).
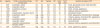
Information about the patients with eperisone anaphylaxis is shown in Table 1. The mean age was 50.6 years, and majority was women. Doctors reported the most number of anaphylaxis cases (48.6%) than other medical personnel. A total of 70% of enrolled cases were rated as “certain” in the causal relationship evaluation. Re-challenge information was available in 20 patients, and 70% of them re-experienced ADRs.
Table 1
Characteristics of eperisone-induced anaphylactic patients in the KIDS-KAERS database (n = 35)

Values are presented as mean ± standard deviation or number (%).
KIDS-KAERS, Korea Institute of Drug Safety-Korea Adverse Event Reporting System; M, male; F, female; WHO-UMC, World Health Organization-Uppsala Monitoring Center; NA, not available.
*Among 35 patients with anaphylaxis, 26 were originally reported as anaphylactic.
![]()
Among the 35 patients with anaphylaxis, 26 (74.3%) were originally reported to have anaphylaxis and 9 were newly re-assessed to have anaphylaxis based on the WHO criteria. Respiratory (e.g., dyspnea and wheezing) and cardiovascular compromises were observed in 45.7% and 20% of the patients, respectively. Meanwhile, 2.7% of the patients experienced altered mental status.
Clinical characteristics and allergy tests of patients with eperisone-induced anaphylaxis from a single center
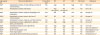
The baseline characteristics of patients with eperisone-induced ADR at a single pharmacovigilance center are shown in Supplementary Table S3 (n = 37). The mean age was 56.5 years, and majority was women (64.9%). In this center, cutaneous manifestations (29.7%) and anaphylaxis (29.7%) were the most common ADRs. There were 11 patients who experienced eperisone-induced anaphylaxis. The demographics, co-administered medications and results of the allergy diagnostic study are shown in Table 2. The average age was 53.9 years, and women were 2.7 times more likely to develop ADRs than men. Most patients were prescribed with eperisone due to muscle cramping (63.6%), and there were no patients who had any other allergic diseases. Eperisone was co-administered with NSAIDs, tramadol, acetaminophen or gastrointestinal protective agents.
Table 2
Characteristics and allergy test results eperisone anaphylactic patients in a single pharmacovigilance center (n = 11)
M, male; F, female; SPT, skin prick test; BAT, basophil activation test; OPT, oral provocation test; ND, not done; Neg, negative reaction; Pos, positive reaction.
*Cumulative dose for positive reaction during OPT; †Onset time of positive reaction during OPT; ‡Others are gastrointestinal protective drugs such as rebamipide, almagate, or ranitidine.
![]()
Allergy screening test to determine the cause was performed using SPT, BAT and open challenge test. All the patients with anaphylaxis showed a positive reaction to OPT using eperisone. SPT of eperisone was performed in 4 patients, and all results were negative. BAT data of the 4 patients are shown in Supplementary Fig. S1A. None of the patients met the BAT positivity criteria described earlier. Tryptase levels were checked in 3 patients after anaphylaxis developed. One had elevated absolute levels (15.5 μg/L, reference range: 0-13.5 μg/L), the other had a 7.7-fold elevation baseline tryptase (from 1.11 to 8.53 μg/L, measured after provocation test), while the other had no changes in tryptase levels. During OPT, 5 patients experienced hypotension, and 7 patients showed urticaria and/or angioedema (Supplementary Fig. S1B). Cumulative dose for positive reaction was 5 to 50 mg of eperisone. On average, 59 minutes were taken for a positive reaction.
As other pain controllers such as NSAIDs are co-administered with eperisone, and they are more commonly known as the cause of drug allergy than eperisone, open challenge test using pain controllers were performed initially. However, all OPTs were negative for pain controllers. Therefore, eperisone was suspected to be the cause of anaphylaxis and OPT was performed.
DISCUSSION
In this study, we analyzed the nationwide incidence of eperisone-induced anaphylaxis including overall ADRs for the first time. In addition, SPT, OPT and BAT12 were performed to determine the mechanism of anaphylaxis. Several case reports of eperisone-induced anaphylaxis and ADRs have been published to date. The signs and symptoms of anaphylaxis and results of the diagnostic tests are summarized in Table 3.
Table 3
Previous studies on eperisone-induced ADRs including anaphylaxis
| Age (year)/sex | Clinical manifestations | Provocation test | SPT | IDT | BAT | Patch test | Reference |
|---|---|---|---|---|---|---|---|
| 64/F | Anaphylaxis (urticaria, throat swelling, and loss of consciousness) | Pos | Neg | ND | Neg | ND | Miki et al.11 |
| 70/F | Anaphylaxis (urticaria and shock) | Pos | Neg (10 mg/mL) | Pos (10 mg/mL) | ND | ND | Kim et al.15 |
| 63/F | Anaphylaxis (urticaria, dyspnea, dysphagia, and chest pain) | Pos | ND | ND | ND | ND | Kang et al.1 |
| 58/M | Anaphylaxis (urticaria, shock, and loss of consciousness) | Pos* | ND | ND | ND | ND | Kang et al.1 |
| 58/M | Anaphylaxis (urticaria, dyspnea, and facial edema) | Pos | ND | ND | ND | ND | Kang et al.1 |
| 54/F | Anaphylaxis (urticaria, angioedema, dyspnea, shock, and dizziness) | ND | Neg | Neg | ND | ND | Hur et al.16 |
| 62/F | Anaphylaxis (dyspnea and angioedema) | ND | Neg | Neg | ND | ND | Hur et al.16 |
| 23/M | Drug eruption | Pos | NA | NA | NA | NA | Ueno and Kawana.22 |
| 30/M | Severe maculopapular rash | ND | ND | ND | ND | ND | Balaraddiyavar et al.23 |
| 42/F | Fixed drug eruption | Pos | ND | ND | ND | ND | Choonhakarn24 |
| 69/F | Acute generalized exanthematous pustulosis | ND | ND | ND | ND | Pos | Yamamoto et al.25 |
ADR, adverse drug reaction; M, male; F, female; SPT, skin prick test; IDT, intradermal test; BAT, basophil activation test; Neg, negative reaction; Pos, positive reaction; ND, not done; NA, not available (published in Japanese except abstract).
*Confirmed by history: 3 times re-challenge.
![]()
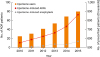
A previous case series reported the highest number of patients with eperisone anaphylaxis in the Korean population. Eperisone is not available as an over-the-counter drug in Korea. To calculate the annual rate of eperisone-induced anaphylaxis, we collected nationwide prescription data from 2010 to 2015. The prescription of eperisone has increased by 44% from 2010 to 2015. In proportion to this increase, the number of reported ADRs also increased by 564% (Fig. 2). In 2015, 901,255 patients were prescribed with eperisone, and 73 cases of ADR, were reported, among which 14 were anaphylactic (calculated incidence: 0.001%). This shows that aside form NSAIDs, eperisone should also be regarded as a cause of anaphylaxis in patients receiving musculoskeletal pain control medications. Eperisone is considered to cause ADRs independent of any other co-administered drugs. In drug interaction studies, there was no known pharmacokinetic interaction between eperisone and aceclofenac13 and pelubiprofen.14
The findings of this study suggest that eperisone-induced anaphylaxis occurs through a non-IgE mechanism. SPT and BAT were negative in this study. In previous reports, SPT yielded negative reactions,111516 and only 1 case of positive intradermal test reaction has been reported.15 However, this study did not indicate a non-irritating concentration of intradermal test. BAT was performed only in one previous study, which also yielded negative reaction.11 Collectively, these results indicate that eperisone-induced anaphylaxis can only be diagnosed through OPT.
In addition to anaphylaxis, drug eruption, severe maculopapular rash, fixed drug eruptions and acute generalized exanthematous pustulosis have been reported as ADRs to eperisone (Table 3). Moreover, aside from hypersensitive reactions, there were also several case reports on toxic reactions after administration of high-dose eperisone. An 18-month-old child lost consciousness and had seizure, apnea and ventricular tachycardia after accidentally taking 100 mg of eperisone hydrochloride, which is equal to at least 1,000 to 2,000 mg eperisone in adults.17 There were toxicity reports of QT prolongation,18 torsades de pointes induced by severe QT prolongation after eperisone overdose and suicide attempt after taking triazolam combined with eperisone.19
In a previous efficacy and safety study, 7 of the 100 patients who received 300 mg per/day of eperisone reported ADRs of light-headedness (n = 1), vertigo and/or loss of equilibrium (n = 3), mild somnolence (n = 2), and epigastric pain (n = 1).20 Patients who received eperisone showed similar or lesser ADRs compared with those who received other pain relievers in a dose-ranging study. Eperisone 300 mg/day was effective and well-tolerated (cumulative ADR incidence: 11.1%) compared with the placebo (cumulative ADR incidence: 16.7%).3 In a comparison study between eperisone and thiocolchicoside, the number of subjects who reported ADRs (nausea, epigastric discomfort and vomiting) was lower in the eperisone-treated group (5%) than in the thiocolchicoside-treated group (21.3%).6 In another efficacy and safety study comparing eperisone and baclofen, the eperisone-treated group showed better tolerability (47.4% patients had ADR) than the baclofen-treated group (77.1% patients had ADR).2
There is no evidence to suggest a cross-reactivity between eperisone and any other drugs. However, eperisone is closely related to tolperisone hydrochloride (dimethyl-2,4′-piperidino-3-propiophenone) as their chemical structures are quite similar. A study suggested that cross-reactivity of eperisone with tolperisone can also cause anaphylaxis.21 Chemical structures of eperisone and related compounds are shown in Fig. 3.

In this study, there are some limitations. First, this study analyzed the self-reported ADRs from heterogeneous reported personnel retrospectively. The nature of the voluntary reporting database implies several limitations such as under-reporting and lack of central quality control by expert panel. Since ADR reports of KIDS-KARES database were anonymized, additional information could not be assessed. As such, it was impossible to determine if the 11 single-center patients were included in the KIDS-KAERS. Secondly, a limited number of patients agreed to participate in the SPT and BAT. Most patients could find culprit drug after multiple OPTs, and then refused an additional SPT or BAT test. Thirdly, the possibility that eperisone metabolites causes IgE-mediated reaction could not be verified in this study. If eperisone metabolite is a culprit, SPT and BAT using eperisone itself can be negative.
In conclusion, eperisone induces anaphylaxis possibly by inducing non-IgE-mediated immediate hypersensitivity. Thus, it should be considered a cause of anaphylaxis in pain medications. The OPT under supervision of an allergy specialist appears to be the optimal diagnostic modality for eperisone-induced anaphylaxis.
 XML Download
XML Download