

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Plantar pain caused by dermatological condition is often associated with plantar epidermal cyst, hemorrhagic corn or callus, plantar fibromatosis, or plantar verruca1. Among laborers, they may develop from excess pressure on the bony prominences of the feet, repetitive uneven friction from footwear, or gait abnormalities. Plantar vein thrombosis is a rare condition causing plantar pain. The exact cause of plantar vein thrombosis is yet unclear, but predisposing conditions, such as prior trauma, surgery, paraneoplastic syndromes, or coagulation disorders have been described. To date, there is no established treatment except surgical excision, but reportedly, nonsteroidal anti-inflammatory drug or heparin with elastic bandage is known to be effective for symptomatic control2345. To the best of our knowledge, this is the typical case of an isolated plantar vein thrombosis resembling a corn or verruca with a bruise, which showed improvement after surgical excision, in a man working as a freight car driver. We received the patient's consent form about publishing all photographic materials.
CASE REPORT
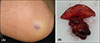
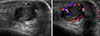
A 52-year-old man working as a freight car driver presented to our clinic with a tender nodule on his right sole toward the heel, which developed 4 years ago and got bigger. He thought it was a corn and applied some keratolytic agents, with which it failed to improve. Physical examination revealed a walnut-sized, firm, fixed subcutaneous nodule with an overlying fine violaceous hyperkeratotic plaque on the heel side of the right plantar area (Fig. 1A). Clinically, he was diagnosed as having a corn or verruca associated with a neighboring bruise. Sonography was performed to rule out the presence of an underlying subcutaneous tumor, and revealed a 1.9×1.2 cm sized, well-demarcated, lobulated heterogeneous hypoechoic mass surrounded by a thin anechoic area with increased peripheral vascularity (Fig. 2). The radiologist suggested an inflamed epidermal cyst. Surgical excision was performed for complete removal of the superficial corn and the subcutaneous tumor, to relieve his plantar tenderness. A dark erythematous rubbery nodule, 2 cm in diameter, was found in the subcutaneous layer (Fig. 1B). There was minimal intraoperative bleeding. Histopathological examination revealed several variable thick and plicated walled small muscular vessels and hemosiderin deposition within and around them in focal areas of the dermis. The subcutaneous layer showed a large vessel whose lumen was blocked by a thrombus consisting of aggregated erythrocytes and eosinophilic fibrin (Fig. 3A). The violaceous bruise-like macule around the nodule was turned out dermal deposits of hemosiderin (Fig. 3B). Based on these findings, he was diagnosed as having an isolated plantar vein thrombosis. Sutures were removed 2 weeks later, and he had no recurrence during 6-month follow up.
DISCUSSION
Plantar vein thrombosis was first reported in 1997 by Legrand et al.6 in a patient developing this condition after a saphenectomy. The exact etiology is yet unknown, but reportedly, it has been associated with trauma or athletic activity2, postsurgical immobilization56, coagulation disorders such as anticardiolipin syndrome4 or prothrombin G20210A mutation3 and paraneoplastic syndromes in a patient with bone metastasis2. Our case was not associated with prior surgery, malignancy, or coagulation disorders and might have been caused by repetitive trauma because as a freight car driver, he was known to have carried heavy loads.
Long-standing subcutaneous venous thrombosis might cause both tender subcutaneous mass and surface hyperkeratosis of the epidermis, which makes diagnosis more difficult. It should be differentiated from other dermatological conditions causing plantar pain such as hemorrhagic corn or callus, plantar epidermal cyst, plantar fibromatosis, and plantar verruca1. A corn or callus is the localized focus of hyperkeratosis, arising on the plantar portion from foot deformity or pressure, and the accompanying pain is usually relieved by paring it or applying keratolytic agent7. Plantar warts appear as horny plugs surrounded by a ring of hyperkeratotic skin with slight elevation7. They also revealed homogeneous black to red dots and globules with papilliform surfaces more prominently seen via dermoscopy8. In the case of plantar epidermoid cyst, there is a tiny blackhead plugging the central punctum of the cyst and sometimes foul smelling cheesy debris drains from it9. Typically, plantar fibromatosis presents along the central or medial aspect of the plantar fascia as a firm, fixed, rather deep subcutaneous nodule10.
To make a proper diagnosis, radiological studies of the lesion may be essential. Plantar vein thrombosis can be diagnosed with Doppler sonography or magnetic resonance imaging (MRI). On Doppler sonography, it characteristically appears as hypoechoic, dilated, noncompressible vessels with no luminal blood flow2. However, being operator dependent, a diagnosis might be missed, and MRI is preferred for evaluating persistent foot pain11. The typical MRI finding is intraluminal filling defect in plantar veins in association with perivenular enhancement12. On the other hand, plantar fibromatosis shows ill-defined, infiltrative mass occurring in the deep aponeurosis adjacent to the plantar muscles with heterogeneous signal intensity equal to or less than that of skeletal muscle on both T1- and T2-weighted MRI10. Unruptured epidermal inclusion cysts have intermediated to slightly increased signal intensity on T1-weighted images and high signal intensity on T2-weighted/fluid-sensitive sequences13. Finally, biopsy, preferentially excisional one, can help confirm the diagnosis. We removed the thrombosed vein surgically with minimal intraoperative bleeding and the patient had a 6-month follow up without recurrence. Therefore, surgical excision should be considered as a treatment option for plantar vein thrombosis.
In conclusion, plantar vein thrombosis is one of the rare dermatologic diseases causing plantar pain. This is the case that looked like a corn associated with a bruise, perhaps due to its long-standing nature and hemosiderin deposition. When dermatologists encounter patients with painful plantar subcutaneous mass, multiple disorders should be considered in the differential diagnosis. Radiological studies or skin biopsy can be a useful tool for the diagnosis.

 XML Download
XML Download