

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Dear Editor:
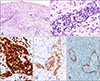
The presence of atypical large lymphoid cells within vascular spaces is an uncommon finding in the skin and suggests intravascular lymphoma (IVL)1. We present a rare case of benign atypical intralymphatic CD30+ T-cell proliferation, that mimicked IVL, along with a review of the literature. A 69-year-old man presented with confusion. Magnetic resonance imaging identified a 2.5 cm mass in left temporoparietal lobe of brain. He was diagnosed with primary diffuse large B-cell lymphoma (DLBL) of the central nerve system (CNS) and underwent chemotherapy with methotrexate and cytarabine. On the second day of chemotherapy, a 0.7 well demarcated ulcer was found on the penile shaft and a punch biopsy was performed (Fig. 1A). Microscopically, the epidermis showed ulceration and superficial dermis contained thin-walled dilated lymphatic vessels, some of which were filled with atypical lymphoid cells (Fig. 2A). The lymphoid cells were medium- to-large with pleomorphic nuclei with prominent small nucleoli (Fig. 2B). These cells were positive for CD3 (Fig. 2C) and CD30 (Fig. 2D), but negative for CD20, CD56, and anaplastic lymphoma kinase (ALK). Epstein-Barr virus-encoded small RNA (EBER) in situ hybridization test was negative, and a BIOMED-2 T-cell receptor gamma gene clonality assays showed polyclonality. The lesion spontaneously regressed without any treatment after two months (Fig. 1B). We received the patient's consent form about publishing all photographic materials.
The presence of atypical lymphoid cells in vascular space suggests possible IVL. Most IVLs are of the B-cell lineage with an aggressive clinical course, and are commonly represented by DLBL and predominant intravascular growth2. Recently, there have been several reports of cutaneous intravascular CD30+ T-cell lymphoproliferative disease (CD30+ TLPD); anaplastic large cell lymphoma (ALCL) and lymphomatoid papulosis (LyP)-like TLPD3,4. Furthermore, benign proliferation of intralymphatic atypical CD30+ T-cells has also been reported1,5. Irrespective of diagnostic diversity, intralymphatic ALCL, LyP-like TLPD, and benign atypical CD30+ T-cell proliferation exhibit compatible morphologic/immunophenotypic features and a similar clinical course (Supplementary Table 1).
Intravascular ALCL presents as a single or multiple nodules and plaques (1.2~12 cm)3,4. Tumor expresses CD30, but is negative for cytotoxic markers, ALK, and EBER1. Lymphomatoid papulosis-like TLPD present multiple plaques and patches that wax and wane3. To date, only 10 cases of benign atypical intravascular CD30+ T-cell lymphoid proliferation have been reported1,5. Patients age range from 17~77 years and the lesions occur on the extremities, trunk, neck, eyelid, left inguinal, uterus polyp and prepuce. Nine cases presented as single lesion (1~3 cm), while one presented as multiple lesions with drug rash. No cases showed clinical signs of lymphoma or clonality1. Nine cases showed complete remission without recurrence after excision or biopsy1 while one underwent radiotherapy that lead to complete remission5.
Although this patient received chemotherapy for the primary CNS DLBL, but the lymphoma continued to progress. After switching to radiotherapy, the lymphoma decreased. The penile lesion regressed with no recurrence in the last 7 months.
In conclusion, we report a rare case of benign atypical intralymphatic CD30+ T-cell proliferation that mimicked IVL. Pathologist and dermatologist should be aware of this entity and its clinical features to avoid misinterpretation.

 XML Download
XML Download