

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Endometriosis is a common disease entity affecting around 10% of reproductive-age women [1]. It has a wide variety of clinical consequences ranging from benign lesions to malignant transformation [234]. In a pooled analysis of case-control studies, endometriosis was found to be significantly correlated with increased risk of epithelial ovarian cancer, especially clear cell adenocarcinoma [5]. In addition, a recent study has provided significant evidence of an association between endometriosis-related genetic variation and ovarian cancer risk, especially in those with clear cell histotypes [6]. In spite of these risks, there are still debates and disagreements as to the optimal treatment and follow-up strategies for patients with endometriosis. Although several guidelines have been developed to provide information on the diagnosis, treatment, and prevention of endometriosis, there is still a lack of evidence regarding follow-up intervals and the timing of surgical intervention especially in patients with asymptomatic endometriosis [78910]. Surgical treatment of endometriomas may confer the benefit of histological confirmation along with a protective effect against later development of ovarian cancer [711]. On the other hand, universal surgical resection of endometriomas may cause operative risk and decreased ovarian reserve [1213]. Previous studies suggested that the risk of malignant transformation of endometriosis was approximately 1% for premenopausal women and 1-2.5% for postmenopausal women [1415]. In a Japanese prospective study, malignant transformation was reported in about 46 (0.72%) of 6,398 patients with endometriosis after a median follow-up period of 12.8 years [16].
Despite the low potential for malignant transformation of endometriosis and the relatively long latent period, studies investigating the management strategies for endometriosis, especially in asymptomatic patients, are urgently needed. The aim of this study was to examine the treatment outcomes of clear cell carcinoma of the ovary in relation to endometriosis and to determine an appropriate management strategy for asymptomatic patients with endometrioma.
Materials and methods
A retrospective review of medical records was performed in patients with clear cell carcinoma of the ovary who were diagnosed and treated between 2001 and 2017 at Ajou University Hospital, Suwon, Korea. A total of 50 consecutive patients with ovarian clear cell carcinoma were identified. All the patients were evaluated with Siemens Acuson S2000 Ultrasound system (Siemens Healthcare, Ultrasound Business Unit, Mountain View, CA, USA) and computed tomographic (CT) scans to inspect the characteristics of the adnexal masses before surgery. Forty-nine patients underwent complete staging surgery, while one patient refused to undergo surgery.
After the surgery, patients received adjuvant systemic chemotherapy with paclitaxel (175 mg/m2) plus 3 to 6 cycles of carboplatin (area under the curve [AUC] of 6). Clinicopathologic characteristics including age at diagnosis, parity, body mass index (BMI), initial symptoms, maximum tumor diameter, and ovarian involvement (laterality) were analyzed. Treatment outcomes including the type of treatment, International Federation of Gynecology and Obstetrics (FIGO) stage, status of residual disease, and disease recurrences were analyzed. Recurrence was defined based on Gynecologic Cancer Intergroup criteria after evaluation using the Response Evaluation Criteria in Solid Tumors guidelines [17]. If a patient was diagnosed with endometrioma prior to surgery, the associations between endometriosis and clear cell carcinoma were analyzed, including a previous diagnosis of endometriosis and the latent period until the diagnosis of clear cell carcinoma. Statistical analysis was performed using IBM SPSS Statistics for windows (version 20.0, IBM Corp., Armonk, NY, USA). Risk factors were compared according to recurrence status using the Mann-Whitney U test for continuous data and Pearson's χ2 test or Fisher's exact test for categorical data. P-values less than 0.05 were considered statistically significant.
Results
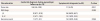
During the study period, a total of 533 patients with epithelial ovarian cancer (EOC) were identified. Clear cell carcinoma of the ovary comprised 9.3% (50/533) of the EOC. Median age at diagnosis was 49.5 (range, 25–75) years; 42 patients (42/50, 82%) were older than 40 years at the time of diagnosis, and only 2 patients were younger than 37 years in this patient cohort. The median tumor size increased with increasing patient age (Fig. 1). Most patients' symptoms were related to the mass effect of the tumor. Frequent symptoms included palpable mass (32%), abdominal distention (20%), and abdominal pain (20%). Only 11 (22%) patients were diagnosed during gynecologic evaluation and did not have any symptoms. Of the 50 patients, 40 patients (80%) had a unilateral ovarian tumor with a size greater than 8 cm. Ten (20%) patients had been diagnosed with endometrioma before the diagnosis of clear cell carcinoma. The initial diagnosis of endometrioma was made by ultrasonography. Nine of the patients self-reported the previous diagnosis of endometrioma in a local clinic, and 1 patient was diagnosed in our institution. However, not all patients had follow-up visits after the initial diagnosis of endometrioma made by ultrasonography. Histologic confirmation of endometriosis was possible in 35 (70%) patients after complete staging surgery. The median time period from the diagnosis of endometriosis to clear cell carcinoma was 50 (range, 12–213) months in the 10 patients (Table 1).
Fig. 1
(A) Number of patients diagnosed with clear cell carcinoma according to the age group. (B) Median tumor size according to the age at diagnosis of clear cell carcinoma.

Table 1
Clinicopathologic characteristics of patients with ovarian clear cell carcinoma (n=50)

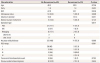
The median tumor size in the patients without and with an endometriosis background was 9.7 cm (range, 5–20) and 10.5 cm (range, 4.6–25), respectively. Presence of endometriosis on pathology was not associated with tumor size or patient age (P=0.519 and 0.451, respectively), nor was it related to the prognosis (FIGO stage, P=0.747; disease recurrence, P=0.672) (Table 2). Interestingly, among patients who had been diagnosed via routine gynecologic examination, only 1 patient experienced disease recurrence (1/11, 6.7%). Asymptomatic patients (n=11) who had regular gynecological examinations were found to have a relatively smaller tumor size, lesser extent of tumor spread, and lower recurrence rate (P=0.011, 0.283, and 0.064, respectively) (Table 3).
Table 2
Characteristics of the patients with or without endometriosis background
Table 3
Clinical stages and recurrence events during the follow-up periods in patients with ovarian clear cell carcinoma
Thirty-eight patients underwent primary debulking surgery, 3 had neoadjuvant chemotherapy with interval debulking surgery due to a comorbid condition or extensive disease burden, and 8 had re-staging surgery after unilateral ovarian cystectomy or unilateral salpingo-oophorectomy. Of the 50 patients, 35 (70%) were diagnosed with FIGO stage I or II disease. Four patients (8%) were found to have concurrent thromboembolic disease during the follow-up period. Fifteen patients experienced disease recurrence (Table 4). Among the various clinicopathologic factors, FIGO stage and the status of residual disease were the only significant factors affecting disease recurrence. A previous history of endometriosis was not a significant factor for recurrence (P=0.654) (Table 5).
Table 4
Treatment outcomes

Table 5
Risk factors for ovarian clear cell carcinoma recurrence
Discussion
According to this study, nearly three-quarters of the clear cell carcinoma cases were confirmed in the background of endometriosis. Most patients were diagnosed during their late thirties or forties with a median of 4 years until malignant change. Yet, asymptomatic patients who were diagnosed during regular gynecologic evaluations were more likely to present with a smaller tumor size and early FIGO stage. More importantly, they experienced a low rate of recurrent disease.
Considering the risk of malignant potential in endometriosis, appropriate follow-up strategies are indispensable. Previous epidemiological and molecular studies have indicated that endometriosis is the most plausible precursor of ovarian clear cell carcinoma [56181920]. In a meta-analysis of 13 case-control studies including 7,911 women with EOC, women with a self-reported history of endometriosis had three times the risk of clear cell carcinoma (odds ratio [OR], 3.05; 95% confidence interval [CI], 2.43–3.84; P<0.0001) and double the risk of endometrioid (OR, 2.04; 95% CI, 1.67–2.48; P<0.0001) and low-grade serous carcinoma (OR, 2.11, 95% CI, 1.39–3.20) [5]. In previous studies, the mechanisms of malignant transformation were suggested to be related to the activation of oncogenic KRAS and PI3K pathways and inactivation of tumor suppressor genes PTEN and ARID1A [1920]. Menopause status has also been indicated as a potential risk factor [14]. In premenopausal woman, the risk of malignant transformation of endometriosis has been estimated at around 1 percent [15]. However, there have been no age-specific guidelines for the timing of active surveillance in asymptomatic patients. Current guidelines recommend that endometriomas be removed only if they have an atypical appearance on imaging studies or other concerning features such as enlarged size in asymptomatic patients, though no information as to the timing or interval of surveillance has been provided [21].
In this patient cohort, many patients were asymptomatic until the median tumor size was about 10 cm. In addition, 80% of the patients did not receive any surveillance until the onset of symptoms, and many of them characteristically presented with a rapidly growing pelvic mass in a background of endometriosis. In a Japanese study of 33 patients with clear cell carcinoma, tumor size was found to have doubled in the 6 months prior to the diagnosis of malignant transformation in 30 patients. These patients had been followed for at least 2 years after the diagnosis of ovarian endometrioma and continued to be followed after the identification of malignant transformation [22]. In the current study, asymptomatic patients who had regular gynecologic examinations were found to have a relatively smaller tumor size with less tumor spreading. In light of the median duration (50 months; range, 12–123 months) of malignant transformation and the age of cancer incidence, surveillance should be started from the age of the mid-thirties, with at least 1-year interval surveillance in asymptomatic patients with endometriosis. Owing to the rapid growth characteristics of clear cell carcinoma, patients should be also informed as to the risk of cancer and the necessity of regular gynecologic surveillance despite a lack of symptoms. If the tumor size increases during regular follow-up, surgical treatment should be considered, since ovarian clear cell carcinoma has been known to be chemo-resistant with an extremely low chemo-response rate [2324].
The current study has some limitations. First, the retrospective nature of the study might have inevitably led to a patient or treatment selection bias. Second, since the most patients with endometriosis were diagnosed at a local clinic, we could not confirm the effectiveness of various multimodal screening tools including CA-125 and sonography. Third, other than age, the risk factors for malignant transformation were not confirmed in this study. Further large studies focusing on the risk factors and screening tools for malignant transformation are necessary. Despite these limitations, the current study has proposed a surveillance strategy for asymptomatic patients with endometriosis. Despite the overall low incidence of ovarian clear cell carcinoma, the current study had a relatively long follow-up period in a single institution. In addition, all patients were treated with the same quality of medical and surgical treatment.
In summary, early detection of malignant transformation during gynecologic evaluation and surgical intervention are directly associated with oncologic prognosis in asymptomatic endometriosis patients. For the timely detection of malignant transformation of ovarian endometrioma, at least 1-year interval surveillance and counseling should be provided, commencing in the patients' mid-thirties.
 XML Download
XML Download