

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Induced labor represents the most frequent interventional procedure in the field of obstetric medicine; it is reportedly applied in 20% to 25% of all pregnancies [12]. Induced labor is indicated in situations in which the outcomes for the mother and neonate are better if the pregnancy is not further prolonged [23].
There are potential medical advantages to scheduled induction of labor at full term, such as reduction in stillbirth and further fetal growth, which leads to macrosomia and its consequences [456]; moreover, elective labor induction can reduce the chance of sudden disruption of the patient's life and provider's work. In addition, regarding neonatal outcomes, studies have shown that an increased risk for perinatal and maternal complications was detected as early as 40 weeks of gestation [7].
However, elective induction may be associated with drawbacks such as increased length of labor, the potential for patient/provider impatience, Cesarean delivery, a long latent phase, increased cost, and neonatal morbidity if the gestational age is less than 39 weeks of gestation [38]. The Cesarean delivery rate, which is thought to be the most important and adverse outcome of labor induction, is inversely correlated with cervical favorability at induction, based on the Bishop score [910]; thus, the cervical status may represent one of the most important predictors of successful vaginal delivery when deciding to induce labor.
Some studies, however, have indicated there is no convincing evidence that elective labor induction is associated with a substantial increase in the rate of Cesarean delivery when the rate at term in electively induced women is compared to that of women at the same gestational age managed expectantly [511121314].
Furthermore, Saccone and Berghella [15] recently demonstrated that the rate of Cesarean delivery was not increased by induction at full term, even for mothers with an unfavorable cervix, and Miller et al. [16] reproduced this result by conducting a randomized, controlled trial in 2015.
The American College of Obstetricians and Gynecologists (ACOG) has stated that induced labor between 37 and 38 gestational weeks, i.e., early term, should be avoided in uncomplicated women [17]. This is because early term newborns have greater neonatal morbidity and healthcare utilization during their entire first year of life than those born at 39 to 40 weeks of gestation [181920].
A recent study showed that the overall frequency of labor induction more than doubled in the United States, increasing from 9.5% in 1990 to 23.8% in 2010 [21], and elective induction for the mother and provider’s convenience accounted for approximately 40% of cases [22]. Some authors supported induced labor at 39 weeks or more [1223]. If elective induction is considered at term, inherent risks must be discussed, informed consent must be obtained, and guidelines must be followed, as promulgated by the ACOG [24].
The purposes of this study were to critically compare the benefits and risks of labor induction versus spontaneous labor in uncomplicated singleton gestations at 39 or more weeks of gestation and to evaluate whether induction of labor at full term in low-risk women reduces the risk of composite maternal and perinatal morbidity.
Materials and methods
This study was an observational, retrospective study conducted between January 1, 2011 and November 30, 2017 at the National Health Insurance Service Ilsan Hospital in the Republic of Korea.
All women from 39 gestational weeks, 0 days to 41 gestational weeks, 6 days were considered for participation in this study. When women were at 39 gestational weeks or more in the outpatient department of the hospital (OPD), they were given the choice between waiting for spontaneous labor or inducing labor. The following inclusion criteria were used: 1) primiparous women, 2) uncomplicated living singleton pregnancy, 3) gestational age from 39 weeks, 0 days to 41 weeks, 6 days, 4) cephalic presentation, and 5) intact amniotic membrane. Women undergoing induced labor due to premature rupture of membranes, which can alter the course of labor, and women with indications for Cesarean delivery, such as placenta previa, previous Cesarean section status, or previous myomectomy were excluded. We excluded women with a myoma more than 8 cm, those with uncontrollable diabetes, or those with other severe medical diseases, such as poorly controlled gestational hypertension. Additionally, we excluded women with fetuses with intrauterine growth restriction or large-for-gestational-age fetuses.
Women in the induction group were admitted to the delivery room via the OPD. Near term, most women have Braxton-Hicks contractions, which are not painful and discovered incidentally on a non-stress test. Because Braxton-Hicks contractions are not accompanied by change in the cervix length, we did not consider them as spontaneous labor. Most women in the spontaneous labor group were admitted directly to the delivery room, or some came to the OPD with complaints of pain and regular labor. All patients were clinically evaluated by pelvic examination to determine the Bishop scores for cervical dilatation, effacement, consistency, and the position and station of the fetus [10]. These 5 components of the Bishop score were measured by 1 expert (EHK). Fetal head engagement in the maternal pelvic cavity was also assessed by pelvic examination at this time.
Next, ultrasonography was performed by 1 expert (EHK) using the Philips Ultrasound IU22 (Bothell, WA, USA) and EPIQ 7 (Bothell, WA, USA) with a vaginal probe. The probe was inserted vaginally 3 cm from the cervix, and the length between the internal and external os of the cervix in the longitudinal section was measured in accordance with previously validated technical criteria [25]. The cervical longitudinal section was defined by the view of the cervical canal, and the cervical length was defined as the shortest value based on 4 or more measurements.
Labor induction was attempted with oxytocin (intravenous injection, 10 IU/mL; Pitocin, Jeil Pharmaceutical Co. Ltd., Daegu, Korea) or prostaglandin E2 (intravaginally, 10 mg; Propess, Bukwang Pharm Co. Ltd., Seoul, Korea), and when women developed spontaneous labor pain, augmentation with oxytocin was attempted if labor progression was inadequate. Fetal heart rate was continuously monitored by cardiotocography between 30 minutes before and 1 hour after oxytocin or prostaglandin E2 administration in all women. Prostaglandin E2 was inserted vaginally and removed 12 hours after the insertion or earlier in case of onset of active labor, rupture of membranes, or abnormal cardiotocography findings (i.e., fetal hyperstimulation or other alteration in the fetal heart rate). If non-reassuring fetal heart pattern developed, we discontinued oxytocin temporarily. In the spontaneous labor group, we used oxytocin when we thought labor progression was inadequate.
From the institution's electronic medical record, we obtained the following information: data concerning the delivery mode (vaginal or Cesarean delivery), time between admission and vaginal delivery, duration of the second stage, maternal age, gestational age, change in the hemoglobin level after delivery (as a decrease implies blood loss during the delivery), and length of hospital stay. To evaluate neonatal complications, we assessed the neonatal weight, 1- and 5-minute Apgar scores, neonatal intensive care unit (NICU) admission rate, meconium status, and neonatal intubation status.
1. Statistical analyses
Demographic and clinical characteristics were compared between women with and without induced labor using Student's t-test for continuous values and the χ2 test or Fisher's exact test for categorical values. We obtained odds ratios for successful vaginal delivery using a logistic regression model. All P-values were 2-tailed, and P<0.05 was considered statistically significant. All analyses were performed using the Statistical Package for Social Sciences, version 23.0 (SPSS Inc., Chicago, IL, USA).
Results
A total of 237 women were recruited for this study; there were 73 women in the expectant group and 164 women in the induction group. Among all women, 199 (84.0%) delivered vaginally.
Table 1 summarizes demographic data and clinical outcomes. The mean gestational age at delivery was 39.4 gestational weeks. Thirty-eight women (16.0%) required Cesarean delivery.
Table 1
Characteristics of women and Comparison of characteristics according to Induced labor (n=237)
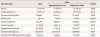
Values are presented as the median (range), mean±standard deviation, or number (%).
BMI, body mass index.
a)Total possible score = 13; b)Statistical significance.
![]()
The mean Bishop score and cervical length before induction were 4.1 and 17.4 mm, respectively, at admission to the delivery room. Among all women, 111 (46.8%) had cervical funneling, as detected by transvaginal ultrasonography (Table 1).
Between the 2 groups, there was no difference in maternal age, gestational age, pre-pregnancy maternal body mass index, ratio of engagement of the fetal head, neonatal birth weight, and rate of neonates with a birth weight greater than 3,500 g. We set the birth weight cutoff value as 3,500 g because weight less than 3,500 g is one of the favorable factors for labor induction [2627]. In contrast, the Bishop score and cervical length were significantly different between the 2 groups (Table 1).
Concerning maternal complications, the Cesarean section rate, decrease in hemoglobin level after delivery, and length of hospital stay were not different between the 2 groups. Delivery time from admission, however, was longer in the induction group than in the spontaneous labor group (597±452 vs. 924±549 hours, P<0.001), and the rate of delivery within 12 hours among women with vaginal delivery was also higher in the spontaneous labor group than in the induction group (75.0% vs. 50.4%, P=0.001) (Table 2).
Table 2
Comparison of maternal/neonatal outcomes according to Induced labor
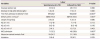
Values are presented as the number (%), mean±standard deviation, or median (range).
Hgb, hemoglobin; AS, Apgar score; NICU, neonatal intensive care unit.
a)Included only vaginal delivery; b)Statistical significance
![]()
Regarding neonatal outcomes, Apgar scores at 1 and 5 minutes were not different between the 2 groups, and the rate of Apgar scores less than 7 at 5 minutes was not different between the groups. The rate of meconium-stained amniotic fluid diagnosed at delivery and the neonatal intubation rate were also not different between the groups. In this study, the indication for NICU admission included a long duration from admission to delivery in addition to other medical problems. The NICU admission rate was higher in the induction group than in the spontaneous labor group, with statistical significance (28.0% vs. 13.2%, P=0.001) (Table 2).
Our data showed that women with Cesarean delivery had a lower initial Bishop score in both the spontaneous labor and induced labor groups. The Bishop score was higher, and the cervix length was shorter, in women with vaginal delivery than in those with Cesarean delivery. Successful vaginal delivery following induced labor was significantly higher with a shorter cervical length and a higher Bishop score (Table 3).
Table 3
Cervix status according to delivery mode and logistic regression analysis for successful vaginal delivery
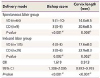
Values are presented as the mean±standard deviation or the median (range).
VD, vaginal delivery; CD, Cesarean delivery; OR, odds ratio; CI, confidence interval.
a)Statistical significance.
![]()
The reasons for Cesarean delivery are shown in Table 4, and failure to progress was the most common. An unstable lie was diagnosed when the baby changed its vertex presentation to facial presentation.
Table 4
Indications for Cesarean delivery
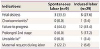
Values are presented as number (%).
a)Diagnosed as a Cesarean delivery indication when the maternal body temperature was above 38.3°C with maternal tachycardia and delivery was not likely to progress quickly; b)Diagnosed when the baby changed its presentation to facial presentation during the labor.
![]()
Discussion
Many retrospective cohort studies of nulliparous women with vertex, singleton, term pregnancies have reported that the rate of Cesarean delivery is increased approximately 2-fold in women who undergo induction of labor compared with those who experience spontaneous labor [8928293031]. However, the spontaneous labor group in these studies included an expectant management group in the mixture and women who were not induced (i.e., managed expectantly) may have had induction or Cesarean delivery recommended later in pregnancy for a medical indication. Remarkably, when electively induced nulliparous or multiparous women are compared with the appropriate comparison group (i.e., those who are expectantly managed), there is no convincing evidence that elective induction is associated with an increased rate of Cesarean delivery, regardless of whether the cervix is favorable [11121314].
Induced labor can reduce maternal anxiety and discomfort related to normal pregnancy, especially when the patient lives far from the hospital or has a history of previous pregnancy with labor abnormalities, or in case of concern for rapid labor in multiparous women.
In the present study, Cesarean section rates and the length of hospital stay were similar between the 2 groups. It has been stated that postpartum hemorrhage from uterine atony is more common in women undergoing induction or augmentation. Indeed, in one study, labor induction was associated with 17% of 553 emergency peripartum hysterectomies [32]. In contrast to this previous study, the blood loss during labor (i.e., the decreased hemoglobin level after delivery) was not different between the groups in the current analysis. Among maternal complications, only the delivery time from admission was longer in the induced labor group than in the spontaneous labor group. Regarding neonatal complications, with the exception of the NICU admission rate, other factors (Apgar scores at 1 and 5 minutes, intubation rate, and Apgar score less than 7 at 5 minutes) were similar between the groups. Although the average gestational age between the 2 groups was not different, the number of pregnant women after the estimated delivery date was higher in the spontaneous labor group than in the induced labor group.
The higher NICU admission rate in the induced labor group is thought to be due to early amniotomy as one of the methods of induction. Early amniotomy increased the duration from rupture of membranes to the delivery time. If the time from rupture to delivery is longer than 18 hours, the pediatrics department requires neonates be admitted to the NICU for close observation and the administration of prophylactic antibiotics because of the risk for sepsis, regardless of their condition at delivery. In reality, the Apgar score, which reflects neonatal health status more accurately, was not different between the 2 groups.
This study showed that women who delivered by Cesarean section had unfavorable cervical parameters compared to those who delivered vaginally. With the exception of 1 case, no woman who delivered by Cesarean delivery had a Bishop score higher than 6, meaning that a favorable cervix is one of the most important factors for vaginal delivery. However, the overall vaginal delivery rate at term was as high as 84%; thus, we favored induced labor as opposed to elective Cesarean, even when the women had an unfavorable cervix at term. The observed Cesarean section rate of 16% justifies an attempt at vaginal delivery, as this will also result in fewer complications in both present and future pregnancies. As may be expected, providers need to discuss the delivery mode with women and caregivers. Indeed, Bernardes et al. [13] reported that induction of labor at or near term in women with a median Bishop score of 3 (range, 1–6) was not associated with a higher rate of Cesarean delivery than spontaneous labor, and approximately 85% of women in both groups achieved vaginal delivery [13].
Studies of uncomplicated pregnancies reported a longer time to delivery and higher cost associated with labor induction [3334]. The time to delivery was longer for labor induction than for spontaneous labor. However, the time required for cervical ripening in labor induction was not long enough to cause the longer hospital stays. Because waiting for spontaneous labor requires additional antepartum medical visits weekly, labor induction at 39 or more weeks could be less costly.
This study has several strengths. First, we were able to obtain complete records from a single institution with a uniform protocol for analysis, including neonatal Apgar scores. Second, in order to reduce inter-observer variations, pelvic examination and ultrasonography were performed by only 1 expert. Third, unlike previous studies, from the beginning we excluded women who would likely undergo Cesarean delivery from this study, such as those with severe maternal complications or those with fetuses with severe intrauterine growth restriction or large for gestational age. Therefore, we could adjust bias of the Cesarean delivery rate to favor the control group.
However, this study also has several limitations. First, the study included a small number of women, which may limit the ability to generalize our results. Second, we had more women in the induced labor group than in the spontaneous labor group. Most women chose induced labor because of maternal circumstances, as they feared passing their due date.
In conclusion, maternal and neonatal outcomes, including the Cesarean delivery rate, were similar when labor was induced at 39 or more weeks of gestation compared to spontaneous labor in uncomplicated, nulliparous women. Our result suggests that induced labor in nulliparous women at full term may be acceptable, even when the indication is only relative for provider and maternal convenience.
Further properly designed, long-term studies on a larger scale are needed to evaluate the precise effects of induced labor on mothers and neonates.
 XML Download
XML Download