

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Endometriosis is a chronic inflammatory condition that affects fertility. The prevalence rate of endometriosis in infertile women is estimated to be 25–40% [1]. It is responsible for approximately 10% of the indications for in vitro fertilization (IVF) [2].
Endometriosis affects fertility by making the in vivo environment harmful for an oocyte or an embryo. Theoretically, surgical treatment of endometriosis could create a more favorable environment for successful conception [3]. On the other hand, surgical intervention for endometrioma may increase the risk of infertility by reducing the ovarian reserve [4].
The spontaneous pregnancy rate at 8 months after surgery was reported to be approximately 30% in infertile patients with minimal/mild endometriosis [5]. This figure is similar to the clinical pregnancy rate following a single IVF trial. In addition, as the endometriosis stage is advanced, the spontaneous pregnancy rate in expectant management may be reduced further [4]. Therefore, the IVF procedure in patients with endometriosis could be justified from the cost-effectiveness aspect. Clinicians are usually concerned about performing an operation for advanced-stage endometriosis or endometrioma before attempting an IVF [67].
The purpose of this paper is to review the efficiency and clinical application of the surgical intervention and IVF in infertile women with advanced-stage endometriosis or endometrioma, on the basis of the results of recent clinical research studies, reviews, and meta-analyses. The views on spontaneous pregnancy in patients with advanced-stage endometriosis was excluded from the focus of this review. The presence of endometrioma was considered as advanced-stage endometriosis based on the revised American Society for Reproductive Medicine classification of endometriosis [8]. Published studies were searched on PubMed and Google Scholar, combining the key terms “endometriosis” and/or “endometrioma” and/or “in vitro fertilization (IVF)” and/or “infertility” and/or “fertility” and/or “laparoscopy” and/or “cystectomy” and/or “surgery” on December 31, 2017. The main inclusion criteria of study subjects for our review were the IVF outcomes of patients with endometrioma and/or advanced-stage endometriosis and/or following surgical intervention for endometrioma. Studies published in languages other than English and those without original full text articles were also excluded from our review. In our review, we considered intracytoplasmic sperm injection cycles as IVF cycles for convenience.
Go to : 
Toxic effects of endometrioma on the ovary
The molecular mechanisms by which endometrioma causes ovarian toxicity are summarized as follows.
First, endometriotic cysts contain high levels of cell damage-mediating factors such as proteolytic enzymes, inflammatory mediators, reactive oxygen species (ROS), and iron [91011]. Thus, endometrioma per se exerts a toxic effect on healthy tissues around the cyst. These toxic contents may interfere with the expression of critical genes in the cells surrounding the endometriotic cysts, resulting in the disruption of normal folliculogenesis and causing subsequent degradation of oocytes [1112].
Second, when endometriosis spreads to the ovaries, oxidative stress levels increase in the ovarian cortex and oocyte apoptosis may occur, causing necrosis of early follicles and a consequent reduction in follicular density. In addition, high levels of ROS suppress ovarian angiogenesis, and ovarian interstitial microvascular injury takes place, which leads to a reduction in blood perfusion to the ovarian cortex [13141516]. Ultimately, the ovarian reserve may be reduced by an endometrioma, which adversely affects pregnancy outcomes.
Simón et al. [17] analyzed IVF cases with donated oocytes and reported that the pregnancy rate was significantly reduced when IVF was performed using oocytes from patients with endometriosis, regardless of the condition of the recipients. Díaz et al. [18] also reported that the IVF pregnancy rate was significantly lower in recipients who received oocytes from oocyte donors with endometriosis than in those who received oocytes from donors without endometriosis. According to a prospective study by Shebl et al. [19], the occurrence rates of metaphase II (MII) oocytes and morphologically normal oocytes were reported to be significantly lower in the endometriosis group than in the non-endometriosis group. Endometriosis stage IV was significantly associated with worse-quality oocytes than stages I–III. Thus, it may be reasonable to judge that endometriosis is clinically likely to reduce the quality of oocytes.
Go to :
Meta-analyses of IVF outcomes in women with advanced-stage endometriosis
Barnhart et al. [20] reported in their meta-analysis that IVF outcomes worsened as endometriotic disease became more advanced. When comparing the IVF pregnancy rate in infertility patients with a tubal factor, the reduction in the IVF pregnancy rate was approximately 20% in patients with mild endometriosis, while the reduction was >50% in patients with extensive/severe endometriosis.
In 2 published meta-analyses, the IVF outcomes in patients with minimal/mild endometriosis were similar to those in patients for whom IVF was performed for other indications, while the outcomes were inferior in infertile patients with moderate/severe endometriosis (fewer oocytes retrieved, lower implantation rate, and lower birth rate) [2122]. Harb et al. [21] reported that in cases with stage III/IV endometriosis, both the implantation and clinical pregnancy rates were significantly reduced by 21%.
Yang et al. [23] recently conducted a meta-analysis that limited cases to patients with endometrioma. They reported that while fewer oocytes and MII oocytes were retrieved and fewer embryos were formed in patients with endometrioma than in the controls, no significant difference was found between the patient and control groups in terms of clinical pregnancy and live birth rates. This result did not correspond with the results of the two above-mentioned meta-analyses [2122]. However, in the meta-analysis of Yang et al. [23], all of the patients who underwent surgery for endometrioma were excluded. As the study subjects were restricted to patients with relatively small-sized endometriomas, selection bias was highly possible. In addition, the few number of involved observational studies was the limitation (three or fewer studies) of the meta-analysis for clinical pregnancy and live birth rates. An inverse relationship was observed; that is, the larger the endometrioma size, the fewer the number of follicles in the ovary, which suggests that the size of the endometrioma itself could be an indicator of the aggressiveness of the disease [24]. The meta-analysis of Yang et al. [23] should be reconsidered given that endometrioma per se negatively affects ovarian reserve even before surgery [25] and that several molecular mechanisms suggest direct toxic effects of endometrioma on ovarian parenchyma and folliculogenesis.
From a clinical perspective, it is reasonable to conclude that the reproductive prognosis of IVF would be worse in the more advanced stage of endometriosis and with more increased endometrioma size.
Go to :
Surgical intervention for endometrioma in infertility management
The dominant opinion is that surgical intervention for endometrioma significantly reduces the ovarian reserve as represented by decreased serum AMH levels [262728]. According to the meta-analysis of Raffi et al. [28], serum AMH levels were reduced by approximately 40% after laparoscopic excision of endometrioma. Endometrioma per se and surgical interventions for endometrioma reduced the ovarian reserve [26282930]. Surgical intervention is likely to further reduce ovarian reserve in patients with endometrioma, whose ovarian reserve has already been reduced by endometrioma per se. In fact, according to the prospective cohort study conducted by Goodman et al. [31], baseline serum AMH levels in the endometrioma group were significantly lower than those in the control group without endometrioma, and serum AMH levels were significantly lower at 1 month after surgery. Furthermore, the larger the size of the endometrioma resection, the greater the reduction in the AMH level after surgery [32].
Roustan et al. [33] reported that the clinical pregnancy and live birth rates per IVF cycle were significantly lower in patients with decreased ovarian reserve (DOR) after surgery for endometrioma than in patients with idiopathic DOR. The retrospective study of Hong et al. [34] compared IVF outcomes between a DOR group without ovarian surgery and an endometrioma surgery-induced DOR group. They concluded that the clinical pregnancy and live birth rates were not significantly different between the two groups. However, Hong et al. [34] reported that the clinical pregnancy rate per cycle (8.5% vs. 20.2%) and live birth rate per cycle (4.2% vs. 13.4%) tended to be lower in the endometrioma surgery-induced DOR group than in the DOR group without ovarian surgery. The critical weakness of this study was the small sample size, where only 47 IVF cycles were included in the endometrioma surgery-induced DOR group. Therefore, the lack of significant differences could be attributed to the small sample size. In a retrospective study by Maignien et al. [35] involving 359 patients diagnosed as having endometriosis who underwent IVF cycles, multivariate logistic regression analysis was conducted to identify the prognostic factors that affected pregnancy rates. The results suggested that a history of surgery for endometrioma (odds ratio [OR], 0.39; 95% confidence ratio [CI], 0.18–0.84), anti-Müllerian hormone (AMH) levels of <2 ng/mL (OR, 0.51; 95% CI, 0.28–0.91), and antral follicle count (AFC) of <10 (OR, 0.27; 95% CI, 0.14–0.53) had adverse effects on assisted reproductive technology (ART) outcomes. Therefore, to prepare for surgical intervention for endometrioma, the high-risk patient group with DOR should be considered on the basis of the following factors [3]. First, poor ovarian responders should be identified by monitoring ovarian reserve markers such as baseline serum AMH level before surgery. Second, another consideration involves the patient's age and presence of bilateral lesions. According to a prospective study by Alborzi et al. [36], serum AMH levels after laparoscopic cystectomy of endometriomas were significantly reduced in women aged >38 years and diagnosed as having bilateral endometriomas. Third, the repeat surgery for recurrent endometriomas may lower AMH and AFC levels, and increase basal follicle-stimulating hormone (FSH) levels, resulting in a detrimental effect on the ovarian reserve [3738]. According to a retrospective study by Park et al. [39], a comparison of patients who underwent IVF cycles without the second-line surgery for recurrent endometrioma with those who underwent IVF cycles after the surgery showed significantly higher deleterious effects of second-line surgery on ovarian response, and implantation and clinical pregnancy rates during IVF cycles. Owing to the risk of premature ovarian failure after surgery for endometriomas in the above-mentioned cases, preoperative banking of oocytes and embryos could be options to preserve fertility before surgery.
In terms of IVF outcomes, the benefit of surgical intervention for endometrioma is uncertain. Xing et al. [40] reported in a recent retrospective study that the number of MII oocytes collected during IVF cycles was significantly lower in women who had previously undergone a laparoscopic endometrioma cystectomy than in women with pelvic endometriosis. In three recently published meta-analyses that compared patients with and patients without surgery for endometrioma, the numbers of total oocytes and MII oocytes collected during IVF cycles were significantly lower in the surgery group than in the no surgery group, but no significant differences were observed between the two groups in terms of live birth and clinical pregnancy rates [234142]. The results suggested that surgical intervention for endometrioma failed to improve reproductive outcomes in IVF cycles (Table 1). In addition to meta-analyses, several review articles consistently suggested no evidence of improvement in reproductive outcomes of IVF after surgical intervention in patients with endometrioma prior to IVF cycles [6434445].
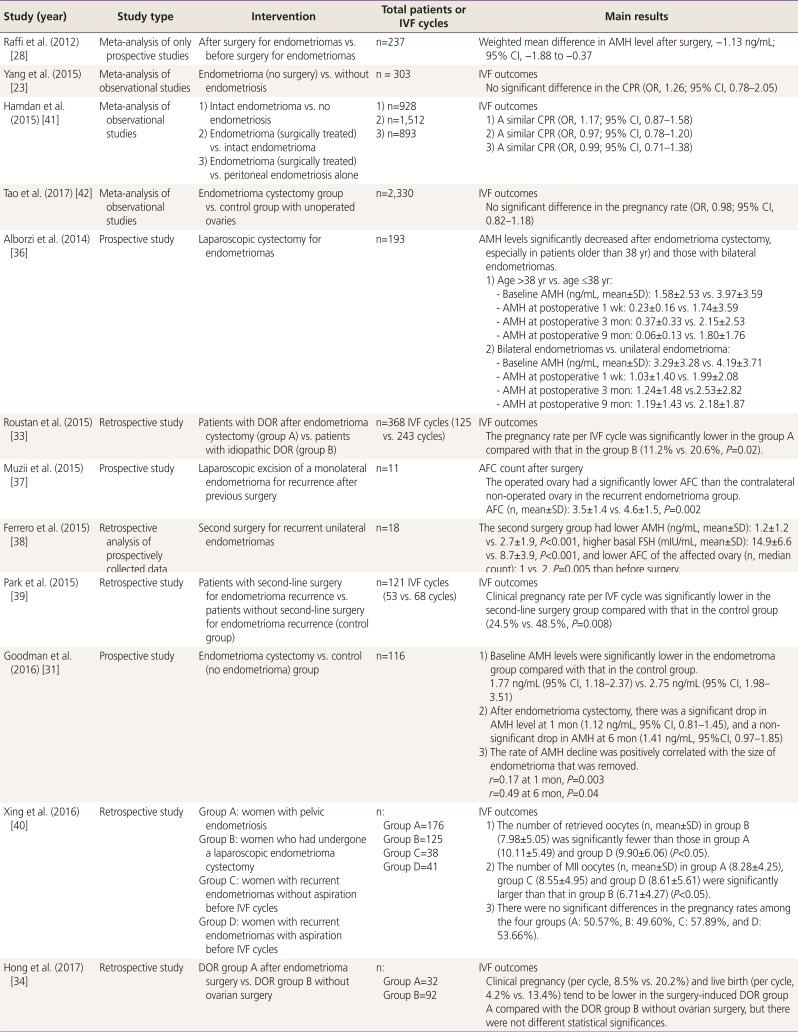
Table 1
Summary of recent clinical studies concerning surgical intervention of endometrioma and the infertility issue
| Study (year) | Study type | Intervention | Total patients or IVF cycles | Main results | ||
|---|---|---|---|---|---|---|
| Raffi et al. (2012) [28] | Meta-analysis of only prospective studies | After surgery for endometriomas vs. before surgery for endometriomas | n=237 | Weighted mean difference in AMH level after surgery, −1.13 ng/mL; 95% CI, −1.88 to −0.37 | ||
| Yang et al. (2015) [23] | Meta-analysis of observational studies | Endometrioma (no surgery) vs. without endometriosis | n = 303 | IVF outcomes | ||
| No significant difference in the CPR (OR, 1.26; 95% CI, 0.78–2.05) | ||||||
| Hamdan et al. (2015) [41] | Meta-analysis of observational studies | 1) Intact endometrioma vs. no endometriosis | 1) n=928 | IVF outcomes | ||
| 2) Endometrioma (surgically treated) vs. intact endometrioma | 2) n=1,512 | 1) A similar CPR (OR, 1.17; 95% CI, 0.87–1.58) | ||||
| 3) Endometrioma (surgically treated) vs. peritoneal endometriosis alone | 3) n=893 | 2) A similar CPR (OR, 0.97; 95% CI, 0.78–1.20) | ||||
| 3) A similar CPR (OR, 0.99; 95% CI, 0.71–1.38) | ||||||
| Tao et al. (2017) [42] | Meta-analysis of observational studies | Endometrioma cystectomy group vs. control group with unoperated ovaries | n=2,330 | IVF outcomes | ||
| No significant difference in the pregnancy rate (OR, 0.98; 95% CI, 0.82–1.18) | ||||||
| Alborzi et al. (2014) [36] | Prospective study | Laparoscopic cystectomy for endometriomas | n=193 | AMH levels significantly decreased after endometrioma cystectomy, especially in patients older than 38 yr) and those with bilateral endometriomas. | ||
| 1) Age >38 yr vs. age ≤38 yr: | ||||||
| - Baseline AMH (ng/mL, mean±SD): 1.58±2.53 vs. 3.97±3.59 | ||||||
| - AMH at postoperative 1 wk: 0.23±0.16 vs. 1.74±3.59 | ||||||
| - AMH at postoperative 3 mon: 0.37±0.33 vs. 2.15±2.53 | ||||||
| - AMH at postoperative 9 mon: 0.06±0.13 vs. 1.80±1.76 | ||||||
| 2) Bilateral endometriomas vs. unilateral endometrioma: | ||||||
| - Baseline AMH (ng/mL, mean±SD): 3.29±3.28 vs. 4.19±3.71 | ||||||
| - AMH at postoperative 1 wk: 1.03±1.40 vs. 1.99±2.08 | ||||||
| - AMH at postoperative 3 mon: 1.24±1.48 vs.2.53±2.82 | ||||||
| - AMH at postoperative 9 mon: 1.19±1.43 vs. 2.18±1.87 | ||||||
| Roustan et al. (2015) [33] | Retrospective study | Patients with DOR after endometrioma cystectomy (group A) vs. patients with idiopathic DOR (group B) | n=368 IVF cycles (125 vs. 243 cycles) | IVF outcomes | ||
| The pregnancy rate per IVF cycle was significantly lower in the group A compared with that in the group B (11.2% vs. 20.6%, P=0.02). | ||||||
| Muzii et al. (2015) [37] | Prospective study | Laparoscopic excision of a monolateral endometrioma for recurrence after previous surgery | n=11 | AFC count after surgery | ||
| The operated ovary had a significantly lower AFC than the contralateral non-operated ovary in the recurrent endometrioma group. | ||||||
| AFC (n, mean±SD): 3.5±1.4 vs. 4.6±1.5, P=0.002 | ||||||
| Ferrero et al. (2015) [38] | Retrospective analysis of prospectively collected data | Second surgery for recurrent unilateral endometriomas | n=18 | The second surgery group had lower AMH (ng/mL, mean±SD): 1.2±1.2 vs. 2.7±1.9, P<0.001, higher basal FSH (mIU/mL, mean±SD): 14.9±6.6 vs. 8.7±3.9, P<0.001, and lower AFC of the affected ovary (n, median count): 1 vs. 2, P=0.005 than before surgery. | ||
| Park et al. (2015) [39] | Retrospective study | Patients with second-line surgery for endometrioma recurrence vs. patients without second-line surgery for endometrioma recurrence (control group) | n=121 IVF cycles (53 vs. 68 cycles) | IVF outcomes | ||
| Clinical pregnancy rate per IVF cycle was significantly lower in the second-line surgery group compared with that in the control group (24.5% vs. 48.5%, P=0.008) | ||||||
| Goodman et al. (2016) [31] | Prospective study | Endometrioma cystectomy vs. control (no endometrioma) group | n=116 | 1) Baseline AMH levels were significantly lower in the endometroma group compared with that in the control group. | ||
| 1.77 ng/mL (95% CI, 1.18–2.37) vs. 2.75 ng/mL (95% CI, 1.98–3.51) | ||||||
| 2) After endometrioma cystectomy, there was a significant drop in AMH level at 1 mon (1.12 ng/mL, 95% CI, 0.81–1.45), and a non-significant drop in AMH at 6 mon (1.41 ng/mL, 95%CI, 0.97–1.85) | ||||||
| 3) The rate of AMH decline was positively correlated with the size of endometrioma that was removed. | ||||||
| r=0.17 at 1 mon, P=0.003 | ||||||
| r=0.49 at 6 mon, P=0.04 | ||||||
| Xing et al. (2016) [40] | Retrospective study | Group A: women with pelvic endometriosis | n: | IVF outcomes | ||
| Group B: women who had undergone a laparoscopic endometrioma cystectomy | Group A=176 | 1) The number of retrieved oocytes (n, mean±SD) in group B (7.98±5.05) was significantly fewer than those in group A (10.11±5.49) and group D (9.90±6.06) (P<0.05). | ||||
| Group C: women with recurrent endometriomas without aspiration before IVF cycles | Group B=125 | 2) The number of MII oocytes (n, mean±SD) in group A (8.28±4.25), group C (8.55±4.95) and group D (8.61±5.61) were significantly larger than that in group B (6.71±4.27) (P<0.05). | ||||
| Group D: women with recurrent endometriomas with aspiration before IVF cycles | Group C=38 | 3) There were no significant differences in the pregnancy rates among the four groups (A: 50.57%, B: 49.60%, C: 57.89%, and D: 53.66%). | ||||
| Group D=41 | ||||||
| Hong et al. (2017) [34] | Retrospective study | DOR group A after endometrioma surgery vs. DOR group B without ovarian surgery | n: | IVF outcomes | ||
| Group A=32 | Clinical pregnancy (per cycle, 8.5% vs. 20.2%) and live birth (per cycle, 4.2% vs. 13.4%) tend to be lower in the surgery-induced DOR group A compared with the DOR group B without ovarian surgery, but there were not different statistical significances. | |||||
| Group B=92 | ||||||
IVF, in vitro fertilization; AMH, anti-Müllerian hormone; CPR, clinical pregnancy rate; OR, odds ratio; CI, confidence interval; SD, standard deviation; DOR, decreased ovarian reserve; AFC, antral follicle count; MII, metaphase II.; wk, week; mon, months.
![]()
In cases of infertility associated with advanced-stage endometriosis, including endometrioma, IVF could be recommended immediately to achieve pregnancy, as surgical treatment has few benefits [46]. However, surgery for severe endometriosis, including endometrioma, may be considered before IVF in the following cases: first, when the pain related to endometriosis is severe [3] and, second, when malignancy cannot be excluded [7]. Third, according the 2014 European Society of Human Reproduction and Embryology guidelines, for patients with endometrioma measuring ≥3 cm, laparoscopic ovarian cystectomy is recommended before IVF to reduce the risk of infection during oocyte retrieval and facilitate access to follicles, or to improve the ovarian response to controlled ovarian stimulation [4]. Fourth, surgical intervention could be considered when the qualities of the oocytes and embryos were found to be poor in IVF cycles before surgery, or in cases of recurrent implantation failure. Theoretically, surgery for endometrioma could facilitate follicular development by reducing the tension in the ovarian tissue. Furthermore, it could reduce the levels of inflammatory factors in follicular fluid [4748]. Soriano et al. [49] performed extensive laparoscopic excisional surgery, including bowel and urinary resection, in 78 patients with severe endometriosis who had repeated IVF failures and reported that 33 patients (42.3%) conceived successfully after surgery (30 patients conceived via IVF cycles, while 3 cases conceived naturally). Restoration of a normal uterine anatomy by surgical intervention could help improve IVF outcomes in these women. However, endometrioma per se and surgical intervention could have toxic effects on ovarian follicles [50]. Consideration of the ovarian reserve may be essential before surgery for severe endometriosis, including endometrioma.
Go to :
Prolonged pituitary downregulation prior to IVF
In cases of infertile women with endometriosis, the treatment approach prior to IVF must be individualized. According to the study conducted by Sallam et al. [51] that meta-analyzed three RCTs in women with surgically diagnosed endometriosis and compared the study group that received gonadotrophin-releasing hormone (GnRH) agonist treatment for 3 to 6 months before IVF with the control group that received no treatment prior to IVF, the clinical pregnancy rate was significantly improved by 4.28-fold in the study group as compared with the control group. The GnRH agonist could lower concentrations of various inflammatory cytokines such as IL-6 [525354]. As a result, this can reduce the toxic effects of peritoneal cytokines on oocytes or embryos. Prolonged pituitary downregulation prior to IVF could be helpful for infertile women with endometriosis.
On the other hand, long-term administration of the GnRH agonists could suppress the expression of implantation factors, which could lead to decreased endometrial receptivity [55]. In addition, use of the GnRH agonist could induce side effects such as hot flashes, vaginal dryness, and decreased bone mineral density. Recently, as an alternative for reducing the side effects of long-term GnRH agonist treatment, dienogest, a novel progestin, is gaining attention [56]. Muller et al. [57] conducted a prospective cohort study that compared pregnancy rates in the following 3 groups after surgical intervention for endometriosis: a group of patients who took 2 mg of dienogest daily for 6 months prior to IVF (group I), a group of patients who had monthly GnRH agonist treatment for 6 months prior to IVF (group II), and a patient group who had no hormonal therapy prior to IVF (group III). The pregnancy rates in groups I, II, and III were reported to be 44.7%, 34.3%, and 16.7%, respectively. A significant difference in clinical pregnancy rate was found between groups I and III (P=0.012). No significant difference was found between groups II and III. While long-term administration of the GnRH agonist conferred a risk of reduced endometrial receptivity, it was thought to show more positive results in terms of clinical pregnancy rates with concurrent dienogest use, as it could improve progesterone resistance in the endometrium [58].
If surgical intervention for endometriosis is performed, when would be the best time to perform ART after the surgery? A retrospective study on ART timing has recently been published. AlKudmani et al. [59] reported that the ongoing pregnancy rate was significantly higher when IVF was performed between 7 and 25 months after surgery for endometriosis than when IVF was performed between 0 and 3 months after surgery. Therefore, if IVF is planned after surgical intervention for endometriosis, administration of long-term hormone therapy prior to IVF should be considered for the suppression of residual endometriotic lesions, rather than performing IVF immediately after surgery to improve the pregnancy rate in IVF. Additional prospective studies about this topic should be conducted in the future.
Go to :
Summary
Endometriosis could be toxic to the ovary and may reduce the ovarian reserve. Endometriosis may have negative effects on oocyte and embryo development. Clinically, the more advanced the endometriosis stage and the bigger the endometrioma, the poorer the reproductive outcomes of IVF. However, no clear evidence supports the use of surgical intervention before IVF to improve the reproductive outcomes of IVF in women with advanced-stage endometriosis or endometrioma. When the pain is severe or when cancer is suspected, laparoscopic ovarian cystectomy prior to IVF may be necessary and justified. When the size of the endometrioma is very large, surgery could be required prior to IVF to facilitate access to follicles during oocyte retrieval or to improve the ovarian response to controlled ovarian stimulation.
IVF as a means of achieving pregnancy could not overcome all the negative effects of endometriosis on fertility [60]. In infertile women with advanced-stage endometriosis or endometrioma, individualizing treatment methods for fertility is important. Basically, unconditional surgery prior to IVF was not recommended in these women. When the qualities of oocytes and embryos are observed to be seriously degraded in IVF cycles or when recurrent implantation fails occur in IVF cycles, surgical intervention for endometrioma could be considered. Restoration of a normal uterine anatomy by surgical intervention could help improve IVF outcomes in infertile women with severe endometriosis and repeated IVF failures [49]. In addition, prolonged pituitary downregulation prior to IVF cycles to suppress remnant postoperative lesions, may be helpful to increase the clinical pregnancy rate in subsequent IVF cycles. In the future, further prospective studies may be required to establish more-detailed guidelines for preserving the fertility of women with endometriosis.
Go to :
 XML Download
XML Download