

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
According to incidence rates, stomach cancer is the fifth most common cancer worldwide and first and fourth among men and women, respectively, in Korea.1,2) The age-standardized rates for allcancer incidence increased by 3.4% annually from 1999 to 2012, and then began to decrease from 2012 to 2015 (annual percent change, −6.1%).2) Stomach cancer was the most commonly diagnosed cancer in 2015, followed by colorectal, thyroid, lung, and breast cancer. However, stomach cancer started to decrease around 2011.2) Although the 5-year relative survival rates for stomach cancer increased in both sexes, from 42.8% in 1993~1995 to 75.4% in 2011~2015, the patients still complained of side effects such as nausea, vomiting, anorexia, diarrhea, fatigue, anemia, and cognitive function changes.3,4) Patients with stomach cancer experience changes in cognitive function due to the course of chemotherapy.5) According to the conceptual model of change in cognitive function related to chemotherapy proposed by Hess and Insel in 2007, psychological factors such as stress, depression, anxiety, and distress and physiological factors such as neurotoxicity, anemia, cytokine, hormonal changes are involved in functional changes.6) Thus, cancer diagnosis and treatment affect not only physical but also psychological factors.7) These problems are important because they are related to mortality and suicide rates of cancer patients. The death rate is increased by 27% in cancer patients with distress, depression, anxiety, and poor quality of life.8) Among these factors, distress includes all psychological, social, and spiritually unpleasant emotional (both cognitive and behavioral) experiences, which reduce patient adaptation to cancer-related symptoms and treatment.9) This is a broad concept that includes anxiety and depression, while distress is reportedly caused by a wide variety of factors in cancer patients. Most studies on distress due to chemotherapy have been conducted in patients with breast cancer. These studies were likely easier to perform because of the high accessibility of breast cancer patients, who are mostly female, compared to that of patients with stomach cancer, with a higher incidence in men.
The present study is based on the model of change in cognitive function related to chemotherapy proposed by Hess and Insel.6) This study aimed to assess differences in stress, psychological distress, anxiety, and depression between patients receiving and not receiving chemotherapy and to identify the factors affecting cognitive function in stomach cancer patients.
METHODS
1. Design and sample
A descriptive survey with cross-sectional design was used to obtain data from stomach cancer patients in the National Cancer Center in 2016. The subjects included 182 stomach cancer patients who received and did not receive chemotherapy. The inclusion criteria included patients 18 years or older who had been diagnosed with stomach cancer, who were able to communicate, who understood the purpose of the study, and who agreed to participate in the study. Patients who were diagnosed with cancer other than stomach cancer and those who had no disease were excluded from the study.
The effect size of 0.5 with 80% power and a significance level of 0.05 required for independent sample t-tests using G*POWER 3.1. The optimal sample number was 64 patients per group (128 total). An additional 20% was added to account for attrition. Therefore, the planned sample size was 156 participants.
2. Measures
The demographic characteristics of the participants used a questionnaire designed by the researchers through the literature review. The clinical information was about, pathological diagnosis, stage at diagnosis, and types of chemotherapy. All participants gave their informed consent to participate. Each participant's medical record was reviewed by the oncology nurse to validate their clinical characteristics.
Stress was measured using the Korean version of the Global Assessment of Recent Stress (GARS).10) This instrument contains a total of eight items with a score ranging from 0 to 72 points. A higher score indicates more serious stress. The Cronbach's α of the Korean version of the GARS was .86.11) In this study, the Cronbach's α was .80.
Patient anxiety and depression were measured using the Korean version of the Hospital Anxiety-Depression Scale (HADS).12,13) It consists of two subscales, which is a 14-item self-reported questionnaire designed to measure the level of anxiety and depression. Each seven items had been answered by the patient on a four-point Likert (0~3) scales. The HADS is scored by summing the ratings for the 7 items to calculate subscale scores for anxiety and depression, respectively.12) In the present study, the Cronbach's α of the HADS was .80 and .83 respectively.
The Distress Thermometer (DT) is a one-item self-report screening tool for measuring psychological distress in cancer patient.14) The instrument measures distress levels over the past week using an 11-point scale from 0 (no distress) to 10 (extreme distress) based on a thermometerlike Likert scale and a midpoint anchor labeled ‘moderate distress’.14)
The original of the Montreal Cognitive Assessment (MoCA) is a neurocognitive test designed to screen for mild cognitive impairment.15) It scores from 0 to 30, where higher scores indicate better cognition and a score below 26 indicates cognitive impairment corresponding to mild cognitive impairment. The MoCA consists of 12 items and it can be administered in 10 minutes. In the MoCA-K, the words used in the short-term memory recall task and the letters used in the trail-making B task were changed, and the phonemic fluency task was replaced with a semantic fluency task.15) The internal reliability of MoCA-K was .84 in this study.
Data analysis
Descriptive statistics were conducted for socio-demographic and clinical characteristics. Independent t-tests and analysis of variance (ANOVA) were used to assess differences among the groups. Pearson's correlation coefficients were performed to assess the correlation among study variables. Hierarchical multiple regression analysis was performed to identify the factors that influenced distress in stomach cancer patients. All statistical tests were two-tailed, with p<.05 indicating statistical significance. All analyses were conducted using SPSS 23.0 for Windows (IBM corporation, Chicago, USA).
Ethical considerations
This study was conducted after having obtained approval (NCC 2016-07-045-002) by the Institutional Review Board of the hospital for the ethical protection of study subjects. Informed consent was obtained from all participants. Confidentiality was ensured through a coding system, with numbers replacing the participants' names. When collecting the data, the participants received explanations about the purpose and procedures of the study. The participants were also informed that they could terminate their participation whenever they wished, that anonymity of study participants would be maintained.
RESULTS
1. Sample characteristics
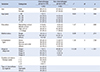
The study participants comprised 182 stomach cancer patients: 123 (67.6%) of patients who received chemotherapy and 59 (32.4%) with no chemotherapy. Participants characteristics are displayed in Table 1. There was statistical significance in sex between the two groups (χ2 =5.32, p=.029). Of the participants, 92 (74.8%) were diagnosed with stage 3 over in the chemotherapy group, while 8 (13.5%) in the non-chemotherapy group. There were significant associations in disease stage(χ2 =112.26, p<.001) between two groups (Table 1).
2. Descriptive statistics of the study variables and group differences.
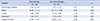
Table 2 show descriptive statistics for the stress, distress, depression and anxiety, and cognitive function. There were significant differences in psychological distress and cognitive function between patients receiving and not receiving chemotherapy. The mean score of stress was statistical significance in the two group (t=−2.65, p=.009). The mean score of cognitive function in the chemotherapy group was 21.53, which was lower than that of the non-chemotherapy group (t=−2.86,
p=.005).
3. Correlations among study variables
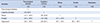
A statistically significant negative correlation was observed for the relationship between cognitive function and stress, anxiety, depression, and psychological distress (r=−.29, p=.001). There were positive correlations with stress (r=.41, p<.001), anxiety (r=.34, p<.001), and depression (r=.33, p<.001). Thus, the lower the cognitive function, the higher the psychological distress; similarly, the higher the level of stress, anxiety, and depression, the higher the level of psychological distress (Table 3).
4. Factors affecting cognitive function in patients with stomach cancer
Hierarchical multiple regression analysis was conducted to identify predictors of cognitive function in patients with stomach cancer (Table 4). Potential confounding variables were minimally controlled for age, gender, and chemotherapy in the first model (model 1). The second model (model 2) was adjusted for the variables in model 1 plus stress, psychological distress, anxiety, and depression. The factors affecting cognitive function in patients with stomach cancer included age (B= −.18, p<.001), chemotherapy (B =−3.09, p<.001), and psychological distress (B = −.38, p=.036).
DISCUSSION
This study was carried out to manage change of cognitive function by analyzing the factors affecting this cognitive function in stomach cancer patients based on the literature review and Hess and Insel6) model of change of cognitive function related to chemotherapy. The study population was similar to a previous study in that the average patient age was 50 years or older and the incidence of stomach cancer was higher in men than that in women.16) Stomach cancer patients who did not receive chemotherapy had higher stress scores than those in patients who received chemotherapy. This is because the quality of life experienced by stomach cancer patients due to gastrectomy, negative body image, and changes in life processed greatly affect their stress.17).
In this study, stomach cancer patients who received chemotherapy had lower level of stress. The patients also had a lower cognitive function score than those who did not receive chemotherapy. This finding is consistent with the results that there is cognitive impairment, such as impairment of performance, concentration, memory, language memory, and recall memory area, in colorectal cancer and breast cancer patients receiving chemotherapy.18)
Breast cancer patients who received chemotherapy with doxorubicin, cyclophosphamide, and taxane over six months had changes in their cognition, such as decreased attention and memory, and symptoms of anxiety, depression and fatigue.19) Because these factors have a negative impact on the physical, psychological, and cognitive functions of cancer patients receiving chemotherapy, they increase an unpleasant emotional experience for cancer-related symptoms and treatment.20) Since most cancer patients are focused on physical symptoms, and psychological symptoms such as depression and stress are being ignored in the treatment process.21) In this study, patients were more likely to be exposed to emotional problems. They need to be actively concerned about the psychological symptoms that are as important as the patient's physical symptoms and manage these symptoms through periodic interviews. Patients with stomach cancer receiving chemotherapy have problems with anorexia, headache, vomiting, malnutrition, and weight loss.22) Anorexia and malnutrition cause anemia and fatigue and these physical problems seriously affect cognition, emotion, and psychological well-being.23) Cancer patients experience physical and psychological distress due to these problems.24) According to previous studies, individual nutritional management for stomach cancer patients receiving chemotherapy is needed to manage their psychological distress and individualized exercise prescriptions and physical activities are needed for the treatment of fatigue.
In this study, age, chemotherapy, and psychological distress increased vulnerability to cognitive function in stomach cancer patients. Psychological distress had a partial mediating effect in the relationship between self-reported cognitive decline and quality of life in colon cancer patients.25) Therefore, distress in cancer patients should be categorized through active screening and appropriate treatment services should be provided to patients who require an intervention. Although evidence of chemotherapy induced impairments in cognitive function does exist, there is still much to be discovered. More studies are needed to further elucidate the phenomenon of chemotherapy induced cognitive dysfunction and to describe its characteristics (e.g., onset, duration).26)
This study was subject to several limitations. First, all the participants were stomach cancer patients at a cancer hospital, which limits the generalizability of the study results. Second, since cross-sectional studies were performed, studies should be conducted to verify the presence of distress over the duration of chemotherapy. Despite these limitations, the merit of this study is that we measured cognitive function changes using the MoCA-K, a standard tool for screening for mild cognitive impairment. The MoCA-K has a strength to integrate cognitive functions of various domains.27) Changes in cognitive function related to chemotherapy have been subjective and measured using insensitive tools, although patient symptoms may be minimal.28)
CONCLUSIONS
This study used the conceptual model described by Hess and Insel to examine the effect of chemotherapy on cognitive function in patients with stomach cancer. Psychological distress is important factor affecting cognitive function; therefore, these factors should be accurately measured and assessed to manage distress caused by chemotherapy among patients with stomach cancer.
As the number of stomach cancer survivors grows, they have gained the attention in the healthcare system. Survivors' reports about their experience of late effects either from the stomach cancer or its chemotherapy now suggest the needs for the related care within the healthcare system. When the proper care for chemotherapy related toxicity and psychological distress is provided, the quality of survivors' life would be enhanced and their emotional stability would be ensured as well.
 XML Download
XML Download