

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Herpes zoster (shingles, HZ) is caused by reactivation of the varicella-zoster virus (VZV), which typically remains latent after primary infection with varicella (chickenpox) during childhood. HZ is largely considered to be an once-in-a-lifetime experience and recurrence is thought to be limited to immunocompromised individuals.
Recently, a live attenuated vaccine against HZ was introduced world-wide and licensed to persons aged 50 years and older. The efficacy of the vaccine in persons over 60 years old and aged 50–59 years old is 51% and 70%, respectively.12 However, the indication of HZ vaccination on the persons who have already had an episode of HZ, and the appropriate withdrawal period for the vaccination after HZ have not yet been elucidated.
Although there have been several studies on HZ recurrence, these usually depended on hospital-based data with a small number of cases or a short follow-up period. General population based epidemiological data on the recurrence of HZ is necessary for treating and preventing recurrent cases. These data will also play an important role in establishing vaccination guidelines. Therefore, we aimed to assess the recurrence rate of HZ and to identify risk factors associated with recurrence using a population-based Korean database.
METHODS
Data source
In Korea, nearly all people have been enrolled obligatorily in the National Health Insurance Service (NHIS) since 1989. All demographic data, including patient's age, gender and socioeconomic status were collected along with diagnoses, physical and laboratory examination, treatment, prescription, nursing acts, and hospitalization.
This study used nationally representative random samples of the NHIS database, NHIS-National Sample Cohort (NHIS-NSC) 2002–2013. The samples were collected from the records for 1,025,340 persons, approximately 2.2% of the entire population at the beginning in 2002, and included all associated medical data of the enrolled patients from January 1, 2002 to December 31, 2013.
Study population
Among the patients included in the NHIS-NSC 2002–2013, we selected the 746,816 patients older than 20 years of age. NHIS-NSC 2002–2013 maintains the sample size by replacing the death cases or cases with loss of qualification with newborn cases every year. Of course, there is variation of follow up period in cases under 20 years old, and these cases were included in the cases under 20 years old. Therefore, we excluded those cases from the study. We followed up on all included cases until death, loss of qualification, or December 31, 2013. In addition, we set up the year 2002 as the washout period.
Case definition
HZ cases were identified through a database search for any subject with the HZ-related International Classification of Disease 10th revision code (ICD-10 code, B02) except postherpetic neuralgia (PHN) with oral antiviral therapy for more than 5 days or intravenous antiviral therapy. This definition excluded overestimation due to non-HZ cases like herpes simplex cases as we previously reported.3
Zoster-related pain (ZRP) is the most common complication of HZ and is related to HZ recurrence. We defined the duration of ZRP as that of treatment of pain associated with an initial HZ episode. We identified the duration through a database search for defined HZ cases with prescribed painkilling medications, or PHN related ICD-10 code with pain killer medication following the diagnosis of HZ. We categorized patients with ZRP by treatment duration of shorter than 31 days, 31–90 days, and longer than 90 days.
We identified initial HZ episode cases, as well as first and second recurrence cases. To meet the definition of recurrence, a minimum of 6 months must have passed from the previous HZ. From those data, we calculated recurrence rate, mean time period and time trend for recurrence following the initial episode.
Risk factors influencing recurrence
We also collected epidemiological features of initial HZ episodes and evaluated their relationship with recurrence rate. These features at the time of the initial episode included: 1) age/gender, 2) socioeconomic status, 3) residence area, 4) duration of ZRP, 5) hospitalization, and 6) immune status and comorbid diseases. Immune status was determined based on the presence of specific diseases, including solid and hematologic malignancies, autoimmune diseases, human immunodeficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS), chronic renal diseases, and chronic hepatic diseases within 6 months before or after the diagnosis of HZ. Patients with one or more of these diseases were considered immunocompromised. The presence or absence of comorbid diseases, such as diabetes mellitus, hypertension and hyperlipidemia was also evaluated. Immunocompromised cases and cases with comorbid disease were identified through a database search for any subject with related ICD-10 codes as described in Table 1.
Table 1
ICD-10 codes for the operational diagnosis of immunocompromised cases or comorbid diseases

ICD-10 = International Classification of Disease 10th revision, HIV/AIDS = human immunodeficiency virus infection and acquired immune deficiency syndrome.
![]()
Statistical analysis
Recurrence rate was calculated as the number of HZ recurrent cases per 1,000 follow-up person years after initial episode. The hazard ratios (HRs) of the various epidemiological features from the initial episode to recurrence were deduced by using univariate Cox proportional hazards regression. The multivariate Cox proportional hazards regression was also used to determine the association between HZ recurrence and HZ recurrence risk factors such as duration of ZRP, immune status, and comorbid diseases to adjust for gender, age, and socioeconomic status. Cumulative recurrence rate curves were calculated using Kaplan-Meier statistics. SAS enterprise guide 4.2 (SAS Institute Inc., Cary, NC, USA) was used for statistical analyses.
RESULTS
During the study period, 39,441 initial episodes of HZ were identified with an incidence of 5.1 per 1,000 person years. Of the initial episodes, 15,638 (39.7%) were men and 23,803 (60.3%) were women. The incidence of HZ increased with age and 66.8% of cases were in patients over 50 years old. For socioeconomic status, the lowest quintile comprised 15.0% of cases. There were 5,408 (13.7%) immunocompromised patients and proportions of solid cancer, autoimmune diseases, chronic renal diseases, chronic hepatic diseases, hematologic cancer, and HIV/AIDS were 6.1%, 5.3%, 2.7%, 0.9%, 0.5%, and 0.1%, respectively. In total, 18,384 (46.6%) of patients with an initial HZ episode had either of diabetes mellitus, hypertension, or dyslipidemia. More detailed epidemiologic features are summarized in Table 2.
Table 2
Epidemiologic features of the initial HZ episode

HZ = herpes zoster, QL = lowest quintile, QO = higher four quintile, ZRP = zoster-related pain, HIV/AIDS = human immunodeficiency virus infection and acquired immune deficiency syndrome.
![]()
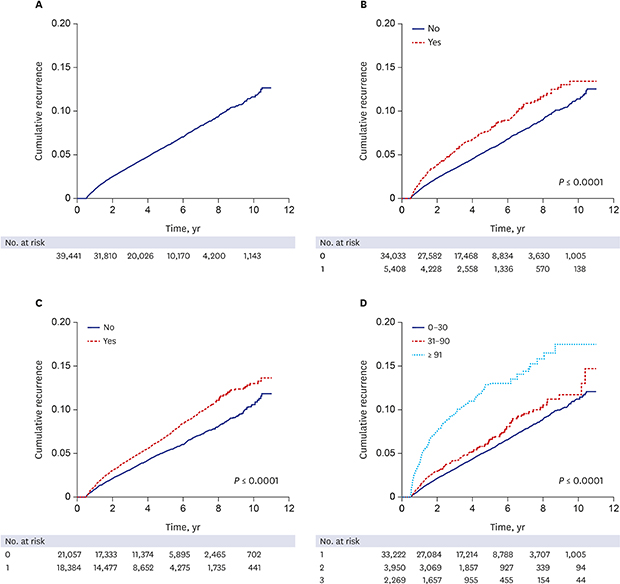
For the recurrence study, 39,441 cases were followed for a mean of 4.4 years, with a range of 1–4,014 days. In total, 2,358 HZ recurrences were observed in 2,100 cases, which included 232 cases with a second recurrence and 26 cases with a third recurrence. The overall recurrence rate was 12.0 per 1,000 person years, or 5.3%. The time between initial HZ episode and first recurrence varied from 181 to 3,815 days, with a mean of 1,062.9 days. A cumulative recurrence rate curve using Kaplan-Meier estimates shows a linear increase until 10 years of follow-up (Fig. 1A).
 | Fig. 1The cumulative recurrence rate of HZ according to risk factors at initial episode. (A) overall, (B) immune status, (C) comorbid diseases, (D) duration of zoster-related pain.HZ = herpes zoster.
|
Age and gender were significantly associated with HZ recurrence (P < 0.001). The recurrence rate in patients over 50 years was 5.8% (1,517/26,347), whereas that in the younger group was 4.5% (585/13,094). Women had more frequent recurrence than men, with a HR of 1.476 (95% CI, 1.345–1.619). In contrast, socioeconomic status and residence area were not significantly associated.
ZRP lasting longer than 30 days was significantly associated with HZ recurrence (P < 0.001). Recurrence rates of the ZRP groups were as follows: 4.9% (1,643/33,222) for ZRP lasting less than 31 days; 5.7% (225/3,950) for ZRP lasting 31–90 days; and 10.2% (232/2,269) for ZRP lasting longer than 90 days. On the other hand, hospitalization did not show a statistical significance.
Out of 2,100 patients with recurrence, 373 (17.8%) were immunocompromised and 1,727 (82.2%) were immunocompetent at the time of the first HZ episode. Some immunocompromising conditions, such as hematologic malignancies and autoimmune diseases, were significantly associated with recurrence (P < 0.001). However, solid cancer, HIV/AIDS, chronic renal diseases, and chronic hepatic disease showed no statistical significance. Among the comorbid diseases, dyslipidemia and hypertension were significantly related with recurrence of HZ (P < 0.001), but diabetes mellitus was not (Table 3).
Table 3
HR of candidate risk factors influencing HZ recurrence

HR = hazard ratio, HZ = herpes zoster, CI = confidence interval, QL = lowest quintile, QO = high four quintile, HIV/AIDS = human immunodeficiency virus infection and acquired immune deficiency syndrome.
aThe HR was adjusted for age, gender, and socioeconomic status.
![]()
A Kaplan-Meier estimate curve of cumulative recurrence rates based on the immune status, the presence of the comorbid diseases, and the duration of ZRP during the initial HZ episode is shown in Fig. 1B-D, respectively. For all parameters except ZRP duration, cumulative recurrence rates increased linearly with time from the first year following the initial HZ episode, as shown in the overall cumulative incidence curve. In cases of ZRP lasting longer than 90 days, cumulative recurrence rate increased sharply within 4 years following the initial HZ episode and gradually increased thereafter.
DISCUSSION
In this study, the population-based recurrence rate of HZ was12.0 per 1,000 person years (5.3%) during a mean follow-up period of 4.4 years. Compared with previous studies, our recurrence rate is on the higher side, with a limited number of studies reporting the recurrence of HZ of 0.2%–12.5%.1456789101112 In reports with a relatively short follow-up period of 3–5 years, the recurrence rate was 0.2%–0.9% out of 457–1,075 initial cases.159 As expected, studies with a longer follow-up period tended to show a higher recurrence rate. For example, Hope-Simpson8 identified 8 recurrence cases out of 192 (4.2%) during 16 years. Similarly, in a larger study population, 31(5.3%) recurrence cases were identified from 590 initial HZ episodes from 1945 to 1959.6 Recently, Yawn et al.4 reported a relatively high recurrence rate of 6.2%, with 105 recurrence cases out of 1,669 first episodes during an average follow-up period of 7.3 years. The discrepancy in these results likely originates from the different population composition, study methods, and duration of follow-up. In addition, most studies were designed to focus on the characteristics of initial HZ episodes rather than HZ recurrence. In most studies, the whole study period was disclosed rather than the follow-up period from the initial episode to the recurrence, meaning the exact follow-up period could not be concluded from the data. Accordingly, recurrence rates could not be expressed by the number of recurrent cases per 1,000 person years, but instead by percentage of initial HZ cases. In this study, we used nationally representative random samples of 39,441 initial HZ episodes with a relatively long-term follow-up period of 4.4 years and a whole study period of 11 years. Therefore, we expect our data to reflect the actual HZ recurrence rate.
Unexpectedly, the recurrence rate was higher than the incidence rate in this study, and the cumulative recurrence rate increased linearly from the initial HZ episode without a sufficient time lag. Generally, a history of previous viral disease serves as a protective factor to recurrence, although this effect may decrease with time. For example, primary infection with VZV results in life-long protection against contracting subsequent varicella after re-exposure. In the case of HZ, it has been reported that VZV-specific T-cell mediated immunity (VZV-CMI) rises and is maintained for 2 years, with higher levels than that of the pre-rash period.13 Recently, the live attenuated HZ vaccine was demonstrated to have a preventive effect against HZ.12 Therefore, we expected recurrence rates to be lower than that of initial episodes, and that, even if there was recurrence, there would be a considerable time lag from the initial episode to the recurrence. However, our results seem to show that there may be little protective effect of an initial HZ episode on subsequent recurrence. This may be explained, in part, by the social boosting theory that varicella vaccination during childhood results in increased HZ incidence due to decreased exposure to VZV in adulthood.1415161718 In Korea, varicella vaccination has been designated as national immunization program since 2006. Unfortunately, exact vaccination rate over the time has not been disclosed. However, from the report by the Korea Centers for Disease Controls and Prevention, 97.3% of infants born in 2012 were completed the varicella vaccination inoculation in 2015. Based on this theory and high uptake of varicella vaccination, we hypothesize that after an initial HZ episode, VZV-CMI may rapidly decrease to a level that is insufficient to suppress the reactivation of latent HZ due to deficient exogenous booster.
On the other hand, there are some limitations to comparing incidence rate and recurrence rate. There must be some differences in the epidemiological distribution between the population for the incidence study and that of the recurrence study. The follow-up period is another factor to consider. It has been reported that the cumulative recurrence rate stabilizes rather than increases linearly after a considerable amount of time from the initial episode.4 This means that a longer follow-up period may result in a lower recurrence rate per 1,000 person years while maintaining the incidence rate if the study period is long enough. Therefore, for precise evaluation of the protective role of an initial episode, further studies with a larger population and a longer follow-up period are necessary.
From a previous study, the highest frequency of VZV-specific CD4 memory cell is observed at 34 years of age after wild-type VZV infection.19 In an elderly group over 60 years old, VZV-CMI response progressively decreased with age; a 2.7%–3.9% decline each year was reported depending on the assay method. In addition, VZV-CMI responses following zoster vaccination or HZ are lower in older persons.2021Although there have been no direct reports of VZV-CMI response after HZ according to age, it could be assumed that immune response to initial HZ would be lower and decrease more quickly in elderly patients. Therefore, HZ recurrence could be more common in the elderly, coinciding with our results. VZV-CMI is also influenced by various diseases and medications which can induce immune suppression. For example, solid cancer, hematologic malignancies, systemic lupus erythematosus, renal failure, antineoplastic drugs, and other immune suppressants are reported to be associated with the incidence and recurrence of HZ.222324
Although host immune status is the most important risk factor for HZ, concurrent chronic diseases such as diabetes, hypertension, dyslipidemia, chronic obstructive pulmonary disease, depression, and hypothyroidism have recently been reported to be associated with HZ incidence and recurrence.252627 In cases of diabetes, a higher incidence of HZ and PNH is thought to be related to T-cell dysregulation.282930 In cases of dyslipidemia, high cholesterol levels or statin use may result in VZV reactivation.3132 In our study, both dyslipidemia and hypertension were significant risk factors of HZ recurrence.
In this study, ZRP lasting longer than 30 days was significantly associated with a higher recurrence rate. Long-lasting ZRP is considered to be related to a greater severity of rash and intensity of pain during the initial HZ episode.1133 Although the reason remains unclear, patients with persistent ZRP may be more immunocompromised or have more comorbid diseases, as suggested in previous reports.34 In addition, those patients tend to seek for medical attention for recurrence symptoms more frequently than patients with mild initial episodes.
Our study had some limitations. We cannot completely exclude misdiagnosed cases, because we identified HZ cases using computerized electronic medical records without detailed descriptions. Also, HZ cases were not confirmed by laboratory tests, but rather by disease code and prescription of antiviral medication. However, to our knowledge, this is the largest study for the recurrence of HZ and its various associated risk factors. Most of all, because NHIS-NSC 2002–2013 is a nation-representative sample database, comparing with other private insurance claim database with selection bias, we presume that the results in our study are similar to the actual natural history of HZ.
In conclusion, these results suggest that the recurrence of HZ is much more common than expected, and that the associated risk factors can play an important role in predicting recurrence and establishing vaccination guidelines for patients with an initial HZ episode.
 XML Download
XML Download