

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Kawasaki disease (KD) is a systemic inflammatory vasculitis primarily affecting children younger than 5 years old.1)2) It occurs worldwide, but mainly in East Asian countries, such as Japan, Taiwan, and Korea.3)4)5) It displays a constellation of clinical features with persistent fever (≥38°C; more than 5 days) and the following 5 principal symptoms: bilateral conjunctival congestion, erythema of the lips and oral cavity, polymorphous exanthema, changes in peripheral extremities, and non-purulent cervical lymphadenopathy (>1.5 cm).6) Although 50 years has passed since KD was first reported by Dr. Tomisaku Kawasaki, its cause is still unknown and its diagnosis is solely based on the clinical symptoms.1) The diagnostic criteria for complete Kawasaki disease (cKD) in the American Heart Association guidelines are a fever persisting at least 5 days with 4 or more principal symptoms.7) Patients with a fever lasting 5 days but with fewer principal symptoms are diagnosed with incomplete Kawasaki disease (iKD). Furthermore, because these symptoms are commonly seen in other diseases, the diagnosis of KD is not definitive. Hence, the clinical presentation of KD is heterogeneous. This clinical variability is also observed in the treatment response and the presence of complications. The standard treatment for KD is high-dose (2 g/kg) intravenous immunoglobulin (IVIG) during a 12-hour period with or without oral aspirin (30–80 mg/kg).7) However, 10–20% of patients do not respond to IVIG treatment.8) A coronary artery lesion (CAL) is present in 15–25% of untreated KD patients and in 3–5% of treated patients.9)10)11)
Although the etiology remains elusive, genetic factors are considered to play important roles in KD. The genetic association is strongly supported by the increased prevalence of KD in families, such as in twins, siblings, and the offspring of KD parents.12)13)14) Genome-wide association studies (GWASs) have identified several susceptibility genes associated with KD, including CD40 (rs4813003), Fc gamma receptor II a (FCGR2A; rs1801274), HLA-DQB2-HLA-DOB (rs2857151), and B lymphoid tyrosine kinase (BLK; rs2254546 and rs2736340).15)16)17)18)19) In our previous GWAS, we confirmed that BLK gene is the most significantly associated with KD in the Korean population as reported in the Japanese and Taiwanese population.17)18)20) Another KD-associated gene, FCGR2A was also significantly associated with KD in our sample set. Thus, to dissect the clinical and genetic heterogeneity of KD patients, we performed genetic association studies in several KD subgroups categorized by clinical characteristics using the very significant KD-associated variants rs6993775 (BLK) and rs1801274 (FCGR2A), which were detected in our GWAS of a high number of case (n=1,011) and control (n=4,553) samples (odds ratio [OR], 1.48; p=4.63×10−11 for BLK and OR, 1.26; p=1.42×10−4 for FCGR2A, respectively).20)
METHODS
Subjects
A total of 1,011 patients with KD were recruited from June 2008 to May 2015 from 12 tertiary academic hospitals in Korea that participated in the Korean Kawasaki Disease Genetics Consortium. All KD patients were diagnosed by pediatricians according to the diagnostic criteria of the American Heart Association.7) IVIG responders were defined as those who defervesced within 24 hours after completion of the initial treatment without recurrence of fever. KD patients were classified as having CAL if the diameter of the largest internal lumen diameter of the coronary arteries was larger than 3 mm (≥4 mm in patients older than 5)7)21) (Table 1). A total of 4,553 control subjects (1,862 males and 2,691 females) obtained from the adult health cohorts of the general population in Korea were used in our study. These control samples were provided by the Biobank for Health Sciences at the Center for Genome Science in Chungwon, Korea. The study protocol was approved by the Institutional Review Board of the Asan Medical Center (protocol number: 2014-0823, date: 08/14/2014) and written informed consent was obtained from all subjects or from the parents of all KD patients.
Table 1
Clinical characteristics of KD patients (n=1,011)
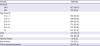
Values are presented as number (%).
CAL = coronary artery lesion; cKD = complete type of Kawasaki disease; iKD = incomplete type of Kawasaki disease; IVIG = intravenous immunoglobulin; KD = Kawasaki disease.
*Four patients had missing age data.
![]()
Genotyping of the single nucleotide polymorphisms rs6993775 (BLK) and rs1801274 (FCGR2A)
Genomic DNA was extracted from whole blood or lymphoblastoid cell lines according to the corresponding protocols. The genotypes of rs6993775 (BLK) and rs1801274 (FCGR2A) were obtained from our initial GWAS data consisting of 296 case samples and 4,553 control subjects, which were generated with Illumina Human Omni1-Quad BeadChips following the manufacturer's instructions (Illumina, San Diego, CA, USA). Additional genotyping of 715 case samples was performed on the high-throughput Fluidigm EP1 system (Fluidigm Corp., South San Francisco, CA, USA) using the Fluidigm single nucleotide polymorphism (SNP) Type™ assay platform according to the manufacturer's instructions. Genotype callings were made using the Fluidigm SNP Genotyping Analysis program (Fluidigm Corp.). The call rates of rs6993775 (BLK) and rs1801274 (FCGR2A) were 100% and 99.98%, respectively, in all 1,011 case samples and 4,553 control subjects.
Statistical analysis
The genetic associations of SNP were analyzed using PLINK (version 1.07) (http://zzz.bwh.harvard.edu/plink/).22) Statistical analysis of clinical variables was performed using SPSS, version 21 (SPSS, Chicago, IL, USA). The χ2 test was used to compare categorical variables. A 2-tailed p value less than 0.05 was considered statistically significant.
RESULTS
BLK (rs6993775) and FCGR2A (rs1801274) are very significantly associated with Kawasaki disease
In our GWAS involving a high number of case (n=1,011) and control (n=4,533) samples, BLK (rs6993775) was significantly associated with KD at a genome-wide significance level (OR, 1.48; p=4.63×10−11). FCGR2A (rs1801274) was also significantly associated with KD but did not reach the genome-wide significance threshold (OR, 1.26; p=1.42×10−4) (Table 2). Additionally, genetically enriched or clinically severe KD subgroups such as KD patients with family history, recurrence, or IVIG non-responders showed larger effect sizes with little or no statistical significance due to the small sample size (Table 2).
Table 2
Genetic association of BLK (rs6993775) and FCGR2A (rs1801274) with KD in KD subgroups

BLK = B lymphoid tyrosine kinase; CAL = coronary artery lesion; CI = confidence interval; cKD = complete type of Kawasaki disease; FCGR2A = Fc gamma receptor II a; iKD = incomplete Kawasaki disease; IVIG = intravenous immunoglobulin; KD = Kawasaki disease; OR = odds ratio; RAF = risk allele frequency.
*The RAF (risk allele: A; non-risk allele: C) of the control was 0.722 for BLK; †The RAF (risk allele: A; non-risk allele: G) of the control was 0.760 for FCGR2A; ‡The p<0.05 was considered significant and is denoted in bold; §The RAF and p for sex were calculated according to the sex specified. The RAFs for BLK were 0.719 and 0.725 for the male and female controls, respectively. The RAFs for FCGR2A were 0.758 and 0.761 for the male and female controls, respectively.
![]()
BLK (rs6993775) and FCGR2A (rs1801274) are not associated with Kawasaki disease in incomplete Kawasaki disease patients or those older than 5 years old
To genetically clarify the clinical heterogeneity of KD patients, we performed genetic association analysis in various clinical subgroups of KD patients according to their clinical characteristics (KD type, sex, age, presence of CAL, presence of family history, presence of recurrence, and IVIG responsiveness) using the variants of the well-known KD susceptibility genes BLK (rs6993775) and FCGR2A (rs1801274). Initially, we tried to identify any clinical subgroups showing significant genetic effects or none at all for either BLK or FCGR2A. BLK (rs6993775) was significantly associated with KD in all KD subgroups except iKD-type patients (OR, 1.23; p=0.211) and those older than 5 years old (OR, 1.15; p=0.302) (Table 2). FCGR2A (rs1801274) was significantly associated with the patients younger than 1 year, while a weak or no association was observed in other age groups, including those older than 5 years old (OR, 0.93; p=0.608) as well as iKD-type patients (OR, 1.05; p=0.794). In addition, after the exclusion of 222 KD patients (22% of all KD patients) with iKD or older than 5 years of age, a larger effect size and higher significance of BLK and FCGR2A were observed in genetic association analysis using a much smaller sample size (OR, 1.58; p=7.57×10−12 for BLK and OR, 1.37; p=4.66×10−6 for FCGR2A, respectively) (Table 3). The increased genetic significance was also observed in several KD subgroups in genetic association analysis after the exclusion of KD patients with iKD or those older than 5 years of age (Supplementary Tables 1 and 2).
Table 3
Genetic association of BLK (rs6993775) and FCGR2A (rs1801274) with KD after excluding iKD and/or patients ≥5 years old

BLK = B lymphoid tyrosine kinase; CI = confidence interval; FCGR2A = Fc gamma receptor II a; iKD = incomplete type of Kawasaki disease; KD = Kawasaki disease; OR = odds ratio; RAF = risk allele frequency.
*The RAF (risk allele: A; non-risk allele: C) of the control was 0.722 for BLK; †The RAF (risk allele: A; non-risk allele: G) of the control was 0.760 for FCGR2A; ‡The p<0.05 was considered significant and is denoted in bold.
![]()
The lack of a genetic association of BLK and FCGR2A in Kawasaki disease patients older than 5 years of age is due to an age group-specific effect
In a comparison of clinical features between cKD and iKD, we found that iKD had a significantly higher proportion of IVIG nonresponsiveness (1.87-fold, p=0.00166), CAL (3.11-fold, p<0.00001), recurrence (3.53-fold, p<0.00001), and age older than 5 years (1.95-fold, p=0.000967) (Supplementary Table 3). In addition, to understand the cause of the lack of a genetic effect of BLK and FCGR2A in KD patients older than 5 years of age, we examined the differences in the distribution of clinical characteristics between KD patients older than 5 years old vs. other age groups. We could not find any difference in clinical characteristics among age groups except the proportion of KD type. KD patients older than 5 years were twice as likely to have iKD (17.4% vs. 8.6%; p=0.00104) (Supplementary Table 4). However, no genetic association of BLK and FCGR2A was observed for either the cKD or iKD type in KD patients older than 5 years of age (Supplementary Table 5), indicating that the lack of a genetic association in KD patients older than 5 years of age is not due to the iKD type but to an age group-specific effect.
BLK (rs6993775) is associated with Kawasaki disease in all Kawasaki disease subgroups, whereas FCGR2A (rs1801274) is associated with Kawasaki disease mainly in male Kawasaki disease patients younger than 1 year old
Although both BLK and FCGR2A are associated with KD, the 2 genes do not exhibit the same genetic effects on KD susceptibility. To investigate the differential influence of BLK and FCGR2A, we compared the genetic association of both genes in several KD subgroups after excluding iKD patients and those older than 5 years of age. BLK was significantly associated with KD in all KD subgroups (Supplementary Table 1), whereas FCGR2A was significantly associated with male KD patients (OR, 1.52; p=4.50×10−6) and KD patients younger than 1 year old (OR, 1.71; p=1.91×10−4) (Supplementary Table 2). Sex-stratified genetic association analysis also showed that FCGR2A was significantly associated with male KD patients younger than 1 year old (OR, 2.17; p=6.69×10−5) (Table 4). On the other hand, in the initial association analysis using all KD patients (n=1,011), FCGR2A was significantly associated with KD in KD patients without CAL (OR, 1.31; p=6.77×10−5) but not in KD patients with CAL (OR, 1.08; p=0.507) (Table 2). However, after excluding iKD patients and those older than 5 years old, a significant association of FCGR2A with KD with the same effect size was observed in both KD patients without CAL (OR, 1.37; p=2.93×10−5) and with CAL (OR, 1.37; p=0.0421; Supplementary Table 2), indicating that FCGR2A acts as a KD susceptibility gene regardless of CAL in KD patients.
Table 4
Sex-stratified genetic association of FCGR2A (rs1801274) with KD in KD subgroups after excluding iKD and ≥5 years old

CI = confidence interval; FCGR2A = Fc gamma receptor II a; iKD = incomplete type of Kawasaki disease; KD = Kawasaki disease; OR = odds ratio; RAF = risk allele frequency.
*The RAFs (risk allele: A; non-risk allele: G) for FCGR2A were 0.758 and 0.761 for the male and female controls, respectively; †The p<0.05 was considered significant and is denoted in bold.
![]()
DISCUSSION
No specific and sensitive diagnostic test is available for KD. Thus, KD is diagnosed solely by clinical symptoms,7) which leads to considerable clinical heterogeneity. Although its high clinical heterogeneity is expected, analytical tools to dissect the clinical heterogeneity of KD are not available. To dissect the clinical heterogeneity of KD patients, in this study, we performed genetic association studies in several clinical subgroups of KD patients using the variants of the well-known KD susceptibility genes BLK and FCGR2A in our large sample sets. Although 4 KD susceptibility loci (FCGR2A, BLK, HLA-DQB2–HLA-DOB, and CD40) were previously identified through GWASs,15)17)18) 2 loci (CD40 and HLA region) were not replicated in our samples (data not shown). Furthermore, we selected an intronic SNP (rs6993775) in the BLK gene, instead of the promoter SNPs (rs2254546, rs2736340) that were identified in other GWASs17)18) because the intronic SNP (rs6993775) showed the most significant association with KD in our sample sets. The most significantly KD-associated genetic variants could help us to dissect the clinical and genetic heterogeneity of KD patients.
In our genetic association analysis in several clinical KD subgroups, there was no genetic association of BLK and FCGR2A in iKD patients and those older than 5 years old. In a genetic association analysis classified by the number of clinical symptoms within cKD or iKD, KD patients with 4 or 5 clinical symptoms (cKD) showed a very significant association with KD for both BLK and FCGR2A, unlike KD patients with 2 or 3 clinical symptoms (Supplementary Table 6). In addition, when we tested the type of clinical symptom in genetic association analysis, almost the same genetic effect was observed for each clinical symptom (data not shown). These results indicate that, instead of the type of clinical symptom, the number of clinical symptoms (at least more than 4 clinical symptoms) is a crucial criterion to diagnose KD. When we compared the distribution of clinical characteristics between the KD types (cKD vs. iKD), we found that iKD patients had a significantly higher proportion of IVIG nonresponsiveness, CAL, recurrence, and age older than 5 years (Supplementary Table 3). All of these clinical characteristics suggest that insufficient numbers of clinical symptoms in KD diagnosis can lead to the inclusion of an unknown disease that would not respond to IVIG treatment and subsequently has high IVIG resistance and CAL. Alternatively, it is also possible that insufficient numbers of clinical symptoms in KD diagnosis can delay the diagnosis and subsequently result in severe clinical outcomes, as previously reported.23) In particular, the presence of an extremely late clinical onset (≥5 years old) and IVIG nonresponsiveness as well as an insufficient number of clinical symptoms in iKD suggest that these iKD-type patients are a unique KD subgroup(s) with a different genetic background or have been misdiagnosed with KD. Furthermore, approximately 15–20% and 20–27% of KD patients have the iKD type in Japan3) and the United States,24) respectively. In addition, approximately 32.8% of KD patients have the iKD type in Korea.25) These results indicate that each country may have a different diagnostic power for the iKD type, with the high inconsistency due to the inclusion of patients with insufficient clinical symptoms. Therefore, special attention is required to diagnose iKD.
It was not clear why BLK and FCGR2A were not associated with KD in KD patients older than 5 years of age. However, our results indicate that the lack of a genetic association in KD patients older than 5 years of age is due to an age group-specific effect. Therefore, special consideration is required to diagnose KD in individuals older than 5 years of age. Unlike BLK, which showed a significant association in all KD subgroups, FCGR2A was strongly associated with KD only in male patients younger than 1 year of age (OR, 2.17; p=6.69×10−5; Table 4). FCGR2A encodes a low-affinity Fc gamma receptor that binds to the Fc portion of immunoglobulin G (IgG). The KD-associated variant rs1801274 (p.His167Arg, previously assigned as p.His131Arg) has been linked to autoimmune diseases such as systemic lupus erythematosus,26) and this variant is reported to affect its binding affinity for IgG2.27) The risk allele (A) of FCGR2A, encoding histidine, binds to IgG2 with high affinity, whereas the non-risk allele (G) shows little or no binding.28) The risk allele (A) in our study was reported to be the non-risk allele in systemic lupus erythematosus, which occurs more prevalently in females, suggesting that this variant has a sex-specific effect.29) In addition, it has been reported that the age-specific incidence rate was highest for infants aged 9–11 months and then gradually decreased with age.3) Furthermore, rare KD cases were observed in infants <3 months old and adults.2) These results suggest that passive immunity in infants and the age-specific development of immunity play a protective role in KD.
One advantage of this study is that the sample size is large enough (1,011 cases vs. 4,553 controls) for subgroup analysis, particularly for the BLK gene variant (rs6993775) showing the most significant association with KD (p=4.63×10−11) in our sample sets. However, in the case of FCGR2A, we had limited power for subgroup analysis due to its lower significance in KD (p=1.42×10−4). Another advantage is that our sample was clinically homogeneous due to the use of standardized clinical data specifically collected from Korean patients from multiple centers. Homogeneity of disease phenotype and a large sample are considered 2 important factors for genetic analysis. Nonetheless, many genetic association studies undervalue the effect of clinical heterogeneity and rely on large sample sizes for detecting risk alleles of diseases. In our study, we considered both a large sample size and clinical homogeneity and demonstrated that well-known KD-associated genetic variants are very useful for dissecting the clinical heterogeneity of KD and differential genetic effects in several clinical KD subgroups using large sample sets.
In summary, KD is a clinically and genetically heterogeneous disease. We found that the KD-associated variants BLK (rs6993775) and FCGR2A (rs1801274) were not associated with KD in iKD patients and those older than 5 years. After excluding iKD patients and those older than 5 years old, we found that BLK was associated with KD in all KD subgroups, whereas FCGR2A was specifically associated with male KD patients younger than 1 year old. Our findings will help us to better understand the clinical and genetic heterogeneity of KD.
 XML Download
XML Download