

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Compared to adults, facial fractures are uncommon injuries in the pediatric population. The incidence is even rarer in children younger than five years of age. It is estimated that only 1% of facial fractures occur in toddlers and preschool-aged children. Pediatric and teenage maxillofacial trauma account for about 15% of all maxillofacial trauma1234.
Research investigation has shown that the mandible is the most commonly fractured facial bone3456789. Mandibular fractures in children may lead to serious complications like asymmetric mandibular growth, temporomandibular joint ankylosis, and malocclusion. In general, soft tissue injuries are more common in children than skeletal fractures. Worldwide, falls from height, road traffic accidents (RTA), sports-related injuries, and bicycle accidents are the leading causes of mandibular fractures in the pediatric population. The incidence and patterns of mandibular fractures vary with geographical location, socioeconomic conditions, and the age of the population10. The majority of previous studies have focused on maxillofacial trauma in the adult population. These reports have shown that RTA is the most common mode of maxillofacial fractures in developing countries, while interpersonal violence accounts for the majority of such cases in developed countries679111213. The purpose of this retrospective study was to evaluate the etiologies and patterns of mandibular fractures in children who reported to a tertiary care center in Kolkata, India between 2012 and 2016.
Go to : 
II. Materials and Methods
A retrospective study of mandibular fracture was performed in patients who presented with maxillofacial trauma to the Department of Pedodontics and Preventive Dentistry of the Dr. R. Ahmed Dental College & Hospital, Kolkata, from July 2012 to June 2016. This institute is affiliated with the West Bengal University of Health Sciences, Kolkata in India. The study was reviewed and approved by the ethical committee of the institute of Dr. R. Ahmed Dental College & Hospital. In this study, information was obtained from the injury report register and entered in a data collection sheet. We reviewed all patients aged 12 years and younger at the time of mandibular fractures. The subjects were divided into three groups: Group A (0–5 years), Group B (6–9 years), and Group C (10–12 years). Patients were categorized based on age, sex, place of residence, fracture mechanism, anatomic location of fracture and date of trauma. The trauma etiology was classified as fall from height, RTA, play- or sports-related injury, bicycle accident, assault, or other. The anatomical sites of the mandibular fractures were determined by panoramic and/or computed tomographic examination of the patients. Furthermore, mandibular fracture sites were classified according to Killey14: symphyseal, parasymphyseal, body, angle, ramus and condyle. Patient charts with incomplete information, extensive head injury and the presence of pathology were excluded from the study.
The results were tabulated and analyzed using the Epi Info (ver. 7; CDC-INFO, Atlanta, GA, USA). Descriptive analyses including frequency, percentage, and proportions were performed. Where appropriate, the significance of the findings was evaluated using the z-test and chi-square test. The level of significance was set at P<0.05.
Go to :
III. Results
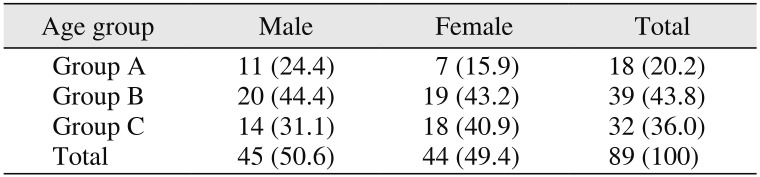
1. Age and sex distribution
A total of 202 cases of maxillofacial trauma records were extracted for review. Among them, 89 pediatric patients (44.1%) sustained mandibular fractures. Of the 89 patients, 45 patients (50.6%) were male and 44 patients (49.4%) were female with a male to female ratio of 1.02:1. The mean patient age (7.73±3.02 years; 95% confidence interval [CI], 7.1–8.36) was slightly higher in females (8.20±3.02 years; 95% CI, 7.31–9.1) than in males (7.26±2.89 years; 95% CI, 6.39–8.14). However, this difference was not statistically significant (z for 95% CI=1.96). Most patients belonged to Group B (39 patients, 43.8%), followed by Group C (32 patients, 36.0%) and Group A (18 patients, 20.2%).(Table 1)
2. Place of residence
There were significantly (P=0.0103, Fisher exact test) more fracture cases (50 patients, 56.2%) reported from rural areas than from urban areas (39 patients, 43.8%) of residence.
3. Mandible fracture etiology
The causes of mandibular fractures are shown in Table 2. Most of the mandibular fractures were caused by falls (40 patients, 44.9%), and other causes included RTA (22 patients, 24.7%), play (16 patients, 18.0%), bicycle accident (8 patients, 9.0%), and violence (2 patients, 2.2%). Only one male patient (1.1%) in Group C sustained a mandibular fracture due to trauma from a tube well handle.

Table 2
Mandibular fracture etiologies by age group
![]()
4. Fracture distribution
The distribution of fractures is shown in Table 3. A total of 131 fracture locations were observed in 89 patients. The majority of fractures (70 patients, 53.4%) occurred in males. Approximately half of these fractures, (62 patients, 47.3%) were seen in Group B, followed by Group C (44 patients, 33.6%) and Group A (25 patients, 19.1%). There were 20 boys and 26 girls, a total of 46 patients (51.7%) that reported a single fracture location and 43 patients (48.3%), 25 boys and 18 girls presented with multiple fractures. However, no significant sex difference (P=0.20, Fisher exact test) was observed in the distribution of fractures. The most common site was the condylar region (38.9%) followed by angle (20.6%), parasymphysis (18.3%), body (15.3%), and symphysis (5.3%). Fracture of the ramus (1.5%) was observed only in Group C. There were no coronoid fractures observed in our study. Multiple fractures were most commonly observed in the condylar and parasymphyseal regions.
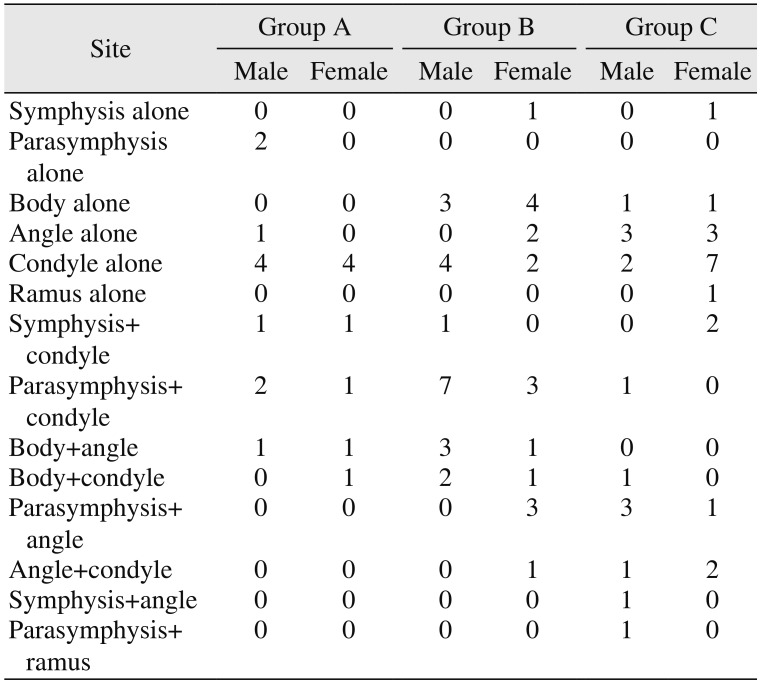
Table 3
Fracture distribution by age group (n=89)
![]()
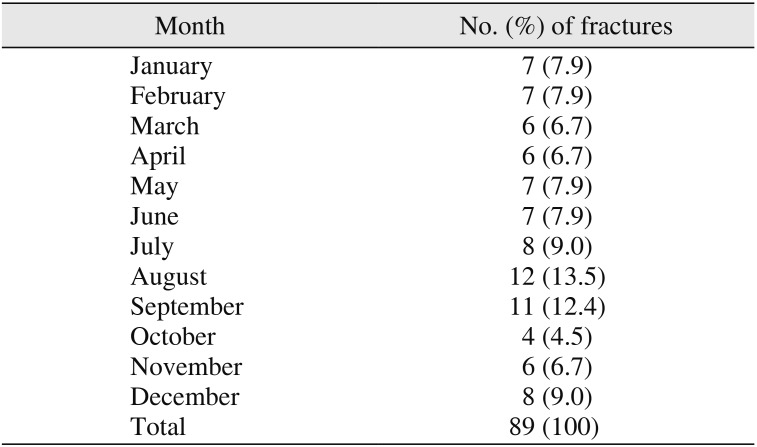
5. Month-wise distribution
With regard to the month-wise distribution of mandibular fractures, the maximum number of cases was reported in August (12 patients, 13.5%) and the minimum number of cases was documented in October (4 patients, 4.5%).(Table 4)
Go to :
IV. Discussion
Maxillofacial trauma is one of the principal causes of morbidity and mortality in children. Mandibular fractures at young ages may lead to functional impairment and disfigurement. Patterns and etiologies of mandibular fractures vary by geographical location, cultural characteristics, and socioeconomic status. The majority of investigations have shown that males are more prone to maxillofacial trauma than females in all age groups345781516. Generally, the male to female ratio of maxillofacial trauma and mandibular fractures is 2:1. In contrast, the results of our study showed no significant sex bias. Cole et al.15 concluded that at a young age, the etiology of mandibular fractures is similar in both sexes. Therefore, sex-related fracture differences are less significant at a young age.
In this study, only 20.2% of fractures were reported in children below five years of age. This is consistent with the results of other investigations that also reported that maxillofacial trauma is uncommon in toddlers and preschool age children237815. This could be attributable to the fact that the younger age groups experience more parental supervision and less independence than older children. In addition, the retruded position of the face in relation to the skull, a greater cranium to face ratio in infants and toddlers, lack of pneumatization of nasal bones and greater flexibility of facial bones may contribute to a lower incidence of maxillofacial fractures in this age group. In our study, most injuries (39 patients, 43.8%) occurred in the 6 to 9 years age group. Several factors, like facial skeleton growth, participation in school activities, and an increase in social interaction may increase the risk of maxillofacial trauma in this age group.
The results of this study support the finding of a study by Namdev et al.16, who also observed the majority of mandibular fracture cases in rural areas. Poor road conditions in some parts of rural India, especially during the rainy season, may have contributed to an increased incidence of maxillofacial trauma.
Falls from height (44.9%) were the major cause of mandibular fracture in this study. Our results are in agreement with the observations of Collao-González et al.5, Joshi et al.8, Namdev et al.16, Owusu et al.17, Kumaraswamy et al.18, and Atilgan et al.19, who also reported that falls from height were the most common mechanism of maxillofacial trauma in children. In this study, more than half of the population in Group A and Group B sustained mandibular fractures due to falls from height, representing low velocity/energy trauma. Kumaraswamy et al.18 observed that in children up to 6 years of age, falls in the home were the most common mode of maxillofacial trauma, and with increasing age and more outdoor exposure, falls tended to occur outside the home.
This study demonstrated that RTA was the second most common cause of mandibular fracture. Some reports have shown that RTA is the main etiology of trauma3720. A recent Indian study by Singhal et al.7 also reported that RTA was the most common mode of maxillofacial trauma (57.27%) in children and adolescents. In this report, motor vehicle as well as motorbike accidents were categorized as RTA, and accounted for approximately 25% of fracture cases. In addition, 9.0% of mandibular fractures occurred secondary to bicycle accidents. One reason for mandibular fractures due to RTA might be the lack of helmet use by children while traveling in motorbikes. Furthermore, the use of seat belts and airbags as safety measures is limited, especially in semi-urban and rural parts of India where traffic rules are not strictly enforced.
In the present study, play- or sports-related injuries increased with age and the highest incidence was observed in the 10 to 12 years age group. Muraoka et al.21 also reported similar trends among Japanese children. A rise in fracture incidence during puberty and adolescence may be due to increased involvement in sports.
Schlievert22 and Knoche et al.23 reported child abuse to be one cause of mandibular fractures in children. In this study, we did not identify child abuse as a mechanism for mandibular fractures, which was similar to the pattern observed by Namdev et al.16 and Fasola et al.24. In comparison, Almahdi and Higzi3, Gassner et al.10, Atilgan et al.19, and Tanaka et al.25 found that interpersonal violence is an important etiology for pediatric facial fractures. Additionally, Bamjee26 reported assaults and gunshot wounds to be the cause of mandibular fracture in 48% of patients. In contrast, only two cases of mandibular fractures due to assaults or interpersonal violence were observed in this study. The higher incidence of mandibular fractures caused by assaults in previous studies may be attributed to differences in socioeconomic factors, behavioral habits, and the inclusion of adolescents in the study population.
In this study, the condylar region was the most common site of mandibular fracture. Our results are in agreement with the observations of other studies reporting the condyle as the most common fracture site of the mandible. In preschool children, condylar fractures accounted for the majority of cases (52%) and the incidence decreases with increasing age. The condylar process in children has high bone marrow content and the cortex is relatively thin. Therefore, this causes low resistance to low velocity trauma during fall. Overall, condylar fractures in the present study accounted for 39% of all mandibular fractures. This is comparable with the results of Almahdi and Higzi3 (29.8%), Joshi et al.8 (40.9%), Namdev et al.16 (40.3%), Owusu et al.17 (27.9%), and Shi et al.27 (55.7%). In addition, approximately half of patients (48.3%) presented with fractures at more than one site. Multiple fractures most commonly involve the parasymphyseal and condylar regions. Patients with RTA as the main etiology for mandible fractures have reported the parasymphysis and condyle to be common fracture sites9.
Haug and Foss2 concluded that mandibular angle fractures are rare in children and adolescents. Shi et al.27 reported mandibular angle fractures in only 3.5% of cases, which primarily occurred in patients with permanent dentition. In our study, the mandibular angle was the second most common fracture site and the incidence of fracture to this area increased with age. This finding is supported by the observations of Almahdi and Higzi3, Owusu et al.17, and Thorén et al.28, who also reported that mandibular angle fractures consistently increased with age. In addition, the overall incidence of fractures of the parasymphysis (18.3%) and body (15.3%) were comparable with the results of Muñante-Cárdenas et al.4 who observed similar incidences of fractures of the parasymphysis (18.7%) and body of the mandible (15.1%).
In this study, the incidence of mandibular fractures was highest in August, although it was relatively constant with seasonal variations. This is in agreement with the results of Joshi et al.8, Haug and Foss2, and Tanaka et al.25 who also observed that month-wise distribution of mandibular fractures remains fairly constant with seasonal variations. Jung et al.29 reported that the highest incidences of fractures occurred during the months of autumn and that the January was the month with the lowest reported incidence. In contrast to our findings, some studies have reported that the monthly distribution of maxillofacial fractures peaked in summer3031.
The limitations of the present study include the retrospective nature and small sample size. In spite of these limitations, our results show the epidemiology and patterns of mandibular fractures in the eastern parts of India. We hope that the results of our study will provide insight for healthcare providers to formulate preventive strategies.
Go to :
V. Conclusion
The results of this study indicated that there was no significant difference in the incidence of mandibular fractures according to sex. Another distinguishing feature of this study was a high incidence of fractures in rural populations. Our finding that condylar fractures were the most common type of fractures and that falls are the primary causes of mandibular fractures was supported by the majority of published data. In addition, RTA and bicycle accidents account for approximately one-third of cases, indicating the need for strict implementation of traffic rules.
Go to :
 XML Download
XML Download