

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Restless legs syndrome (RLS) is a sleep-related neurological disorder characterized by an urge to move the legs due to unpleasant sensations. RLS usually occurs at rest, worsens at night, and is relieved by movement of the affected limbs.1 RLS was also known as Willis-Ekbom disease, named after Dr. Thomas Willis, an English physician whose first case report was published in 1685, and Dr. Karl Axel Ekbom, a Swedish neurologist who introduced this term for the disease and described how to diagnosis it in 1945.2
The standard diagnostic criteria of RLS were first proposed by the International RLS Study Group (IRLSSG) in 19953 and revised in 2002.1 RLS commonly occurs secondary to various medical conditions such as end-stage renal disease, peripheral neuropathy, iron deficiency, and pregnancy.4 The impact of RLS can be mild to severe, with adverse effects on sleep quality, cognitive functions, mood, and quality of life.5
While pregnancy-related RLS has been well described, its prevalence, natural course, and pathophysiology have not been identified.6 Recent systemic reviews found that the prevalence of RLS during pregnancy ranges between 11% and 34%,78910111213 which is typically two to threefold higher than in general nonpregnant women.4 Furthermore, the prevalence of RLS during pregnancy was reported to peak in the third trimester and may be related to the parity.9 These data were assessed from the pooled prevalence mostly in American, European, and East Asian countries, and have been lacking from the Southeast Asia.13
Possible mechanisms underlying the pathophysiology of pregnancy-related RLS have been proposed. These include iron and folate deficiency due to a dilution effect and utilization for fetal development, hormonal changes, psychological conditions, lumbosacral radiculopathy, and peripheral venous congestion in pregnancy.4 Since RLS has a negative impact on the quality of sleep, RLS may result in a higher risk of pregnant women developing pregnancy and delivery complications, and of adverse effects on fetal development.514
A population-based epidemiological study has not been performed previously among pregnant Thai women. Therefore, the primary aim of this study was to estimate the prevalence, natural course, and predictive factors of RLS in pregnant Thai women. The secondary aim was to determine the effect of RLS on sleep quality in pregnant women.
Go to : 
METHODS
This cross-sectional retrospective study enrolled pregnant Thai women who attended Thammasat University delivery unit from October to December 2017. Three hundred and fifty-four pregnant women older than 15 years were interviewed. Of those, 131 pregnant women were excluded due to non-Thai citizenship or no data available for the history of antenatal care. Women who were admitted to a private ward or had severe pregnancy complications such as preeclampsia and miscarriage were excluded. Finally, 214 pregnant women were enrolled. All subjects received regular obstetrical care by their physician, and no alteration of obstetrical care was recommended or mandated for any of them. Our study was approved by the Human Research Ethics Committee of Thammasat University (IRB No. MTU-EC-IM-0-046/60).
The study participants were diagnosed with RLS in a face-to-face interview with a neurologist during their admission for labor and delivery care. RLS was diagnosed according to the revised criteria of the IRLSSG.1 General demographic data were collected, including the antenatal-care history, routine blood test results, and past medical illnesses. Scores on the Thai versions of the Epworth Sleepiness Scale (ESS) and Pittsburgh Sleep Quality Index (PSQI) were determined.15 Pregnant women who fulfilled the IRLSSG diagnosis criteria were diagnosed as having pregnancy-related RLS. RLS-positive participants were also questioned about the onset, duration, and severity of RLS. The IRLSSG Rating Scale (IRLS) was used to evaluate the severity of RLS.16 Furthermore, participants diagnosed as having pregnant-related RLS were followed for postpartum symptoms and complications for 6 weeks.
Maternal and neonatal outcome data
The antepartum medical records of all enrolled participants and their newborns were collected, including delivery type, birthweight and sex of the newborn, Apgar scores at 1 and 5 minutes, and immediate postpartum complications. The continuous variables were summarized as mean±SD values, and categorical variables were summarized as number (percentage) values. Quantitative data were compared using student's t-test, and qualitative data were compared using the χ2 test. Multiple regression analysis was applied to identify significant predictive factors of RLS. A p value of less than 0.05 was considered statistically significant.
Go to :
RESULTS
This study included 214 pregnant women aged 28.60±6.52 years and with an age range of 15–45 years. Demographic and clinical characteristics of the study participants with and without RLS are provided in Table 1.
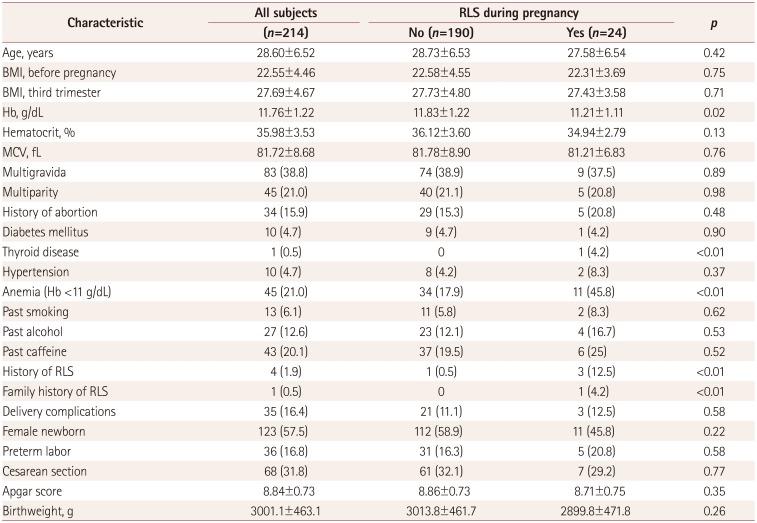
Table 1
Demographic and clinical characteristics of the study subjects with and without RLS
![]()
Comparisons of participants with and without RLS during pregnancy
RLS was diagnosed in 24 of the pregnant women, indicating an RLS prevalence rate of 11.2%. Comparison of the data among the RLS and non-RLS groups revealed no significant differences in the age, body mass index, gravidity, parity, and maternal and childbearing history. In addition, personal behaviors such as the history of smoking, alcohol, and coffee consumption did not differ significantly between the two groups. The hemoglobin level (Hb) during pregnancy was significantly lower in the RLS group than in the non-RLS group (11.21±1.11 vs. 11.83±1.22 g/dL, p=0.02). The hematocrit and mean corpuscular volume were also lower in the RLS group; however, the differences were not statistically significant. The incidence rates of anemia during pregnancy (defined as an Hb of less than 11 g/dL), thyroid disease, previous history of RLS, and family history of RLS were significantly higher in the RLS group (p<0.01) (Table 1). Multiple logistic regression analysis revealed that Hb less than 11 g/dL [odds ratio (OR)=3.21, 95% CI=1.27–8.13] and a history of RLS (OR=16.62, 95% CI= 1.52–181.32) were associated with RLS during pregnancy (Table 2).

Table 2
Results from a multiple logistic regression model with variables for RLS during pregnancy
![]()
In terms of sleep quality, 75% of pregnant Thai women were considered as poor sleepers according to the Thai-PSQI global score.15 Comparing the data between the RLS and non-RLS groups revealed no significant differences regarding Thai-PSQI sleep quality, latency, duration, habitual sleep efficiency, disturbances, use of medication, daytime dysfunction subscore, or global score (8.63±3.71 vs. 7.77±3.21, p=0.26). Subjects with RLS reported a longer sleep onset latency than those without RLS, but the difference was not statistically significant (54.79±58.08 vs. 40.55±36.55, p=0.09). Thai-ESS scores were significantly higher in the RLS group (3.04±1.49 vs. 1.54±1.33, p<0.001) (Table 3) and were associated with gravidity, parity, history of RLS, and alcohol consumption. However, only the presence of RLS during pregnancy was associated with a high Thai-ESS score in a multivariate analysis (Table 4).
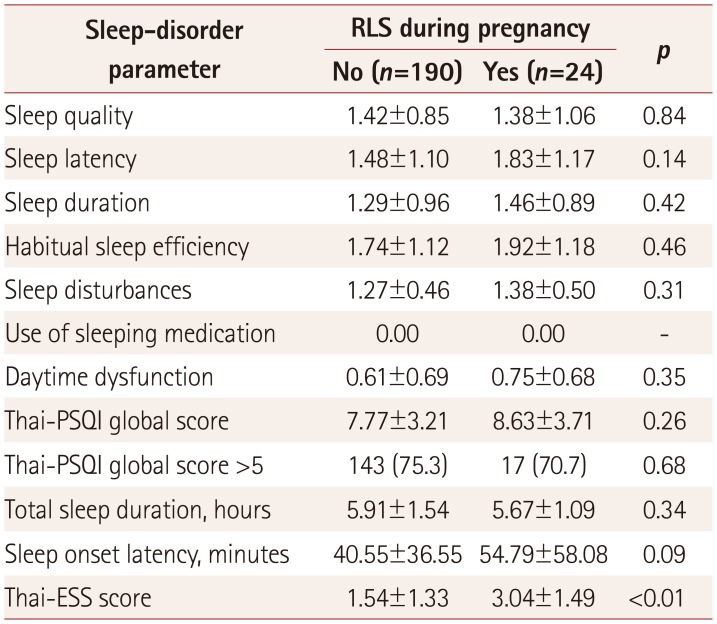

Table 3
Scores on the Thai versions of the PSQI and ESS in the RLS and non-RLS groups
![]()
Table 4
Results from a multiple linear regression model of a high Thai-ESS score
![]()
Natural course of RLS during pregnancy
The proportions of participants having RLS during different trimesters among the 24 pregnant Thai women enrolled in the study were as follows: 4.2%, 25.0%, and 70.8% in the first, second, and third trimesters, respectively. All of the subjects who developed RLS during pregnancy reported that their symptoms had persisted through the third trimester, with a duration of 2.08±1.25 months (range=1–6 months). The demographic variables did not differ significantly among subjects with RLS starting in the first, second, and third trimesters. All subjects with RLS scored within the range of severe symptom severity according to the IRLS (range=22–30).16 There was no significant factor related to the severity of symptoms among the RLS subjects. After delivery, eight participants (33.3%) continued experiencing RLS symptoms, indicating that the prevalence of RLS decreased significantly to 3.7%. The symptoms disappeared within a few days in seven of these participants, and within 1 week in the eighth. None of the subjects required pharmacological treatment other than the standard iron and supplements during antenatal-care visits. There were no intergroup differences in delivery type, complications, Apgar scores, birthweight, or sex of the newborn.
Go to :
DISCUSSION
The prevalence of pregnancy-related RLS found in this study is consistent with previous reports of 11.2% to 12.3% in the Chinese population,917 which is lower than the prevalence found in pregnant European and Scandinavian women.812 Based on a recent systemic review and meta-analysis, this could be the first report on the prevalence in the Southeast Asia.13 The differences in prevalence can be attributed to several factors: 1) the ethnicity of the study population, since the general prevalence of RLS is reportedly lower in Asians than in Caucasians, 2) women with mild RLS symptom severity may remain undiagnosed due to them being unaware of their symptoms, and 3) the prevalence rate in our study is based on interviews performed during the third trimester.
Regarding risk factors, our study found that anemia and a previous history of RLS were risk factors for developing RLS during pregnancy, which is similar to the findings of previous studies.49 This reflects the underlying pathophysiology of iron and folate depletion during pregnancy. Since the symptoms disappeared rapidly after delivery, the depletion may be the result of a dilution effect rather than an absolute iron and folate deficiency. Future studies should evaluate the serum levels of iron and ferritin in general pregnancies, and women who develop iron deficiency anemia during pregnancy should be adequately treated with iron supplementation. Other hypotheses associated with the pathophysiology of RLS during pregnancy such as genetic susceptibility, hormonal changes, or psychological conditions were not evaluated in this study.
Concerning sleep quality, the subjects with RLS had a relatively higher Thai-PSQI global score and longer sleep onset latency than those without RLS, but the difference was not statistically significant. This may have resulted from the high incidence of poor sleepers (Thai-PSQI global score >5) among general pregnant Thai women. Sleep problems including in conditions other than RLS during pregnancy should be explored, and there should be a focus on providing education about healthy sleep behaviors. Excessive daytime sleepiness may occur during pregnancy and be related to the RLS frequency as a result of poor nighttime sleeping.17 In our study, pregnant women with RLS were more likely to experience daytime sleepiness than were those without RLS, but none of them had significant problems with daytime sleepiness.
Regarding pregnancy-associated complications and delivery outcomes, no significant differences were seen between the RLS and non-RLS groups. Since RLS during pregnancy is transient and has a benign course, providing information about RLS and natural course to pregnant women are needed.
We acknowledge that our present study has some limitations. First, our study based on one center and the number of participants was limited. Even though the study population was adequate to estimate the RLS prevalence, it was too small to identify the certain predictive factors of RLS during pregnancy. A prospective, multicenter registry with a larger sample size should be considered in the future. Second, the diagnosis of RLS was based on the recalled data during the third trimester of pregnancy. Third, the levels of iron and ferritin were not evaluated in the study. Further research on iron metabolism and pregnancy-related RLS pathophysiology is needed. Fourth, major pregnancy and delivery complications were excluded from the study. Last, environmental factors that could affect the quality of sleep were not controlled. A standard sleep monitoring with polysomnography should be considered.
In conclusion, our study confirmed a high prevalence of RLS and its impacts on sleep in pregnant Thai women. Anemia and history of RLS are predictors of developing RLS during pregnancy. RLS is commonly found in the second to third trimesters of pregnancy. In general, pregnancy-related RLS is benign. The symptoms usually transient and disappear within a few days after delivery. There was no immediate labor or newborn complications associated with RLS.
Go to :
 XML Download
XML Download