

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The primary aim of operative treatment in most epilepsy surgery candidates is to cure (or at least reduce) seizures, which leads to substantial improvement in the quality of life. Minimizing the adverse effects of antiepileptic drugs (AEDs) or reducing the exposure time to AEDs are also important treatment issues in pediatric epilepsy. When children achieve seizure freedom after epilepsy surgery, the benefits of AED withdrawal are weighted against the risk of seizure recurrence after withdrawal. AED withdrawal can avoid unnecessary long-term toxicity of the drugs and improve cognitive processing and neuropsychological performance.1234
Seizure recurrence after planned AED withdrawal is another important consideration. Some patients experience seizure recurrence during AED reduction, whereas others experience relapse after AED withdrawal. Several predictors of seizure recurrence after AED withdrawal have been reported in the literature. Early AED withdrawal,567 older age at surgery,5 longer duration of epilepsy,78 seizure recurrence before withdrawal,7910 incomplete resection,1112 and an abnormal postoperative EEG81213 are known risk factors for seizure recurrence subsequent to AED withdrawal. However, a meta-analysis of predictors of relapse after AED withdrawal did not produce consistent results, largely because of the extreme heterogeneity in patient populations, types of epilepsy surgery, and postoperative follow-up durations.14
Focal cortical dysplasia (FCD) is the most-common cause of medically intractable focal epilepsy in childhood. Most of the pediatric surgical cohorts have included a considerable number of children with low-grade glioma and vascular malformations besides FCD.612 It is widely accepted that the pathophysiological basis of epileptogenesis or pathological substrates would determine the surgical outcomes.
We focused on the surgical outcome after AED withdrawal in children with FCD. In this study we aimed to determine the seizure recurrence rate after planned AED withdrawal, to measure the chances for regaining seizure freedom after AED reintroduction, and to identify potential predictors of seizure recurrence after drug withdrawal.
METHODS
Patients
We retrospectively reviewed the records of patients who underwent resective epilepsy surgery at the Seoul National University Children's Hospital (Seoul, Korea) between 2004 and 2015. The included patients underwent surgery at <18 years of age, were followed for at least 2 years after surgery, and were pathologically diagnosed with FCD type I, II, or IIIa based on the International League Against Epilepsy classification.15 To assemble a uniform cohort, patients with tumor-related epilepsy, vascular malformations, infections, and ischemic changes were excluded. Patients who underwent functional hemispherectomy or corpus callosotomy were also excluded. This study was approved by the local Institutional Review Board (IRB No. 1804-140-941). Given the retrospective nature of the study, the requirement to obtain informed consent was waived.
Preoperative evaluations and surgery
All patients underwent standard presurgical evaluations, including the detailed clinical history, a physical examination, scalp and video-EEG according to the 10–20 system, and high-resolution brain MRI with a 1.5- or 3-tesla epilepsy protocol. Intracranial EEG monitoring was performed when noninvasive investigations failed to localize the extent of the epileptogenic zone or suggested the wide involvement of extralesional areas, or the epileptogenic zone involved highly eloquent areas. Functional imaging such as ictal SPECT, interictal fluorodeoxyglucose PET, and magnetoencephalography was performed when clinically indicated. The type and extent of the resection were decided based on the presumed epileptogenic zone. Complete resection was defined if the region of the structural abnormality on MRI or the epileptogenic zone presumed from intracranial EEG was entirely removed.
Postoperative management
Seizure recurrence was ascertained in a personal interview with each patient. Acute postoperative seizures within the first 2 weeks after surgery were not considered as part of the recurrence. When patients were seizure-free for at least 6 months after surgery, we discussed with them or their caregivers about the benefits of AED withdrawal and the likelihood of seizure recurrence. The decision to discontinue AEDs was always only made after discussion, and only with consent from the patients or their caregivers. The timing of AED withdrawal and AED reduction rates were decided on an individual medical basis. The dose was reduced in a stepwise manner every 2 to 3 months. Postoperative EEGs were obtained on individualized schedules. We selected data from a single EEG recording session that was performed closest to 3 months postoperatively.
Statistical analysis
Descriptive statistics were used for demographic data. Patients with and without seizure recurrence on AED tapering were compared using the Fisher's exact test and Mann-Whitney U test. The time to an event after surgery was plotted as a Kaplan-Meier survival curve to estimate the probability of seizure freedom after surgery. Also, logistic regression analysis with the forward stepwise (likelihood ratio) method was used to evaluate risk factors for seizure recurrence after a planned AED withdrawal. Odds ratio and 95% CIs were also calculated, with p<0.05 considered statistically significant. All analyses were performed using SPSS (version 22.0, IBM Corp., Armonk, NY, USA).
RESULTS
Cohort characteristics
Seventy patients (37 males and 33 females) were eligible for the present analysis. The clinical characteristics and preoperative and operative variables for the entire cohort are summarized in Table 1. The age at seizure onset was 4.91±3.66 years (mean±SD), the duration of epilepsy was 5.27±3.82 years, and the follow-up duration after surgery was 5.45±2.77 years. The patients were taking a median of 2.5 AEDs. Of the 70 patients, 58 patients (82.9%) exhibited focal lesions including hippocampal sclerosis on MRI, and 45 patients (64.3%) received intracranial EEG monitoring. All except 6 patients underwent resection confined to a single lobe: temporal lobes in 36, frontal lobes in 19, parietal lobes in 5, and occipital lobes in 4. Forty-five patients (64.3%) underwent complete resection.
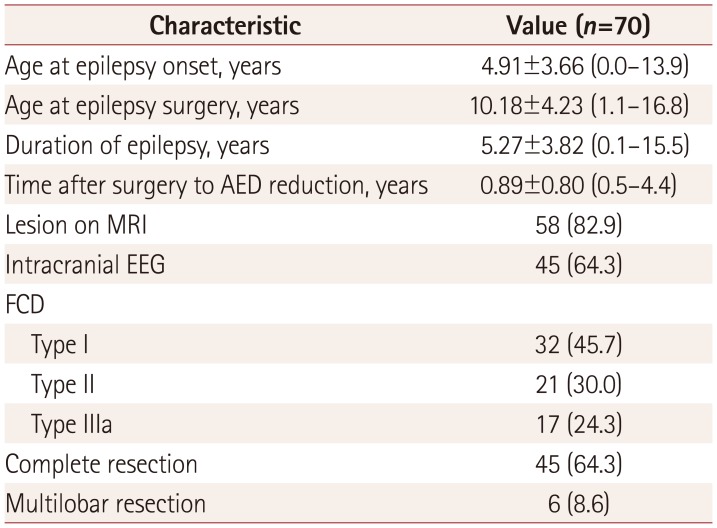
Table 1
Clinical characteristics of the overall cohort
![]()
Seizure outcomes
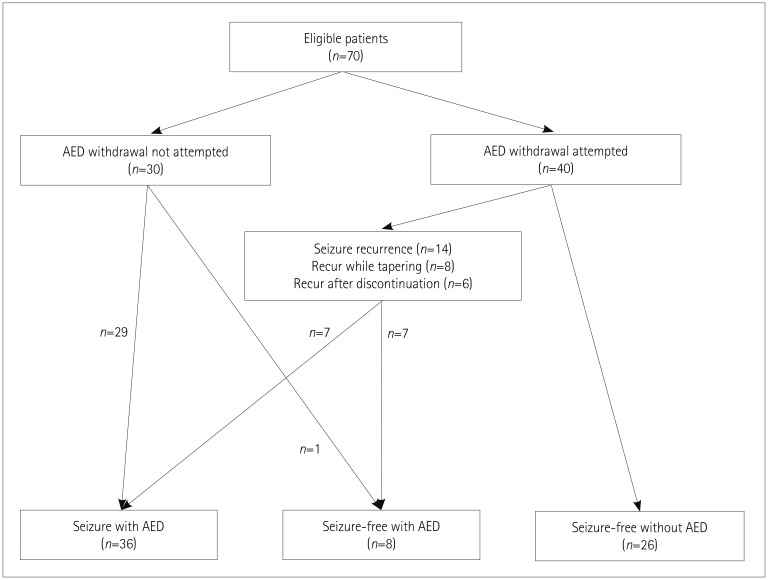
The longitudinal seizure and AED therapy outcomes in the overall cohort are illustrated in Fig. 1. AED withdrawal was attempted in 40 patients; the remaining 30 continued to receive medication throughout the follow-up period. One of these 30 patients was seizure-free for 4 years after surgery, but opted to remain on AED due to a fear of relapse. Over the follow-up period of 4.54±2.20 years (range, 2–12 years), 26 patients (37.1% of the entire cohort) achieved a seizure-free status without AEDs, and 8 patients (11.4% of the entire cohort) were seizure-free with AEDs. Twenty-six patients achieved a seizure-free and AED-free status at a mean follow-up period of 4.9 years after surgery, which was 4.1 years after starting AED withdrawal. One of the 26 patients experienced rare seizures after surgery and became seizure-free as a result of the runningdown phenomenon, and was able to discontinue AEDs.
Seizure recurrence after AED withdrawal
Seizure recurred in 14 (35%) of the 40 patients who started AED withdrawal. The median time of starting AED tapering after surgery was 10.8 months (range, 6 months to 4.4 years). The clinical characteristics of patients who experienced seizure recurrence on AED withdrawal (n=14) were compared to those without recurrence (n=26) (Table 2). The rates of incomplete resection (p=0.001) and postoperative epileptic discharges (p=0.018) were significantly higher in patients who experienced seizure recurrence, while the timing of starting the AED taper did not differ between patients who did and did not experience recurrence (p=0.251). The timing of seizure recurrence in relation to AED withdrawal is depicted in Fig. 2. Seizures recurred while reducing the AED dose in 8 patients and after discontinuation in 6 patients. Seizures recurred at a mean of 9.6 months after AED withdrawal (range, 20 days to 2.3 years) in patients who recurred while the AED dose was being reduced, and at a mean of 4.2 years after the start of AED withdrawal (range, 1.2–8.5 years) in those who experienced relapse after AED discontinuation.

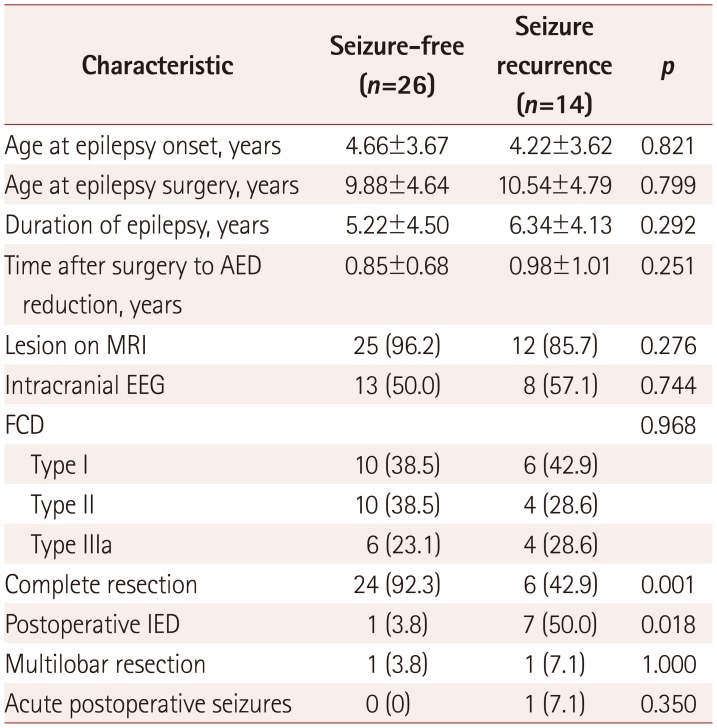
Fig. 2
Differential Kaplan-Meier survival curves for the timing of seizure recurrence in patients with recurrence on AED reduction (red dotted line) versus recurrence after AED discontinuation (blue solid line). AED: antiepileptic drug.
![]()
Table 2
Clinical characteristics of patients with and without seizure recurrence after drug withdrawal
![]()
Chance of regaining seizure freedom after AED reintroduction
Half of the 14 patients who experienced postwithdrawal seizure recurrence regained seizure freedom after AED reintroduction. They achieved seizure freedom for a mean duration of 2 years (range, 3.6 months to 6.2 years) (Supplementary Table 1 in the online-only Data Supplement). Three of the 8 patients who experienced recurrence while reducing the AED dose became seizure-free after AED reintroduction. In addition, 4 of the 6 patients who experienced relapse after AED discontinuation were seizure-free after AED reintroduction. Six of the 14 patients received monotherapy and 8 patients received polytherapy. The AED dose or number was reduced in 8 patients (57.1%) and remained unchanged in two (14.3%) (Supplementary Table 1 in the online-only Data Supplement).
Predictors of seizure recurrence after AED withdrawal
A comparison of possible predictors between patients with and without seizure recurrence on AED withdrawal, based on a logistic regression analysis, is presented in Table 3. Univariate and multivariate analyses found that incomplete resection (p=0.004) and epileptic discharges on postoperative EEG (p=0.025) were significantly associated with an increased risk of seizure recurrence following attempted AED withdrawal. Older age at surgery, longer duration of epilepsy, presence of a lesion on MRI, and intracranial electrode implantation were not significantly associated with seizure recurrence after AED withdrawal. In addition, the time after surgery to AED reduction was not associated with seizure recurrence.
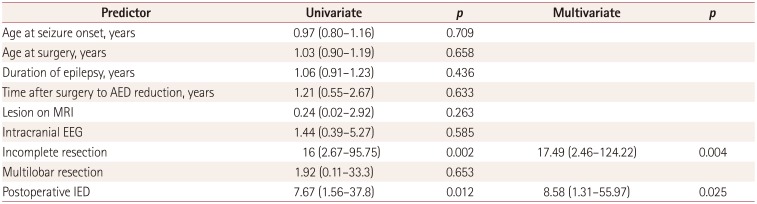
Table 3
Results from the univariate and multivariate analyses of predictors of seizure recurrence after AED withdrawal
![]()
DISCUSSION
The findings of this study suggest that approximately 35% of postoperative seizure-free children with FCD experience relapse after they start to reduce their antiepileptic medications. In several pediatric surgical cohort studies involving heterogeneous etiologies, the recurrence rate after AED withdrawal ranged from 6% to 22%.6101116 Menon et al.8 reported that FCD could be a risk factor for seizure recurrence after AED withdrawal compared with well-localized low-grade tumors and vascular malformations. The relatively higher relapse rate in our FCD cohort could have been attributable to pathological etiologies.
Postwithdrawal seizures have been widely accepted to be relatively benign and easy to control. Several adult temporallobe epilepsy studies found that >90% of patients regained seizure freedom after AED reintroduction,131617 while pediatric surgical studies demonstrated that 64–70% of the patients regained seizure freedom after AED reintroduction.61012 However, the chance of regaining seizure freedom in our cohort was lower than expected. Our results were compared with those obtained in an intractable neocortical surgical cohort, which comprised 64% adult FCD patients and found that 41.5% of the patients who experienced recurrence regained seizure freedom after AED reintroduction.7 We could not identify which factors influenced the regaining of seizure freedom after AED reintroduction due to a small number of patients with recurrence in our cohort and the retrospective study design. We assume that patients with FCD would have lower probability of achieving seizure freedom after AED reintroduction.
Older age at surgery (>30 years) or longer duration of epilepsy (>11 years) have been reported as risk factors for seizure recurrence after AED withdrawal.578 However, the age at surgery was lower and the duration of epilepsy was much shorter in our pediatric surgical cohort than in adult surgical cohorts, and so neither factor could predict seizure recurrence after AED withdrawal in our children with FCD.
Of great concern is the relationship between recurrence rate and early AED withdrawal after surgery. Findings from adult studies have suggested that early drug withdrawal increases the likelihood of seizure recurrence.57 The risk of recurrence was found to be increased in children who discontinue AEDs within 6 months after surgery.6 Our study found that the risk of recurrence was not increased when children started to taper AEDs from at least 6 months after surgery. However, we could not suggest the optimal timing for AED reduction.
Complete resection of the epileptogenic zone is the most-important predictive factor for a favorable surgical outcome in children with FCD.18192021 It is reasonable to expect that incomplete resection is associated with seizure recurrence after drug withdrawal. Surprisingly, a relationship between incomplete resection and seizure recurrence has been demonstrated only in the TimeToStop study.12 Several other authors have argued that epileptogenic regions remaining in patients with incomplete resection would increase their risk of early relapse after surgery, making them unable to withdraw from AEDs. Our study provides evidence that if the surgery does not completely remove the epileptic focus, patients may still experience seizure recurrence after drug withdrawal. Therefore, defining the entire epileptogenic region and completeness of surgical resection in children with FCD are the core factors for producing a favorable surgical outcome and successful drug withdrawal after surgery
Several studies have found the presence of postoperative interictal epileptic discharges (IED) to be associated with unfavorable seizure outcomes.8121322 Our study supports that postoperative EEG is useful for estimating the risk of recurrence before starting AED reduction in children with FCD. However, our study was subject to several limitations: the timing and duration of postoperative EEGs were not uniformly performed, and we used data from a single postoperative EEG recording session. The predictive value of seizure outcomes after AED withdrawal could be influenced by the timing and duration of EEGs, and the utilization of single versus serial EEGs.
In conclusion, approximately 35% of the present postoperatively seizure-free patients experienced seizure recurrence after AED withdrawal. The probability of regaining seizure freedom in patients with intractable FCD would be lower than expected. Children with incomplete resection and IED on postoperative EEGs have a high risk of seizure recurrence following drug withdrawal. Complete resection would lead not only to a favorable seizure outcome but would also increase the likelihood of successful AED withdrawal after surgery.
 XML Download
XML Download