

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Multiple sclerosis (MS) is a chronic, demyelinating disease of the CNS that affects approximately 2.5 million people worldwide and is the most-common cause of neurological disability in young adults.1 MS is characterized by episodes of neurological symptoms that are usually followed by neurological deficits that lead to increasing disability over 30–40 years.23 The disabilities caused by the disorder include fatigue, decreased mobility, bladder and bowel dysfunction, depression, and cognitive impairment.4 These disabilities interfere with family life, work, and recreational activities, and require the patients and their families to adjust to lifestyle changes and restrictions.1 Half of MS patients will not be able to walk without unaided within 15 years after the onset of illness, and will be unemployed within 10 years.4 About 30% of MS patients need home assistance, and in about 80% of the cases this assistance is provided by informal caregivers, usually family members who mostly comprise their spouses or partners.567
The assistance provided by informal caregivers covers a wide range of services, such as personal care, homemaking, mobility, and recreational activities.7 Caregivers play an important role in supporting patients suffering from MS at home.4 Caregivers also have to cope with the unpredictable course and prognosis of MS, including the possibility of the patient becoming severely disabled.8 Especially as the disease progresses, caregiving may become physically and emotionally more demanding and time-consuming, a combination that often leads caregivers to neglect their own needs and care,910 and also even neglect and mistreat patients.11 Some caregivers develop feelings of insufficiency and self-blame despite their commitment to the patient and adapting their lifestyle to the needs of the patient.12 Distressed caregivers might lose the ability to organize themselves and perform crucial tasks effectively.13 As Benito-León et al.14 suggested, the emphasis in MS treatment needs to shift from a patient-oriented approach to an approach that combines patients and caregivers, because caregivers are both “hidden patients” and “cotherapists”15 whose well-being is of the utmost importance for the well-being of the patients.
The aim of the present study was to measure the quality of life, fatigue, stress, and depression in caregivers of patients with MS, and to identify further possible correlations among these characteristics and characteristics of caregivers (age, gender, affinity with the patient, duration of caregiving, income, education, and hobbies) and the severity of the patient disability.
Go to : 
METHODS
Setting, study design, and subjects
One hundred and thirty-one caregivers of patients suffering from MS [age=51.2±12.8 years (mean±SD), males=53.4%, and duration of caregiving=10.0±6.3 years] and the corresponding patients themselves were prospectively enrolled in this study. Their baseline characteristics are presented in Table 1. The MS patients were recruited from the Department of Neurology, University Hospital of Ioannina, Greece from October 2015 to March 2017. The inclusion criteria for the patients were 1) having a definite diagnosis of MS, 2) being stable at the time of the study [defined as no change in the Kurtzke Expanded Disability Status Scale (EDSS) in the 3 months prior to study enrollment], 3) needing a caregiver to help them in everyday life, and 4) able to understand the aim of the study and give informed consent. The exclusion criteria for the patients were 1) acute phase or relapse of MS, 2) change in the EDSS score during the previous 3 months, 3) coexistence with another disabling disease not related to MS, 4) diagnosis of dementia according to Diagnostic and Statistical Manual of Mental Disorders-5 criteria, 5) history of alcohol or substance abuse, or 6) refusing to give informed consent.
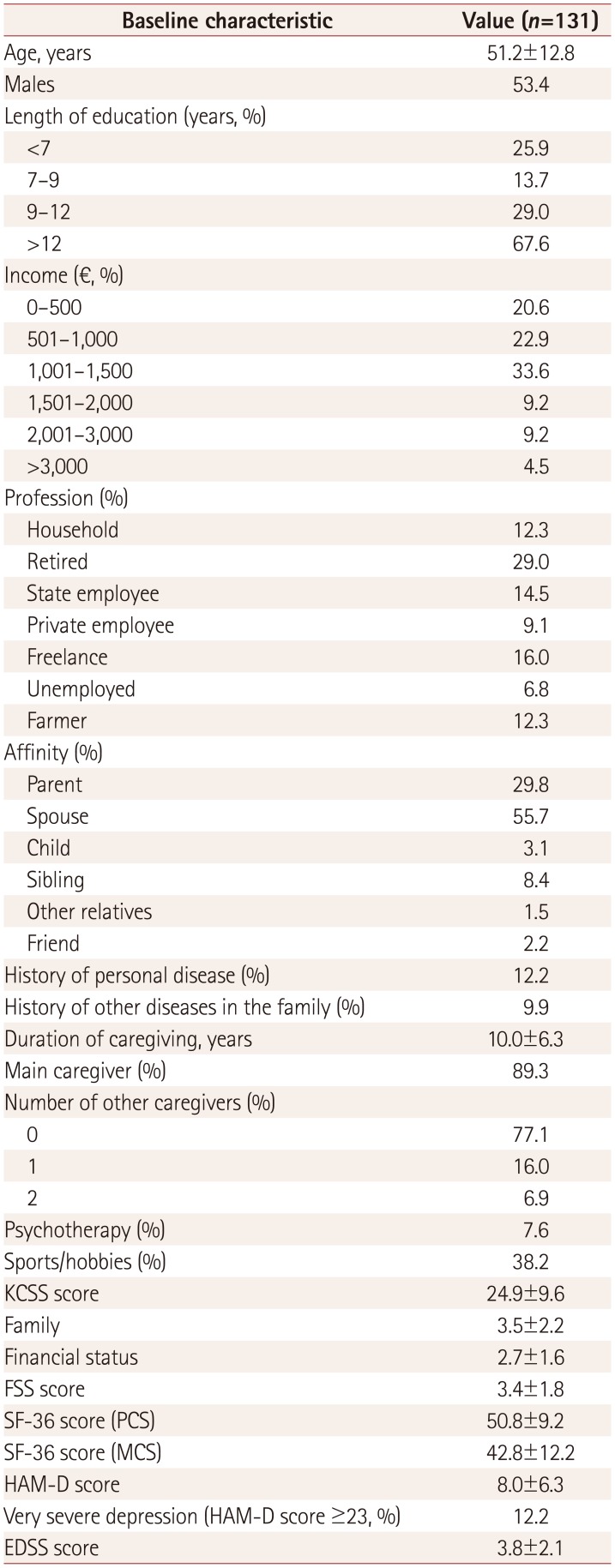
Table 1
Baseline characteristics of the caregivers
![]()
For the caregivers, defined as the persons who provided informal care on a regular basis, the inclusion criteria were 1) living with the patient and being responsible for his/her everyday care and well-being, and 2) not being paid for caregiving.
The complete study protocol was approved prior to study initiation by the ethics committee of the University Hospital of Ioannina (IRB approval number: 875-21.12.2015). Written informed consent was obtained from all patients and caregivers prior to study enrollment.
Methods
Caregiver assessments
The quality of life of the caregivers was assessed using the 36-item Short Form Health Survey (SF-36) (non-commercial license agreement, Office of Grants and Scholarly Research, OPTUM; License number: OM 029174).
The SF-36 measures physical and mental health in the following eight dimensions: vitality, physical functioning, body pain, general health perceptions, physical role functioning, emotional role functioning, social role functioning, and mental health. These eight dimensions are scaled so that the total score of the SF-36 ranges from 0 to 100, with lower scores meaning greater disability.16 The SF-36 is one of the most widely used quality-of-life instruments, and it exhibits high validity and reliability.17
Fatigue was assessed using the Krupp Fatigue Severity Scale (FSS) that includes nine items related to fatigue and its impact on everyday activities. Each item is scored from 1 to 7, and a total score of 36 or more indicates the presence of fatigue. The FSS was chosen because it possesses high sensitivity, reliability, and internal consistency in assessments of fatigue.18
Stress was assessed with the Kingston Caregiver Stress Scale (KCSS), which consists of ten questions dealing with caregiving, family, and financial status (seven, two, and one question, respectively). Each answer is scored from 1 (no stress) to 5 (extreme stress).19 KCSS is especially suitable for assessing unpaid caregivers, usually the partner or other relatives of the patient, and has satisfactory psychometric properties.20
Caregiver depression was assessed using the Hamilton Scale for Depression (HAM-D). This scale consists of 21 items, with the score being based on the first 17:8 are scored on a 5-point scale ranging from 0 (not present) to 4 (severe), and 9 are scored from 0 to 2.21 For evaluating the HAM-D scores, we adopted the severity ranges for the HAM-D reported by Zimmermann et al.22 as follows: no depression (score of 0–7), mild depression (8–16), moderate depression (17–22), and severe depression (≥23). The HAM-D has been considered a gold standard for assessing the severity of depression in both clinical settings and research.23
Patient assessments
The EDSS was applied by an experienced neurologist to rate the disability status of each patient.27
Statistical analysis
We first used linear regression models to identify correlations of the KCSS and its three domains (caregiving, family, and financial status) with both the HAM-D and the two domains of the SF-36 [physical component summary (PCS) and mental component summary (MCS)]. Additional linear regression analyses were performed to investigate the association of both the PCS and MCS of the SF-36 with the FSS and HAM-D. We then used univariable and multivariable logistic regression analyses to investigate possible associations of all baseline ordinal characteristics of the caregivers and the severity of patient disability (quantified by the EDSS score) with the caregiver fatigue status, as expressed by the numerical values on the corresponding scale. All baseline characteristics that contributed to the outcome of interest in the initial univariable analyses at p values <0.1 were included in the multivariable model as candidate variables. The final variables that were independently associated in the multivariable logistic regression analyses with the outcome of interest were selected by a backward stepwise selection procedure using a p value of <0.05. Finally, the association of caregiver fatigue with baseline non-ordinal characteristics regarding the caregiver profession and their affinity with the patient was assessed using a one-way ANOVA.
All statistical analyses were performed using the stata statistical software (release 13 for Windows, StataCorp., College Station, TX, USA).
Go to :
RESULTS
Caregivers had scores on the FSS, KCSS, and HAM-D of 3.4±1.8, 24.9±9.6, and 8.0±6.3, respectively, with severe depression (HAM-D score ≥23) reported in 12.2%. Their SF-36 scores for the PCS and MCS were 50.8±9.2 and 42.8±12.2, respectively.
In linear regression analyses (Table 2 and 3), caregiver fatigue was found to be positively associated with stress, as assessed using the KCSS (r=0.38, 95% CI=0.30 to 0.46, p<0.001), and negatively correlated with both physical health status (r=−1.11, 95% CI=−1.35 to −0.88, p<0.001) and mental health status (r=−0.75, 95% CI=−0.94 to −0.56, p<0.001). Similarly, caregiver stress (as assessed using the KCSS) was found to be positively associated with depression (r=0.99, 95% CI=0.79 to 1.19, p<0.001) and negatively correlated with both the physical health status (r=−0.51, 95% CI=−0.67 to −0.35, p<0.001) (Fig. 1A) and mental health status (r=−0.49, 95% CI=−0.59 to −0.38, p<0.001; Fig. 1B). Finally, depression (as assessed with the HAM-D) was negatively correlated with both the PCS (r=−0.30, 95% CI=−0.41 to −0.19, p<0.001) and MCS (r=−0.33, 95% CI=−0.40 to −0.26, p<0.001) of the SF-36.

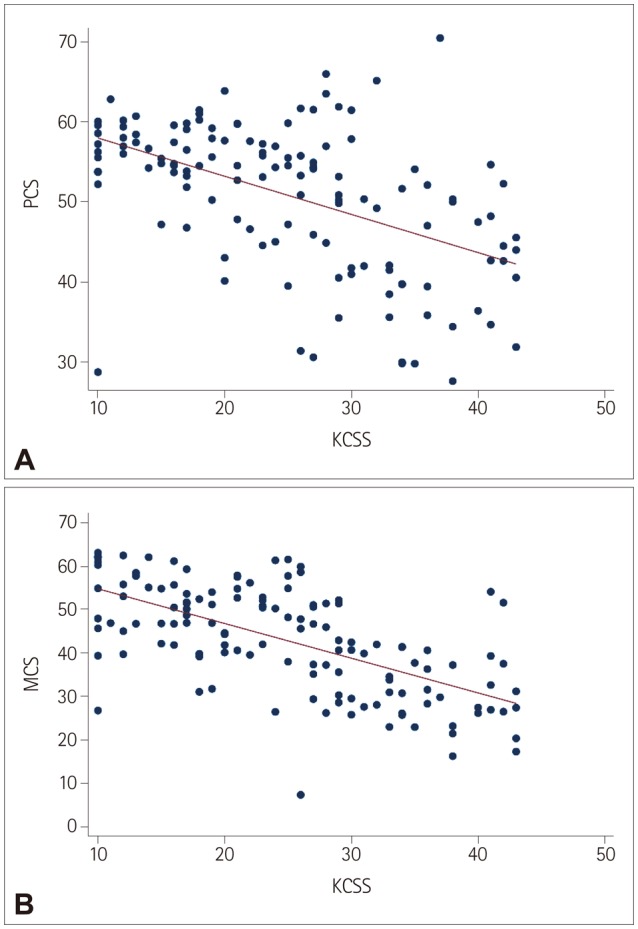 | Fig. 1Association of stress with the physical health status (A) and mental health status (B) of caregivers of patients with multiple sclerosis. Stress was assessed using the KCSS, while physical health status and mental health status were assessed with the PCS and MCS, respectively, of the 36-item Short Form Health Survey. KCSS: Kingston Caregiver Stress Scale, MCS: mental component summary, PCS: physical component summary.
|
Table 2
Associations of the KCSS with the FSS, HAM-D, and SF-36
![]()

In the univariable analysis of the associations of nonordinal baseline characteristics (Table 4), caregiver profession was significantly associated with fatigue (p=0.038), with unemployed caregivers reporting fatigue symptoms more often than the other categories. Similarly, the reported fatigue level varied significantly according to the affinity of the caregiver with the patient (p=0.027). In the univariable logistic regression analysis (Table 5), caregiver age (p=0.001), education (p=0.002), sports (p=0.006), history of chronic disease (p=0.002), other chronic disease in the family (p=0.012), and the disability status of the patient (p=0.023) were significantly associated with caregiver fatigue. In multivariable logistic regression analyses (Table 5), caregiver fatigue was independently associated with education status (OR=0.61, 95% CI=0.37 to 0.99, p=0.046), history of chronic disease (OR=5.52, 95% CI=1.48 to 20.55, p=0.011), other chronic disease in the family (OR=7.48, 95% CI=1.49 to 37.47, p=0.014) and disability status of the patient (OR=1.36, 95% CI=1.03 to 1.80, p=0.032).

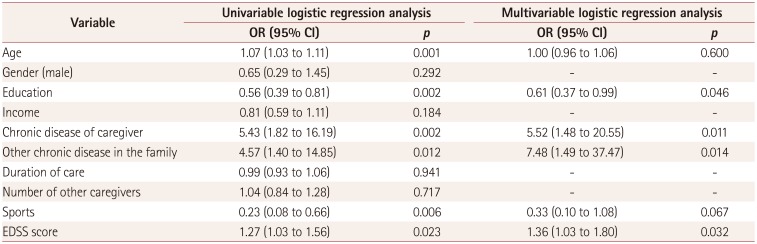
Table 4
Results from the univariable analysis of the association of baseline nonordinal characteristics with fatigue
![]()
Table 5
Results from the univariable and multivariable logistic regression analyses ofthe association of baseline ordinal characteristics with fatigue
![]()
Go to :
DISCUSSION
This study found that caregivers experienced high levels of stress, as indicated by a KCSS score of 24.9±9.6, and a reduced quality of life, as indicated by PCS and MCS scores on the SF-36 of 50.8±9.2 and 42.8±12.2, respectively. We also found high rates of clinical depression in caregivers, with very severe depression (HAM-D score ≥23) reported in 12.2% (n=16), severe depression in 3.8% (n=5), and moderate depression in 9.2% (n=12) of the caregivers. Depression was negatively correlated with both physical health status and mental health status, and positively correlated with fatigue and caregiver stress. Labiano-Fontcuberta et al.28 reported depressive symptoms in 25% of a sample of 63 caregivers of MS patients, with 19% and 1% having moderate and severe depression, respectively. The caregivers with more depressive symptoms were mainly females and had greater comorbidity (additional diseases).
Caregiver fatigue was associated with their education status, history of chronic disease, history of other chronic disease in the family, their affinity with the patient, and the disability status of the patient. It was particularly notable that unemployed caregivers reported fatigue symptoms more often than the other categories. Employment seems to contribute to the well-being of caregivers. As other studies have suggested, well-being is associated with the ability of individuals to find life goals and a meaning-making system in their lives. The importance individuals give to life domains such as family, work, social relationships, and hobbies is crucial in determining how a domain contributes to their life well-being. Professional life functions as a protective factor against fatigue among caregivers, and age, gender, and personality characteristics may also play roles.29 The present study found that caregiver fatigue was not associated with gender or age. Males constituted 53.4% of our caregiver sample. That is in accordance with other studies, because MS is more prevalent in women and so men are more likely to be the spousal caregivers. According to Lee et al.,30 women caregivers tend to experience higher levels of strain, higher needs for emotional support, and higher perceived social support. However, no statistically significant difference was observed between the male and female caregivers in our sample.
Caregiver stress was correlated with physical disability of the patients (as measured by the EDSS), which is in accordance with previous reports of this factor being a strong indicator of caregiver stress.831 Katsavos et al.32 reported that caregiver stress was positively correlated with age, EDSS score, and disease duration, and negatively with cognitive, physical, and mental health. Depression in MS patients seems to be strongly correlated with depressive symptoms in caregivers, resulting in a less-satisfying relationship, reducing the motivation and investment of the caregiver in his/her role.8 The present study found that the severity of illness and the history of other chronic disease in the family were significantly correlated with caregiver strain, although illness duration did not to influence caregiver strain. This could have been due to caregivers tending to get used to the diagnosis of MS but not to its severe consequences. Income does not seem to play a role in caregiver strain, although low income imposes restrictions on leisure activities, while education and employment does. Caregivers with higher education and who are employed experience less strain, perhaps because employment gives them the opportunity to change their roles and obligations as well as to have social relationships unrelated to the MS patient.
Despite the strengths of our study associated with its prospective design and the consecutive enrollment of both patients and caregivers, some limitations should also be acknowledged. First, since our sample was small and representative of an urban population in northwestern Greece, the obtained results might not be applicable to other populations. Second, the patient sample consisted of an ambulatory outpatient MS population and thus the more severely affected patients who require extensive or permanent nursing-home care were underrepresented. Finally, it should be noted that our patient group did not undergo an extensive neuropsychological assessment, and so we cannot draw any conclusions about a possible correlation between cognitive deficits of the patients and caregiver stress.
In conclusion, this study found that caregiver strain was positively correlated with the severity of illness, history of other chronic disease in the caregiver or another family member, their affinity with the patient, and the education of the caregiver. Illness duration, income, and caregiver hobbies do not seem to influence caregiver strain. We also found that high rates of depression in caregivers were positively correlated with caregiver stress and negatively with physical health status and mental health status as expressed in SF-36 scores. Future studies need to further elucidate the great impact that the psychological condition of caregivers has on the quality of life of MS patients.
Go to :
 XML Download
XML Download