

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Human memory does not constitute a unified system, and so should be assessed as a set of distinct subsystems. Explicit memory (also called declarative memory) is a type of long-term memory that can be further subdivided into episodic memory and semantic memory.1 The main functions of episodic memory are the storage and retrieval of specific episodes and events occurring in the life of an individual. In contrast, semantic memory is a more systematized record of facts and knowledge that an individual has acquired about the world.23 There is a wide clinical consensus that the loss of episodic memory is the most-representative symptom of Alzheimer's disease, and deficits in semantic memory have attracted less attention from researchers even though it is also commonly encountered in clinical practice. Another important difference between episodic memory and semantic memory is that whereas episodic memory impairment is frequently observed in healthy elderly patients, semantic memory remains relatively stable across the adult lifespan. This means that semantic memory is potentially useful as a marker for distinguishing pathological aging from normal senescence. However, recognizing semantic memory decline in the early stage of Alzheimer's disease remains difficult. Therefore, in order to detect subtle impairment of semantic memory, both its quantitative and qualitative aspects need to be thoroughly evaluated.
Unlike prior research on healthy elderly patients, or those with Alzheimer's dementia (AD), previous studies of semantic memory in patients with mild cognitive impairment (MCI) have produced controversial results.4567 Important causes of this inconsistency include the application of diverse analysis methods and the various criteria used for patient selection and classification. In this context, it is essential to characterize the target group based on both neuropathology concepts and clinical criteria.
In order to obtain a deeper understanding of the prodromal stage evolving into AD, the present study focused on the amnestic MCI (aMCI) stage stratified by the β-amyloid (Aβ) status, which is known to be the pathological hallmark of Alzheimer's disease. We hypothesized that, despite similar clinical severities, qualitative aspects of semantic memory impairment differ between Aβ+ and Aβ− aMCI patients. We further hypothesized that a disease continuum corroborated by the pattern of semantic memory dysfunction exist from Aβ+ aMCI to AD.
METHODS
Participants
This study enrolled 314 participants selected among the patients who visited the memory clinic of Asan Medical Center, Seoul, Korea from February 2015 to August 2016. All participants or their proxies signed informed-consent forms. All participants underwent 3-tesla brain MRI, detailed neuropsychological testing, and fluorine-18 [18F]-florbetaben amyloid PET. [18F]-florbetaben amyloid PET was performed at 90 to 110 min after the intravenous injection of 300 MBq florbetaben. Two neurologists (J.L. and J.H.R.) and two nuclear medicine physicians (J.S.K. and M.Oh.) reviewed PET scans according to the predefined regional cortical tracer binding (RCTB) and the brain amyloid plaque load (BAPL) scoring system. The final score was reached by consensus, with a BAPL of 1 regarded as Aβ− and BAPL of 2 and 3 considered to be Aβ+. The cognitive status of each participant was judged based on history-taking and neuropsychological results.
All of the participants underwent blood tests including a complete blood count, chemistry battery, vitamin B12, folate, syphilis, and HIV serology, as well as thyroid function tests to rule out medical conditions causing cognitive decline. The ApoE genotype was identified after extracting genomic DNA from the venous blood. To rule out the probability of mixed dementia, the participants whose MRI results showing cerebral white matter hyperintensities on T2-weighted/FLAIR sequences (Fazekas scales 2 or 3)8 were excluded from the data set. The Institutional Review Board of Asan Medical Center approved the study protocol (2014-0783).
MCI group
The patients with MCI were defined according to the criteria proposed by Petersen et al.9 The aMCI subtype was determined when the scores were below the 16th percentile (-1 SD) for demographically matched norms in verbal or visual memory tasks. We included all patients with single- or multiple-domain aMCI with no evidence of impairment when performing the activities of daily living. The aMCI patients were further subdivided into two groups according to the Aβ status based on PET scans.
Control group
Along with aMCI as a target group, we set up two control groups: normal controls and disease controls. A diagnosis of cognitively normal (CN) was made when scores in all subdomains of detailed neuropsychological tests exceeded -1 SD of the age- and education-level-adjusted mean score. Only cases with Aβ− CN verified by an [18F]-florbetaben amyloid PET scan were included in the normal control group. Similarly, we included only Aβ+ clinically probable AD10 in the disease control group.
Neuropsychological assessments
General cognition and subdomain scores
All participants were assessed using the Seoul Neuropsychological Screening Battery (SNSB) as a formal test. The SNSB is a comprehensive neuropsychological battery that includes various tests measuring attention (forward/backward digit span), language (comprehension, repetition, confrontational naming, reading, and writing), calculation, praxis (buccofacial and ideomotor), visuospatial function [Rey Complex Figure Test (RCFT)], verbal memory (Seoul Verbal Learning Test immediate recall, delayed recall, and recognition), visual memory (RCFT immediate recall, delayed recall, and recognition), and frontal/executive function (contrasting program, go/no-go test, verbal fluency, and the Stroop test). The Korean version of the Mini Mental State Examination (K-MMSE), Global Deterioration Scale (GDS), Clinical Dementia Rating (CDR), Korean Dementia Screening Questionnaire (K-DSQ), Neuropsychiatric Inventory (NPI), and Geriatric Depression Scale (GDepS) were also used. The subdomain scores for 14 items conforming to a normal distribution are presented as z scores.
Qualitative assessments of semantic memory
In view of the essential role played by language function in the process of codification and storage, we focused on lexical semantic memory. While several methods measuring lexical semantic memory are available, confrontation naming tasks11 and verbal fluency tasks1213 can be easily conducted in clinical settings. Therefore, to enhance feasibility, we conducted qualitative assessments using the 60-item Korean version of the Boston Naming Test (K-BNT) and the Controlled Oral Word Association Test (COWAT), which form part of the SNSB. Participants with advanced AD who failed to complete both the K-BNT and COWAT were excluded from the data set.
K-BNT for testing confrontational naming ability
Participants were asked to name the object after presenting each of 60 picture cards. If a participant answered incorrectly or did not respond after 15 seconds, a semantic cue was provided. If the participant still failed to answer after giving the semantic cue, the first syllabic cue and the second syllabic cue were given in sequence. Incorrect responses recorded during the task were reviewed and classified into the following six error types14:
1) Visuoperceptual errors, in which the responses are visually similar but belong to different semantic categories (e.g., ‘umbrella’ for ‘cobweb’).
2) Semantically related errors, of which three subcategories can be differentiated: superordinate (i.e., the response is visually similar to the item and belong to category with a moregeneral concept), coordinate (i.e., the response is visually similar to the item and belong to the same category), and circumlocutory (i.e., the responses are about proper function or relevant statements of the item).
3) Semantically unrelated errors, which include irrelevant statements about the item, simple descriptions, or are based on the own experiences of the participants.
4) Phonemic errors, which are mispronunciations of the target name, including omissions, substitutions, paraphasia, and neologism.
5) Responded that they did not know the answer.
6) Did not respond.
We quantified the proportion of errors as the number of errors in each category expressed as a percentage of the total number of errors on the K-BNT.
Thereafter we estimated the cueing effect after semantic cues and syllabic cues. In the Korean language, the concept of a phonemic cue should be regarded as a syllabic cue because, unlike English words, Korean words are composed of syllables rather than phonemes.15 The cueing effect was calculated as the increase in the number of correct answers after cueing divided by the total number of each cue for the semantic cue, the first syllabic cue, and the second syllabic cue.
COWAT for testing generative naming ability
We compared the total number of words excluding errors and repetitions generated during 1 minute for each task. We then analyzed the functions of clustering and switching, which are two main components of verbal fluency tasks introduced by Troyer et al.16 In the present context, clustering refers to the production of words within semantic or phonemic subcategories. For example, in the semantic fluency task for animal names, clusters were defined as groups of successively generated words belonging to the same subcategory, such as pet, livestock, fish, bird, and insect names.17 Here the concept of 12 animals of the Chinese zodiac should be considered, since Koreans have their own Chinese zodiac sign for their year of birth. The names of these zodiac signs include various domestic animals (e.g., pig, dog, sheep, and horse) and wild animals (e.g., tiger, rabbit, monkey, and reptiles such as snake). Therefore, if more than four animal names belonging to the zodiac category were reported successively, they were counted as one cluster.18 More than two words were deemed to create a cluster, and so if a certain subcategory consisted of one word, we excluded it from the cluster count.
Also in the present context, switching represents the ability to shift between clusters, and this was counted as the number of transitions between clusters, including all single words. Cluster size was counted beginning with the second word in each cluster (e.g., a cluster of two words was assigned the size score of 1, while a cluster of four words had a size score of 3). The mean cluster size was calculated by summating all cluster sizes and dividing by the total number of clusters.19
We measured the total number of generated words, number of switches (NS), number of clusters (NC), and mean cluster size (MCS) for each fluency task. In accordance with previous suggestions that different brain regions mediate the generation of living items and nonliving items,202122 semantic fluency tasks for animal names and supermarket items were analyzed separately. The results for the phonemic fluency task were analyzed after summing and then averaging the results for three phonemes.
Measurement of interrater reliability
To measure interrater reliability, 20% of the samples from each group were randomly extracted using the Microsoft Excel program. Another neurologist (S.H.P.) rated qualitative variables of the K-BNT and COWAT according to the same references. Two raters (J.E.K. and S.H.P.) showed strong agreement for each error type (all >95%) with the exceptions of ‘don't know’ responses and no responses (80% and 75%, respectively) due to equivocal differentiation. We therefore modified error-type classification by combining ‘don't know’ responses and no responses into a single nonresponses category. For continuous variables including accuracy rates after each cue, NS, NC, and MCS, we estimated the intraclass correlation coefficient (ICC) using a two-way random model. The range of ICC values (0.772–0.891) demonstrated the high reliability for all variables.
Statistical analyses
The statistical analyses were performed using SPSS (version 21.0, IBM Corp., Armonk, NY, USA). In the first step, to figure out the pattern distribution of the data, we conducted Kolmogorov-Smirnov tests. Furthermore, one-way ANOVA and paired t-test for the data showing normal distribution were run. Analysis of covariance was also used when there was a need of the age-adjusted comparison between the groups. For data that did not conform to a normal distribution, the Kruskal-Wallis test was used for continuous variables and the chi-square test was used for ordinal scales.
Categorical variables were represented as proportions, while continuous variables were represented as mean±SD. The criterion for statistical significance was set at p<0.05; however, in case of multiple comparisons, the post-hoc p value was adjusted using the Bonferroni correction method: p<0.05/(number of tests). Although our main focus was comparing Aβ+ aMCI and Aβ− aMCI, we also investigated whether there was any trend across the groups for each of the variables.
RESULTS
Demographic and clinical characteristics
Among 314 subjects who participated in all of the tests, the 56 nonamnestic MCI patients were excluded based on the results of detailed neuropsychological testing. In addition, the participants finally diagnosed as Aβ+ CN (n=3), Aβ− clinically probable AD (n=9), or dementia of other neurodegenerative etiology (n=29) were also excluded from the control group. Thus, a total of 217 participants (Aβ− CN, n=53; Aβ− aMCI, n=66; Aβ+ aMCI, n=56; Aβ+ AD, n=42) were included in the final analysis.
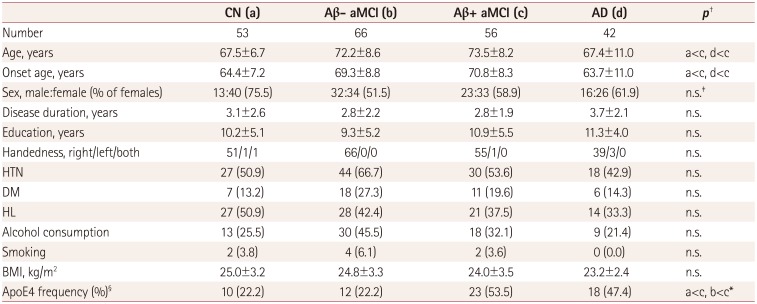
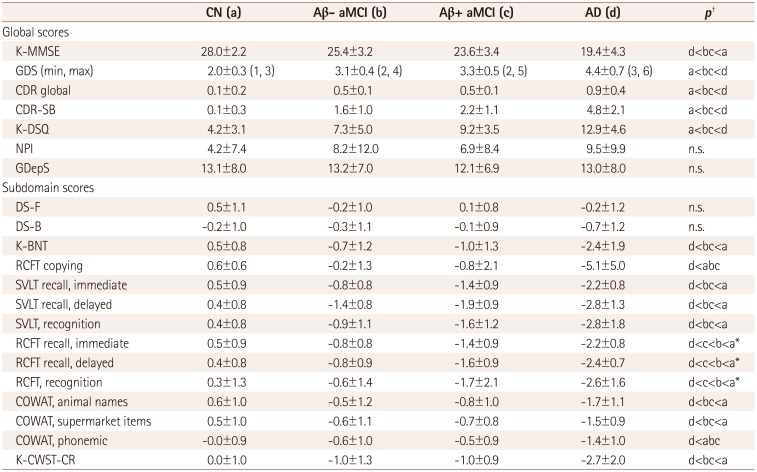
The detailed demographic and clinical characteristics of the participants are presented in Table 1. The patients with Aβ+ aMCI were older than the participants in the control groups, but did not differ from Aβ− aMCI patients. Of note, the frequency of the ApoE4 allele was significantly higher in the Aβ+ aMCI group (53.5%) than in the Aβ− aMCI group (22.2%, p=0.002), but similar to the frequency in AD (47.4%, p=0.585). Other demographic factors including the sex distribution, disease duration, education level, handedness, vascular risk factors, and body mass index did not show significant differences between the two aMCI groups.
Neuropsychological assessments
General cognition and subdomain scores
Detailed neuropsychological profiles for the global scales and subdomain scores are presented in Table 2. The scores on global scales including the K-MMSE, GDS, CDR global, CDR sum of boxes, GDepS, K-DSQ, and NPI did not differ significantly between the two aMCI groups. The impairment of the visual memory function was greater in the Aβ+ aMCI group than in the Aβ− aMCI group, but no differences in attention, visuospatial function, verbal memory, or frontal/executive function were observed. Of note, the quantitative measurements based on z scores of the K-BNT and COWAT also did not differ between Aβ+ aMCI and Aβ− aMCI.
Qualitative assessments of semantic memory
K-BNT for testing confrontational naming ability
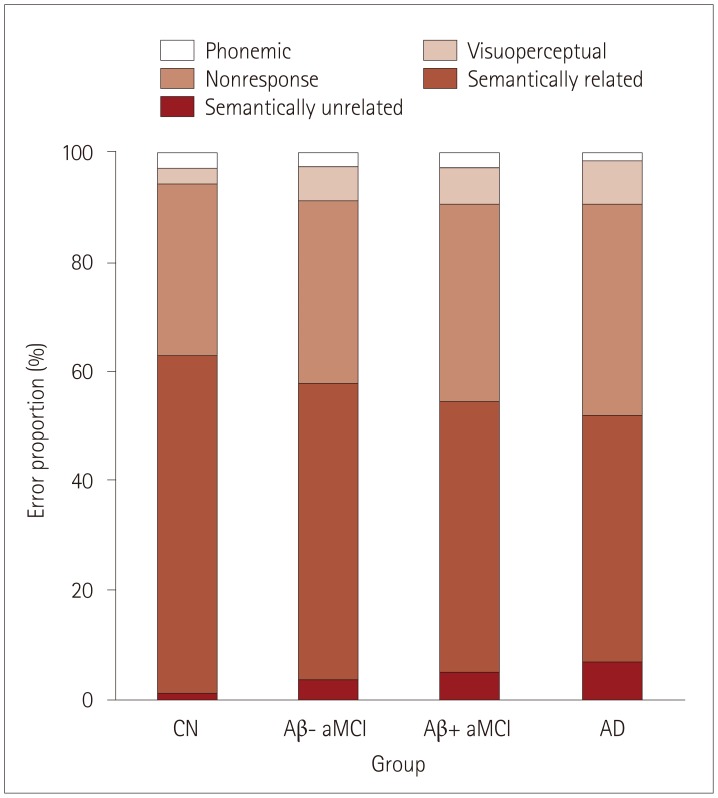
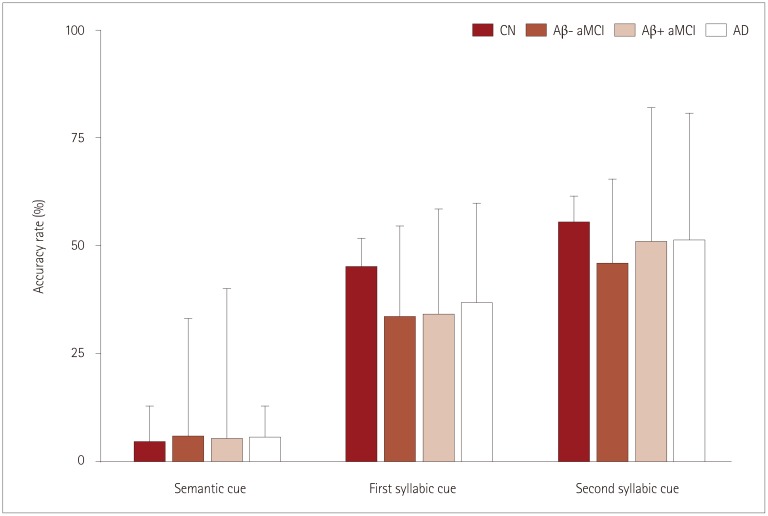
In terms of error proportion, semantically related errors were the most common among the five subtypes throughout the group. Although the differences between the two aMCI groups did not reach statistical significance (semantically related error, p=0.895; semantically unrelated error, p=0.747), a decreasing or increasing tendency was noted. Intriguingly, semantically related errors showed a decreasing proportion in the order of CN, Aβ− aMCI, Aβ+ aMCI, and AD, while semantically unrelated errors showed an inverse pattern (Table 3, Fig. 1). Specifically, Aβ+ aMCI and AD demonstrated a significantly higher proportion as compared to CN, while Aβ− aMCI did not. These findings suggest that there is a subtle semantic memory disruption even in the Aβ+ aMCI group, namely at the prodromal AD stage. Cueing effects for semantic and syllabic cues were not significantly different between the two aMCI groups (semantic cue, p=0.937; first syllabic cue, p=0.998; second syllabic cue, p=0.799). Across all groups, the accuracy rate was the lowest after semantic cue and the highest after second syllabic cue (Fig. 2).
COWAT for testing generative naming ability
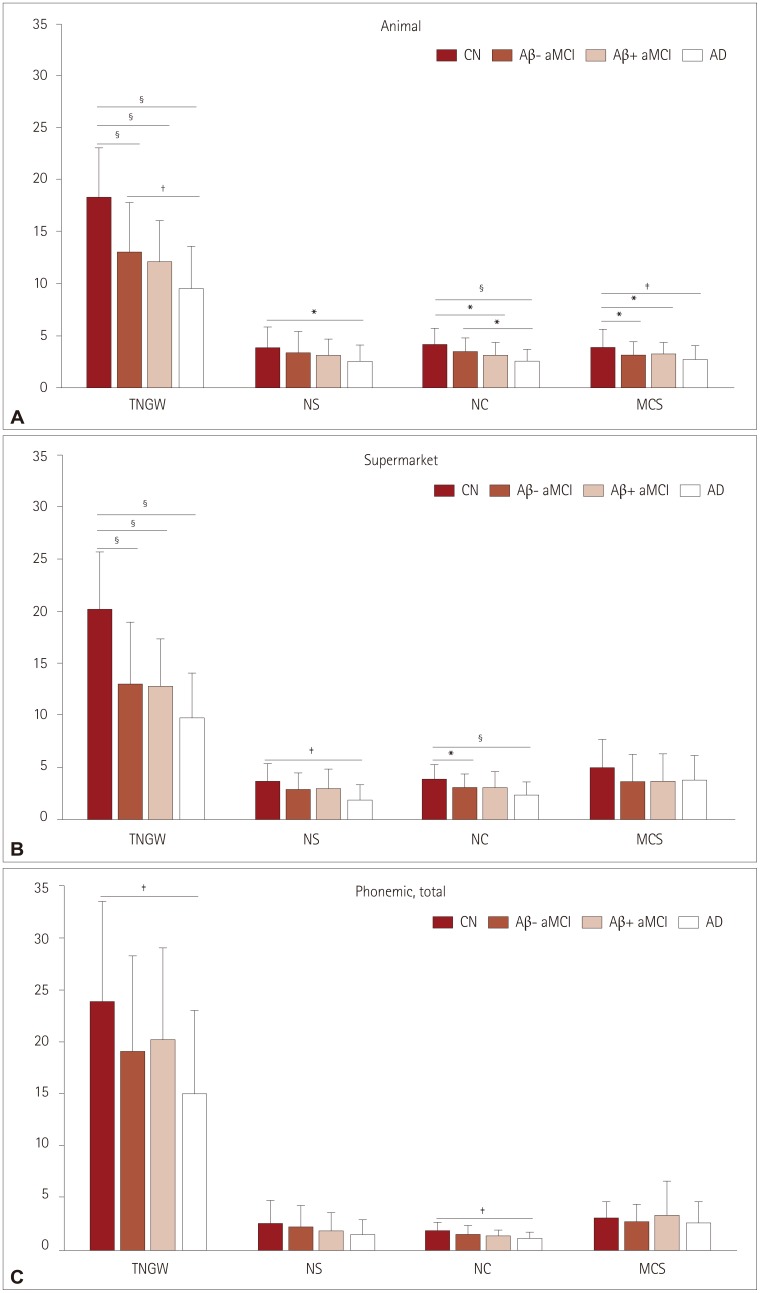
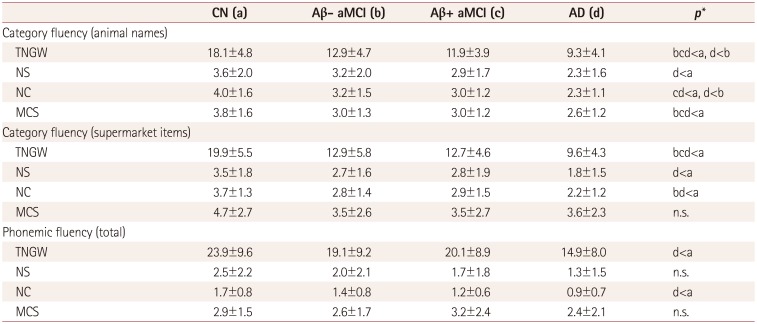
No statistical differences between Aβ− aMCI and Aβ+ aMCI for all variables including NS, NC, and MCS in both category fluency and phonemic fluency tasks were found. However, we found a decreasing tendency in NS, NC, and MCS in the order of CN, Aβ− aMCI, Aβ+ aMCI, and AD in the animal naming task. Compared to the animal (living items) naming task, this trend was more blurred in the supermarket items (nonliving items) task and the phonemic fluency task. It should be noted that there was no significant difference between Aβ+ aMCI and AD (p=0.112), while Aβ− aMCI showed better performance than AD (p=0.006) in terms of NC in the animal naming task (Table 4, Fig. 3).
DISCUSSION
This study compared the neuropsychological performance in terms of semantic memory disruption between aMCI groups stratified based on the brain Aβ status. The Aβ+ aMCI group was more similar to AD in the pattern of qualitative measurements of confrontational naming and verbal fluency. In addition, there was a continuum of semantic memory dysfunction across the CN, aMCI, and AD groups. Semantic memory impairment has known to be common in Alzheimer's diseases,122324 even though it is neither the first nor the most-sensitive symptom. Patients with Alzheimer's disease frequently show progressive impairment in tasks requiring semantic memory function, such as object naming and word finding.112526 Specifically, AD patients demonstrate worse performance in the category fluency task than in the phonemic fluency task, indicating the presence of semantic memory disruption.
There are two primary hypotheses about the semantic deficits found in AD: the first hypothesis emphasizes the loss of semantic information or representation itself, while the second hypothesis claims that semantic deficits are caused by disruption in accessing or retrieving information stored in long-term semantic memory.27 The semantic memory dysfunction in Alzheimer's disease is characteristic not only of the stage of apparent dementia, with several studies having already documented semantic memory impairment even in MCI patients.7122829 Although there are some controversies about neural substrates in the MCI stage in terms of semantic memory, there is a growing understanding that it is not limbic structures, but widespread cortical regions that are implicated in the semantic system.303132 Therefore, considering the hierarchical progression of neuropathology in Alzheimer's disease,33 semantic memory impairment can be probably subtle or subclinical at the early stage of disease.
Several studies have attempted to characterize the nature of semantic memory impairment in aMCI, which is considered the prodromal AD stage.343536 However, due to the high variability in the methodological approaches, there is no consensus about the nature of semantic memory in aMCI. For instance, whereas, in the present study we focused on lexical semantic memory, there are many other aspects of semantic memory and ways of assessment. Above all, a well-characterized target group is a prerequisite of the study aimed at the prodromal AD stage. Owing to the lack of neuropathological markers, identifying aMCI based solely on clinical diagnostic criteria can yield mixed results for aMCI due to AD or non-AD. Clinical features and disease severity of Aβ+ aMCI can be very similar to Aβ− aMCI, although they are not identical phenocopies. However, a better differentiation of them in clinical settings is hardly attainable without relevant information about neuropathological markers. Hence, in the present study, we dichotomized the patients with aMCI based on their brain Aβ status using visual assessments of [18F]-florbetaben amyloid PET scans. Normal control and disease control groups were also defined based on combinations of the Aβ status and clinical criteria. This approach enabled us to further the understanding of semantic memory deficits in Aβ+ aMCI as a transitional stage evolving into AD. However, we did not intend to investigate the correlation between semantic memory impairment and the Aβ burden or distribution. It has been shown that the functional decline is correlated with neurofibrillary tangle pathology rather than being directly correlated with Aβ pathology.3738 Therefore, acquiring additional information about the distribution and sequential order of two hallmarks of AD pathology will allow the correlations with semantic memory deficits and structural change to be addressed.
Error patterns on the K-BNT task showed fewer semantically-related errors and more semantically-unrelated errors in the Aβ+ aMCI group as compared to the Aβ− aMCI group without a gross difference in confrontational naming ability. Previous studies have found that patients with Alzheimer's disease exhibit high rates of semantic errors when performing the confrontational naming task, with these errors being a consequence of semantic memory disruption.394041 It is widely known that the process of naming objects consists of several steps that occur sequentially42: recognition of a visual stimulus, semantic processing, selection of an abstract representation (lexical access), and naming the stimulus. The qualitative error types presented in the K-BNT can result from individual or combined disruptions at different stages. Among those, semantic errors may indicate a disruption in the process where integrated information triggers semantic knowledge. Therefore, our results are indicative of the difficulties involved in this process in aMCI, and more specifically in Aβ+ aMCI. As the disease progresses, the proportions of each error types may change due to the overall dysfunction of the naming process. Therefore, characterizing longitudinal patterns of the error distribution in neuropathologically identified Alzheimer's spectrum disorder will be helpful for better understanding the disease continuum. In addition, verifying subclinical semantic disruption as an early marker of brain Aβ pathology, it may be beneficial to compare the proportion of converter to AD in Aβ+ aMCI showing prominent semantic errors with Aβ− aMCI.
Regarding cueing effects, our findings suggest that some degree of semantic knowledge was preserved in Aβ+ aMCI, thereby causing minimal response to semantic cueing. Given that we excluded patients with advanced AD who failed to complete the full K-BNT from the final analysis, semantic memory disruption in the AD group might also not have been especially severe. We found that the patients with both aMCI and AD needed assistance when retrieving the phonological information about a given object. Although the accuracy rates did not differ significantly between the CN group and the patients with aMCI or AD, the efficacy after each cue was highest for the CN group. If patients with more-severe AD had been included in the disease control group, the difference between prodromal and apparent AD would be more evident in terms of cueing effect.
Verbal fluency tests are the most widely used measurements to investigate the function of associative exploration and retrieval of words with a time constraint based on semantic or phonemic criteria. While phonemic fluency requires searching strategies based on the lexical representation, semantic fluency requires the ability to apply semantic extensions of a target category, which is based on the integrity of semantic associations. Therefore, impaired semantic fluency may reflect semantic memory disruption rather than phonemic fluency;2543 for example, a meta-analytic review investigated the relative magnitudes of cognitive deficits in semantic and phonemic fluency tests in patients with focal cortical lesions.44 The results of this study strongly suggest that while two types of fluency task demonstrated comparable demands on executive functioning, semantic fluency task was more dependent on the integrity of semantic memory.
Regarding neural substrates, previous studies have reported that semantic fluency is more related to temporal lobe dysfunction, while phonemic fluency is more sensitive to frontal dysfunction.4546 In a similar context, numerous studies have reported disproportionately impaired semantic fluency relative to phonemic fluency in the patients with Alzheimer's disease.134748 Along with discrepancies in terms of the task type, qualitative measurements including switching and clustering also reflect different semantic function.49 Clustering is related to the ability to search words within certain subcategories, and it depends on temporal-lobe processing. In contrast, switching involves shifting from one subcategory to a new one, and it depends on frontal-lobe processing comprising strategic searching and cognitive flexibility.1650 Impaired clustering and switching abilities have also consistently been found to affect category fluency in patients with AD,505152 and also (to a lesser degree) phonemic fluency.50
The question about the dissociation of naming abilities between living and non-living categories has emerged since the report of four patients who suffered from herpes simplex encephalitis.27 Dissociation between the knowledge of living and nonliving things in Alzheimer's disease has also been reported, suggesting more impaired performance for living items5354 and a significantly faster declining rate than non-living items.21 Furthermore, many lesion studies investigating neural substrates of conceptual organization have found the left anterior temporal cortex to be related to the ability to process living items,5556 while the left posterolateral temporo-parietal cortex has been found to be related to nonliving items.57 In our results, compared to the Aβ− aMCI group, the Aβ+ aMCI patients showed a more prominent deficit in the number of clustering on the semantic fluency task, especially for animal (living item) naming. All these findings suggest that semantic network deficits with decreased strategy usage may have a negative impact on performance. Additionally, a probable dysfunction of dominant temporal lobe is suggested when comparing the features of semantic memory deficits in Aβ+ aMCI with those of Aβ− aMCI.
The present study has several limitations. First, it is a cross-sectional study without evidence for longitudinal changes in the disease continuum. Therefore, we may be able to get more information on the trajectory of the semantic memory system with the follow-up data of neuropsychological tests and neuroimaging. Second, despite its strength of feasibility, lexical memory is not representative of the entire semantic system. Third, some patients with a profound cognitive decline were excluded from the further analysis due to the lack of analyzable neuropsychological data. As a result, a higher proportion of mild AD was included, which could have attenuated representativeness of the disease control group. However, despite aforementioned limitations, the strength of the present study is that we classified all groups using clinical diagnostic criteria combined with the Aβ pathology status, which enabled us to get a deeper understanding of prodromal AD. In addition, we approached semantic memory, an understudied domain in the clinical practice, in a comprehensive and systematic manner.
In future research, studying the distribution of tau aggregation in patients with proven brain Aβ deposits would be informative in terms of investigating the correlations between AD pathology and functional or structural changes in the semantic memory network. Furthermore, considering that semantic memory deficits are subtle in the early stage of Alzheimer's disease, an additional stratification of the aMCI group into early versus late aMCI may be helpful to identify the nature of the disease continuum.
In summary, despite similar disease severities and clinical manifestations, Aβ+ aMCI may differ from Aβ− aMCI in terms of semantic memory. Along with episodic memory, semantic memory may serve as an early indicator of brain Aβ pathology. Therefore, the semantic memory dysfunction deserves more attention in the clinical practice.

 XML Download
XML Download