

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Transthyretin familial amyloid polyneuropathy (TTR-FAP) is a rare inherited amyloidosis disorder associated with mutation in the TTR gene that affects more than 38,000 patients worldwide and manifests as a progressive sensorimotor and autonomic polyneuropathy.123 The gene mutations lead to destabilization of the tetrameric structure of the TTR protein, such as dissociation, misfolding, and aggregation. The TTR protein usually acts as an amyloid target to the peripheral nerve tissue, and axonal degeneration initiating from small myelinated and unmyelinated nerve fibers to larger myelinated fibers, causing sensory syndromes including pain and temperature sensation in the lower extremities, motor impairment, muscle weakness, progressive and autonomic gastrointestinal, urogenital, and cardiovascular dysfunctions, or even death within a decade from onset.45
TTR is a plasma protein consisting of 127-amino-acid monomers, which is mainly secreted by the liver and functions as a backup transporter for thyroxine and a primary transporter for the retinol-binding protein/vitamin A complex.6 The TTR gene is located on chromosome 18q12.1 in human. More than 120 described point mutations have been identified related to TTR-FAP and degeneration.78910 The most-common TTR-FAP cases are linked with the replacement of valine by methionine at position 30 of the TTR protein (V30M).71112
Liver transplantation has been considered as the primary option for patients with TTR-FAP, which replaces the main source of the variant TTR protein with a normal donor organ to halt the progression of neuropathy in well-selected patients with mild hereditary TTR-FAP, and achieves an acceptable 20-year survival rate of more than 50% despite multiple disadvantages.1314 However, as an invasive treatment, liver transplantation is also accompanied by high perioperative mortality and morbidity even when chronic immunosuppressive treatment is applied.1516 Additionally, in spite of a higher survival rate for early-onset V30M TTR-FAP patients, poor responses in late-onset V30M TTR-FAP and non-V30M TTR-gene-mutant patients have been reported.1417
Given this limitation, a noninvasive therapy with superior medication safety and curative effect is urgently needed.
Tafamidis is an orally administered amyloid fibrils inhibitor that can potently occupy thyroxine-binding sites and stabilize tetramers with high specificity, and is the first approved disease-modifying medicine for treating TTR-FAP.18 Many recent researches have focused on the efficacy and safety of tafamidis in TTR-FAP patients from diverse populations and regions. Tafamidis is emerging as a first-line medicine option to replace liver transplantation.19202122
The present study is the first systematic literature review and meta-analysis performed to evaluate the efficacy and safety of tafamidis in TTR-FAP patients, with the aim of improving the medical-evidence base for applying it as a treatment option for TTP-FAP.
METHODS
Search strategy
This systematic literature review and meta-analysis were performed using the methodology suggested by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. A systematic search of the English-language literature was performed through to May 31, 2018 in the following databases: MEDLINE, PubMed, Embase, Web of Science, and Cochrane Library. The following keywords used were: “tafamidis,” “transthyretin familial amyloid polyneuropathy,” “TTR-FAP,” “V30MTTR,” “nonV30MTTR,” “randomized,” and “randomly.” These keywords were combined with appropriate Boolean operators, and further relevant articles were searched for by also checking the reference lists of all of the identified publications. After completing the literature searches, the titles and abstracts of the study reports were screened by Z.Y.N. and X.Y.G., and any disagreement was resolved by discussion with or (if necessary) adjudication by H.W.Y.
Selection criteria
The following inclusion criteria were applied in the present systematic review and meta-analysis: 1) a randomized, placebo-controlled trial (RCT) with at least 12 months of follow-up, 2) patients diagnosed with TTR-FAP, and 3) studies that compared the effects of 20 mg of tafamidis self-administered once daily as a 1:1 meglumine salt or matching placebo. Studies with the following characteristics were considered ineligible: 1) studies that did not include outcomes information, 2) case reports or studies for which insufficient information was provided about the patients, and 3) studies without sufficient data to allow the incidence of mortality or other outcomes to be determined.
Endpoints
Primary endpoints
Primary efficacy analyses were performed to assess the efficacy of tafamidis, including changes from baseline in the Neuropathy Impairment Score–Lower Limbs (NIS-LL) and the Norfolk Quality of Life-Diabetic Neuropathy total quality of life (TQOL) score. The NIS-LL quantifies the motor and reflex functions in the lower limbs to assessing the disease severity in TTR-FAP.2324 The Norfolk Quality of Life scale utilizes a patient-reported questionnaire that provides a TQOL score ranging from −2 (best) to 138 (worst).25 The efficacy endpoints were obtained before the drug regimen was changed.
Study selection, data extraction, and quality assessment
The following basic information was extracted for each study independently by Z.Y.N. and S.Z.Y. using a standard form: surname of the first author, year of publication, country in which the procedure was performed, study design, group assignment, number of patients and their basic characteristics, follow-up duration, and outcomes (Table 1).
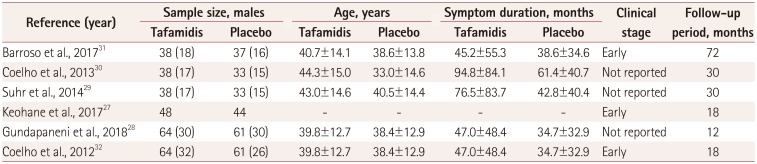
Table 1
Baseline characteristics of the included studies
| Reference (year) | Sample size, males | Age, years | Symptom duration, months | Clinical stage | Follow-up period, months | |||
|---|---|---|---|---|---|---|---|---|
| Tafamidis | Placebo | Tafamidis | Placebo | Tafamidis | Placebo | |||
| Barroso et al., 201731 | 38 (18) | 37 (16) | 40.7±14.1 | 38.6±13.8 | 45.2±55.3 | 38.6±34.6 | Early | 72 |
| Coelho et al., 201330 | 38 (17) | 33 (15) | 44.3±15.0 | 33.0±14.6 | 94.8±84.1 | 61.4±40.7 | Not reported | 30 |
| Suhr et al., 201429 | 38 (17) | 33 (15) | 43.0±14.6 | 40.5±14.4 | 76.5±83.7 | 42.8±40.4 | Not reported | 30 |
| Keohane et al., 201727 | 48 | 44 | - | - | - | - | Early | 18 |
| Gundapaneni et al., 201828 | 64 (30) | 61 (30) | 39.8±12.7 | 38.4±12.9 | 47.0±48.4 | 34.7±32.9 | Not reported | 12 |
| Coelho et al., 201232 | 64 (32) | 61 (26) | 39.8±12.7 | 38.4±12.9 | 47.0±48.4 | 34.7±32.9 | Early | 18 |
![]()
The modified Jadad quality scoring scale evaluates various parameters such as the generation of random sequences, distribution methods, randomized concealment, and whether a blind method was adopted.26 The total Jadad score ranges from 0 to 7; 1–3 points for a low-quality study and 4–7 points for a high-quality study. Two raters performed the quality assessment independently (Z.Y.N. and X.Y.G.), with disagreements resolved by seeking the opinion of the third rater (H.W.Y.) (Table 2). Publication bias was evaluated using Egger's regression test, and Begg's adjusted rank correlation test (Table 3).

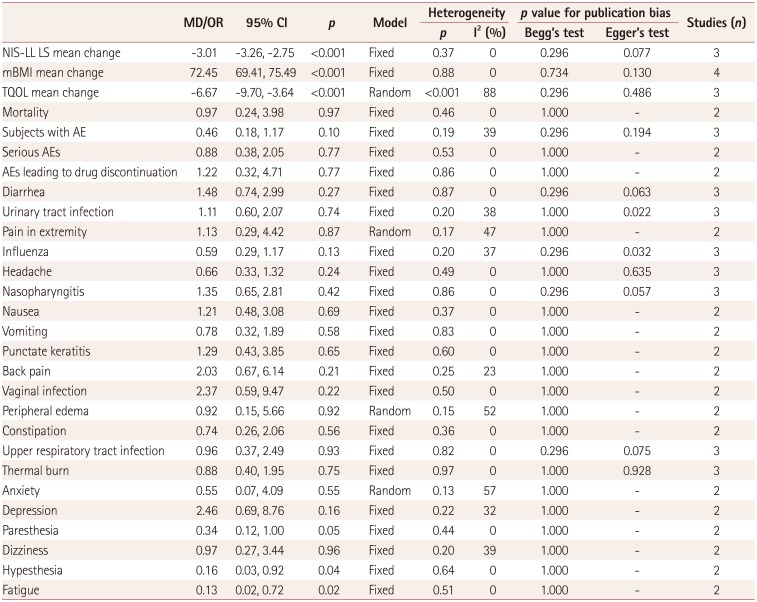
Table 2
Jadad scores for the included studies
| Reference (year) | Randomization | Concealment of allocation | Double blinding | Withdrawals and dropouts | Jadad score |
|---|---|---|---|---|---|
| Barroso et al., 201731 | 2 | 1 | 2 | 1 | 6 |
| Coelho et al., 201330 | 2 | 1 | 2 | 1 | 6 |
| Suhr et al., 201429 | 2 | 1 | 2 | 1 | 6 |
| Keohane et al., 201727 | 2 | 1 | 2 | 1 | 6 |
| Gundapaneni et al., 201828 | 2 | 1 | 2 | 1 | 6 |
| Coelho et al., 201232 | 2 | 1 | 2 | 1 | 6 |
![]()
Table 3
Results from the meta-analysis of various outcomes and publication bias
![]()
Statistical analysis
The statistical analysis was performed independently by X.Y.G. and H.W.Y. according to recommendations from the PRISMA statement and the Cochrane handbook from the Cochrane Collaboration. The pooled mean difference (MD) or odds ratio (OR) with 95% confidence intervals (CIs) were calculated for each principal dichotomous variable outcome. Cochrane's Q-test and I-squared (I2) were used to evaluate the statistical heterogeneity for the pooled results. The combined result was regarded as having heterogeneity if p<0.05 or I2>50%. A fixed-effect model was used to conduct a meta-analysis when the data showed inconspicuous heterogeneity, otherwise a random-effect model was applied. Subgroup analysis was also conducted in our meta-analysis.
The meta-analysis was performed using RevMan software (version 5.3, Cochrane Collaboration; Copenhagen, Denmark). The presence of publication bias was assessed with Egger's regression test and Begg's adjusted rank correlation test using the meta bias commands in STATA (version 14.0, StataCorp, College Station, TX, USA). All of the statistical tests were two-sided, and p<0.05 was considered statistically significant.
RESULTS
Literature selection
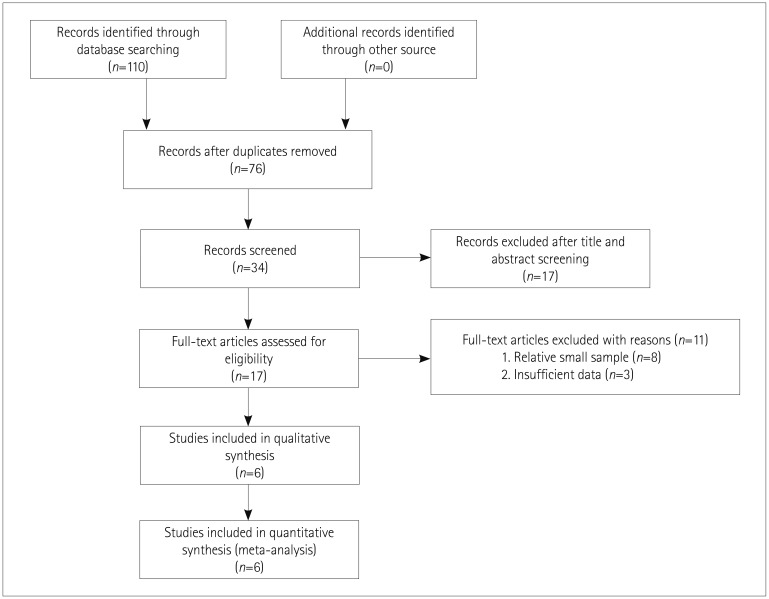
The database searches yielded 110 entries, of which 76 were excluded due to duplications, reviews, or irrelevance. Of the 34 publications that qualified for abstract review, 17 were dropped for the following reasons: only a single treatment arm (n=3), comparison of the effect of tafamidis on TTR-FAP between different TTR gene mutations (n=2), follow-up duration of less than 1 year (n=1), lack of clarity of the NIS-LL or Norfolk Quality of Life score (n=3), treatment regimens in the control group not in accordance with our inclusion criteria (n=8). Full-text articles were assessed for the remaining 17 publications, and 11 were excluded with the following reasons: sample too small (n=8) or insufficient data (n=3). We therefore finally enrolled six trials for further analysis. The PRISMA flow diagram for study selection is shown in Fig. 1.
Efficacy endpoints
Co-primary endpoints
The NIS-LL and the least-squares (LS) mean changes in the NIS-LL from the baseline to the endpoint levels were reported for three of the included studies.272831 The overall meta-analysis revealed a statistically significant difference, with an MD of −3.01 in the LS mean change between the tafamidis and placebo groups, with no significant heterogeneity (95% CI=−3.26 to −2.75, p<0.001, I2=0%) (Fig. 2, Table 3, Supplementary Fig. 1 in the online-only Data Supplement).
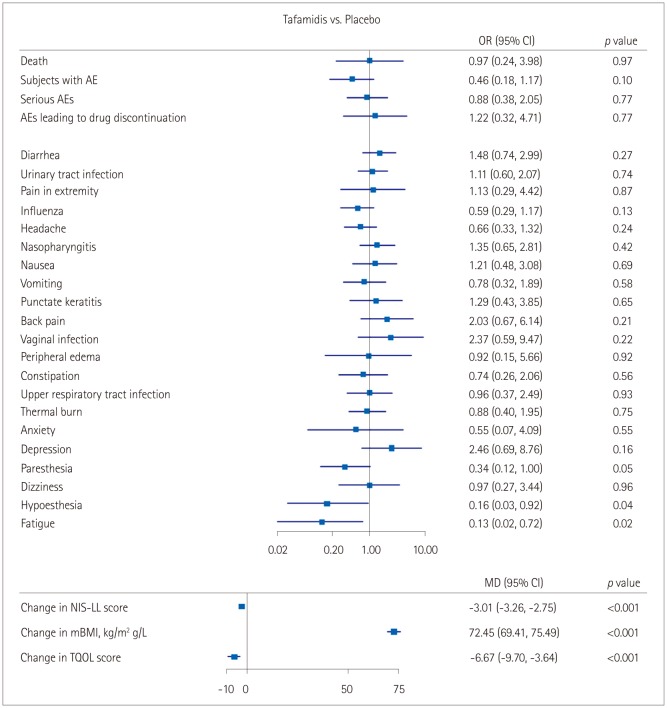
The LS mean change from the baseline in the Norfolk Quality of Life-Diabetic Neuropathy TQOL score to the endpoint level was reported for three of the included studies.273132 The overall meta-analysis revealed a statistically significant difference, with an MD of −6.67 in the LS mean change between the tafamidis and placebo groups, with a significant heterogeneity (95% CI=−9.70 to −3.64, p<0.001, I2=88%) (Fig. 2, Table 3, Supplementary Fig. 1 in the online-only Data Supplement).
Secondary endpoint
The change in mBMI was taken as the secondary endpoint for evaluating the nutritional status in the tafamidis and placebo groups, and four studies were included.27293132 The overall meta-analysis revealed a statistically significant difference, with an MD of 72.45 for the mBMI change between the tafamidis and placebo groups (95% CI=69.41 to 75.49, p<0.001, I2=0%) (Fig. 2, Table 3, Supplementary Fig. 1 in the online-only Data Supplement).
Safety endpoints
Adverse events were reported in detail for three studies.303132 The proportion of patients reporting adverse events did not differ between the groups: 132 (89.8%) of the 147 patients in the tafamidis group versus 134 (95%) of the 141 patients in the placebo group (OR=0.46, 95% CI=0.18 to 1.17, p=0.10, I2=39%) (Fig. 2, Table 3, Supplementary Fig. 2 in the online-only Data Supplement). Mortality events were reported for two of the studies.3132 The proportion of such events did not differ between the groups (OR=0.97, 95% CI=0.24 to 3.98, p=0.97, I2=0%) (Fig. 2, Table 3, Supplementary Fig. 2 in the online-only Data Supplement).
Subgroup analyses showed that most-common adverse events did not differ between the tafamidis and placebo groups (Fig. 2, Table 3, Supplementary Fig. 2 in the online-only Data Supplement). However, the proportion of patients reporting fatigue differed significantly between the two groups: 1 (0.01%) of the 103 patients in the tafamidis group versus 10 (10%) of the 100 patients in the placebo group (OR=0.13, 95% CI=0.02 to 0.72, p=0.02, I2=0%) (Fig. 2, Table 3, Supplementary Fig. 2 in the online-only Data Supplement). The proportion of patients reporting hypesthesia also differed significantly between the groups: 1 (0.01%) of the 103 patients in the tafamidis group versus 8 (8%) of the 100 patients in the placebo group (OR=0.16, 95% CI=0.03 to 0.92, p=0.04, I2=0%) (Fig. 2, Table 3, Supplementary Fig. 2 in the online-only Data Supplement).
Quality and publication bias of the included studies
The quality of the included studies was quantitatively assessed using the Jadad scale. All six included studies employed randomization, concealment of allocation, and double blinding, and all of them had a Jadad score of 6 points, indicating that they were of high quality (Table 2).272829303132 Publication bias was tested using Egger's regression test and Begg's adjusted rank correlation test, and we found no significant correlation between effect size or other evidence of publication bias (Table 3).
DISCUSSION
We collected six double-blind RCTs that included patients with TTR-FAP to evaluate the efficacy and safety of tafamidis. The pooled results demonstrated the following: 1) tafamidis treatment achieved a significantly better result than placebo treatment in terms of the LS mean changes from the baseline in the NIS-LL, TQOL score, and mBMI, and 2) the incidence rates of adverse events were similar in the tafamidis and placebo treatment groups. Although subgroup analysis revealed that the most-common adverse events did not differ between the tafamidis and placebo groups, the risk of hypesthesia and fatigue were significantly lower in the tafamidis group than in the placebo treatment group of patients with TTR-FAP.
A previous study found that tafamidis treatment did not affect patients with TTR amyloid cardiomyopathy.33 However, a recent multicenter, international, double-blind, placebo-controlled, phase 3 trial involving 441 patients with TTR amyloid cardiomyopathy randomly assigned to a tafamidis or placebo group for 30 months found that tafamidis was associated with reductions in all-cause mortality, cardiovascular-related hospitalizations, and the declines in functional capacity and quality of life as compared with placebo.34 This represents strong evidence that tafamidis is an effective therapy for patients with TTR amyloid cardiomyopathy.
In addition to clinical studies of the effect of tafamidis on TTR-FAP patients, several trials have examined the roles of a kinetic stabilizer (diflunisal) on TTR-FAP disease progression.353637 Diflunisal is a generic nonsteroidal anti-inflammatory drug that has been successfully complexed to the thyroxine binding site, and it has been demonstrated to kinetically stabilize circulating TTR protein tetramers, thereby inhibiting the release of the TTR protein monomer necessary for amyloidogenesis.3839 These findings represent strong clinical evidence that kinetically stabilizing an amyloidogenic precursor protein (transthyretin) exerts beneficial effects on amyloid-related neurologic disease progression.
TTR gene silencing therapies that inhibit the hepatic production of the mutant and nonmutant TTR proteins via posttranscriptional gene silencing have recently received considerable attention in explorations of invasive treatments. Antisense oligonucleotides are synthetic strings of nucleotides designed to prevent the expression of a targeted protein by selectively binding to the RNA that encodes the targeted protein and thereby prevent translation. It was reported very recently that inotersen, a 2′-O-methoxyethyl-modified antisense oligonucleotide that inhibits hepatic production of TTR, improves the course of neurologic disease and the quality of life in patients with hereditary TTR amyloidosis. The limitations of this clinical trial included that it had insufficient statistical power for measuring the effects of inotersen treatment on cardiomyopathy.40 ISIS-TTRRX is a second-generation antisense inhibitor of the molecular target TTR, and is designed to bind within the nontranslated portion of the human TTR gene messenger RNA (mRNA) and thereby degrade this mRNA to prevent the production of both nonmutant and mutant TTR proteins.41
RNA interference (RNAi) therapy has also been used to suppress the production of TTR.42 RNAi is an endogenous cellular mechanism for controlling gene expression in which small interfering RNAs that are bound to the RNA-induced silencing complex mediate the cleavage of target mRNA.4344 RNAi-based drugs harness endogenous posttranscriptional gene silencing pathways for therapeutic purposes. Two RNAi drugs (ALN-TTR02 and ALN-TTRsc) have been developed that target the disease-causing mutant TTR gene mRNA in the liver for treating TTR-FAP. A greater efficacy in targeting the disease-causing mutant combined with lower risk and better toleration are expected for RNAi-based drugs targeting TTR-FAP. Patisiran is another investigational RNAi therapeutic agent, which specifically inhibits the hepatic synthesis of TTR. A recent randomized, placebo-controlled, phase 3 trial involving patients with hereditary TTR amyloidosis with polyneuropathy found that patisiran improved multiple clinical manifestations of hereditary TTR amyloidosis.45 That trial also yielded evidence that patisiran improved the cardiac manifestations of hereditary transthyretin amyloidosis. We also anticipate that RNAi-based drugs will be widely used for other hereditary diseases in the future. However, no previous clinical trial has compared the efficacy and safety between tafamidis and RNAi drugs for TTR-FAP patients. We therefore also look forward to such clinical studies, which could yield strong evidence of useful treatment options for TTR-FAP patients.
While the present study included six high-quality RCTs, it was also subject to some limitations. Firstly, because this meta-analysis focused on a rare disease, the statistical power was unavoidable restricted by the relative smallness of the sample of existing studies. Secondly, most of the included studies had both a prospective and open-label design, resulting in missing data and a possibility of bias. Thirdly, the inherent limitations of a meta-analysis such as publication bias cannot be ignored. Fourthly, the statistical heterogeneity was quantified for the outcome of TQOL mean changes. The heterogeneity of indicators of continuous variables is generally quite difficult to investigate. Due to a very small number of reports on TQOL mean changes and the different sample sizes and selection criteria applied in the studies, we were unable to conduct a subgroup analysis. Moreover, our sensitivity analysis (Supplementary Fig. 3 in the online-only Data Supplement) failed to identify the real sources of the heterogeneity. We speculate that the heterogeneity was caused by multiple factors such as age, sex, disease course, and treatment time.
In conclusion, this systematic review and meta-analysis of six RCTs has demonstrated that tafamidis exhibits a slower neurologic disease progression and better preservation of nutritional status and quality of life.
The rate of adverse events did not differ between the patients in the tafamidis and placebo groups. These findings indicate that tafamidis might be a safer noninvasive option for patients with TTR-FAP.
 XML Download
XML Download